Effectiveness of Curry-Leaf Mouthwash in Maintaining Salivary and Tongue pH as Compared to Chlorhexidine Mouthwash: A Randomised Controlled Trial
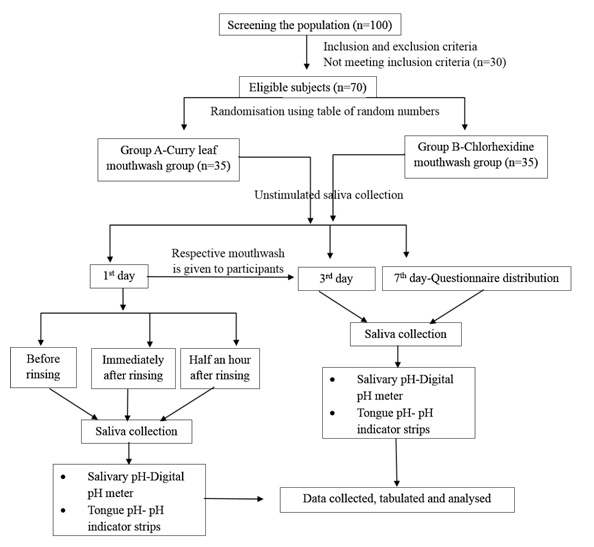
<p style="text-align: justify;">Background: Saliva plays a critical role in maintaining oral health through various defensive mechanism and salivary pH is a fair indicator of various dental diseases. A lot of synthetic salivary pH stabilising agents are available but they have undesirable side effects. Therefore there is a need for the search of alternate products. One of those agents is curry leaf (Murraya koenigii), which is easily available and has no adverse effects. Aim: The purpose of the study was to evaluate effectiveness of curry leaf mouthwash in maintaining salivary and tongue pH as compared to chlorhexidine mouthwash. Methodology: A randomized parallel-group study was conducted among 70 participants who were randomly allocated to two groups. (35 participants in curry leaf and chlorhexidine mouthwash group). Stimulated saliva was collected on 1st, 3rd and 7th day and at three time intervals on 1st day. After this, salivary and tongue coating pH were measured by a digital pH meter and coloured pH indicators. A questionnaire was distributed to the participants on the last day related to the use of two mouthwashes. Data were analyzed statistically using chi-square, independent t test and paired t test. Results: There was no statistically significant difference between the two groups in relation to salivary and tongue pH. Mean salivary pH difference was found statistically significant within both the groups and mean tongue pH difference was found significant only within curry leaf mouthwash group at 2 point intervals (immediately and half an hour after rinsing). Conclusion: Traditional curry leaf mouthwash can be considered as safe, effective, and economical agent and as an alternative to the commercially available mouthwash.</p>
Introduction
Oral diseases starting from cavities to cancer are recognized as major public health problems throughout the world. Among them, the most common one is dental caries. It is an infectious microbiologic disease of the tooth with multifactorial aetiology and factors. One of the recognized and contributing factors for the causation or prevention of dental caries is saliva. The defensive system of saliva includes salivary pH, buffering capacity, salivary flow etc [1]. Salivary pH is of great relevance to oral cavity more specifically to dental caries as many of the pathological conditions are strongly dependant on the pH changes [2]. Salivary pH ranges from 6.2-7.4 and the drop of salivary pH beyond the critical pH creates favourable environment for acidophilic microorganisms such as Streptococcus mutans and Lactobacilli, and subsequently start of the caries process by demineralization of the dental enamel [3]. A lot of commercial agents are available in the market for improving the oral health of the individual by stabilizing the salivary pH through anti-cariogenic effects of the agents, but they also have several undesirable side effects such as allergic reactions, vomiting, diarrhoea, and tooth staining [4]. In order to overcome these side effects, World Health Organization (WHO) has advised to incorporate natural products as an alternate to these commercial agents as they are safe, effective and economical. Almost 25 centuries ago Hippocrates, the father of Medicine, proclaimed “let food be thy medicine and medicine be thy food” [5]. Since many years “Danta- shastra’ was being practised in our country. It is a term used for utilizing the natural products ranging from chewing sticks till herbal mouthwashes for the maintenance of healthy teeth [6]. Among those natural food products, one of them is extremely popular ingredient of Indian cuisine and is used in every home to give flavor and aroma to most of the recipes, it is known as curry leaf (Murraya koenigii; Rutaceae) or “Magical plant of Indian Spice”. The official name of curry leaf in India is Saurabhanimba. The plant has a monography at the Ayurvedic Pharmacopoeia of India. It is a green leafy vegetable which is easily available, commonly known as Kurrypatte or meethi neem [7]. It has various systemic and oral benefits and can be used in many forms- fresh raw leaves, paste, dried or powdered leaves and mouthwash. Green leaves are eaten raw for cure of dysentery, diarrhoea and vomiting. They also act as anthelmintic, analgesic and can be used for curing piles, inflammation, itching, leucoderma and blood disorders [8, 9]. They are also used as calcium source to those having calcium deficiency and are rich source of Vitamin A, Vitamin B and B2, Vitamin C, iron, carbohydrates, proteins, amino acids and minerals [10]. The fresh curry leaves contain 2.65% volatile essential oils like sesquiterpenes and monoterpenes which have broad anti-microbial effects [11]. Chowdhury, et al. (2001) reported that alkaloids present in curry leaf have antimicrobial activity against gram positive and negative bacteria and fungi [12]. Curry leaf also contains chlorophyll, which was thought to be the anticariogenic agent and reduces halitosis [11]. Few studies related to curry leaf were conducted in past but no study has compared the effects of curry leaf mouthwash with a commercial available mouthwash [13, 14]. Therefore there is a need to evaluate the effectiveness of curry leaf mouthwash on salivary and tongue coating pH and its comparison with the gold standard mouthwash i.e., the 0.2% chlorhexidine gluconate mouthwash.
Materials and Methods
Study Design
A randomized controlled trial consisting of parallel groups (curry leaf mouthwash group and chlorhexidine group) was conducted to assess the effectiveness of curry leaf mouthwash on salivary and tongue pH as compared to gold standard chlorhexidine mouthwash.
Study Population, Duration and Setting
College students aged 18-24 years of Bangalore City, without the history of systemic diseases and antibiotics are included in the study. The study was carried out from September 2016 to October 2016 in a dental college and the study duration was one week.
Ethical Approval
The study protocol was reviewed by the Ethical committee of Institutional Review Board and was granted ethical clearance Journal of Natural & Ayurvedic Medicine
+𝒁𝟏−𝜷)𝟐𝝈𝟐 (𝒓+𝟏)(𝒁∝
𝟐 Sample size: 𝑁=
𝒓𝒅𝟐 𝑛1 r = 𝑛2 is the ratio of sample size required for 2 groups = 1
∝ Z
2 = is the normal deviate at a level of significance=1.96 Z1-𝛽= is the normal deviate at 1-𝛽% power with 𝛽% of type II error= 1.28 𝜎 = pooled standard deviation=4 d = difference of means of 2 groups=2.2 Final sample size was 70 students. The study protocol was described to the students and then consent form was distributed. Seventy college students aged 18 years and above and who signed the informed consent form, were included in the study. After the inclusion of the participants in the study, randomization of the students to their respective groups was done using table of random numbers (35 students in each group) by a different investigator.
Preparation of Mouthwash
Percent Curry Leaves Mouthwash:
- Fresh curry leaves was obtained and an aqueous extract was prepared by using 100 g of fresh curry leaves and 100 ml of distilled water, all of which were processed in an electric mixer for 10 minutes.
- The resulting extract was filtered and sterilised by paper filter.
- All solid and liquid residues were weighed and attained a concentration of 25%. (250gm of curry leaves paste in 1000 ml or 1 litre).
- It was again diluted with distilled water to attain a final concentration of 2.5% [14].
Collection of Saliva
On the day of study, the participants were asked to perform their normal oral hygiene procedure, but refrain from eating or drinking up to one hour prior to saliva collection. Participants were seated comfortably in a dental chair and were instructed to bend the head forward to collect stimulated saliva into a paper cup with the help of chewable rubber bands.
Journal of Natural & Ayurvedic Medicine
Saliva collection was done on three days over a period of one week (1st day, 3rd day and 7th day) and on first day at three time intervals (Before rinsing, immediately after rinsing and half an hour after rinsing). Stimulated saliva was collected by the investigator on the 1st day before rinsing with the respective mouthwash and then tongue coating pH was recorded with the help of pH strips. The participants were then asked to rinse the mouth with the respective mouthwashes (10 ml for 1 minute) and then again saliva was collected and tongue pH was recorded. After half an hour of rinsing, same procedure was repeated for the salivary pH and tongue pH assessment. None were allowed to eat or drink during the phases. Mouthwashes were handed over to the students for 7 days as per group respectively (10 ml mouthwash, twice daily for 1 minute). Salivary samples were collected on 3rdand 7thday and estimation of salivary and tongue pH was done. Salivary pH was assessed using digital salivary pH meter and tongue pH with the help of pH indicator strips (pH 0-14).
Questionnaire
On 7th day, a questionnaire was distributed to all the
Mean salivary pH
participants and all of them were questioned about mouthwash taste, breath alteration, burning sensation, tooth colour alteration and systemic adverse effects. The questionnaire was in English language, self-administered and previously validated [14, 15].
Statistical Analysis
The Statistical software Statistical Package for Social Science (SPSS) version 22.0 was used for the analysis of the data and Microsoft Excel have been used to generate graphs, tables etc. Descriptive statistics with frequency and percentage was obtained. Independent t test, paired t test and chi-square test were applied. The p value was taken as significant when less than 0.05.
Results
Seventy (100%) college students of age 18 years and above were included in the study with a mean (± S.D.) age of 20.46 (± 2.16) years. Fifty three (75.7%) of them were females and 17 (24.3%) were males.
| mmeenhda 7.67 | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 7.62 | 7.61 7.6 7.59 | |||||||||||||||||
| 7.56 | 7.56 7.54 | |||||||||||||||||
| 7.49 | ||||||||||||||||||
| 7.43 | ||||||||||||||||||
Journal of Natural & Ayurvedic Medicine
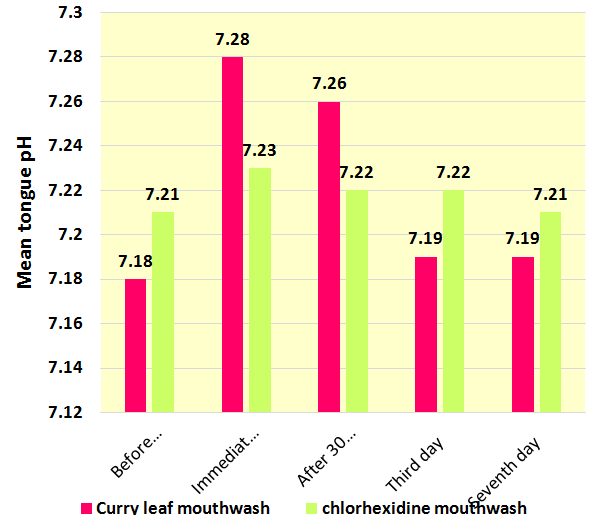
Mean salivary pH was compared between curry leaf mouthwash group and chlorhexidine mouthwash group at different time intervals within one week. There was no significant difference found between both the groups (p>0.05) (Figure2).
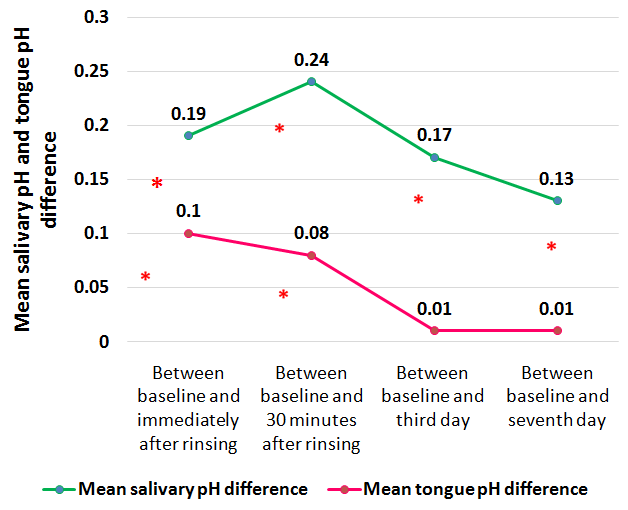
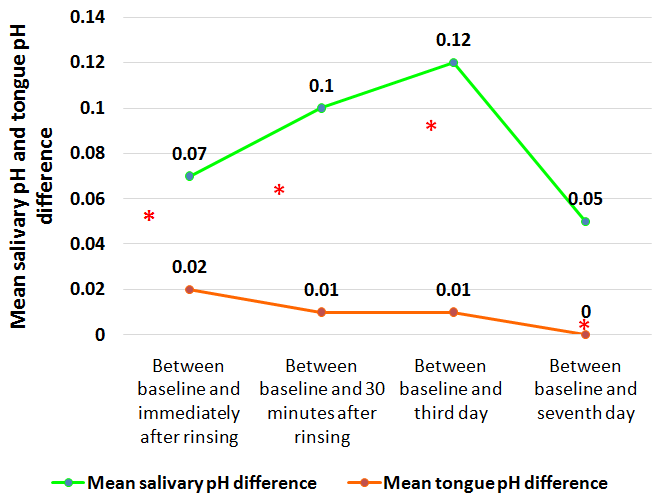
(Paired t test, *denotes statistical significance) Figure 4: Comparison of mean salivary pH difference and mean tongue pH difference at different point intervals within curry leaf mouthwash group.
Journal of Natural & Ayurvedic Medicine
Mean salivary pH and tongue difference was calculated by comparing the mean pH of various intervals with the baseline pH to evaluate the deviation from the mean pH at various points of study intervals in curry leaf mouthwash group. Mean salivary pH was found significant at all the point intervals (p<0.05), whereas mean tongue pH difference was found significant only between baseline and immediately after rinsing and between baseline and half an hour after rinsing with the curry leaf mouthwash (p<0.05) (Figure 4).
included in the questionnaire (alteration in taste, breath, tooth colour, burning sensation and systemic adverse effects) (Table 1).
| Question | Group | Low | Moderate | Serious | Severe | |
| Alteration in taste | Curry leaf mouthwash | 10(28.5%) | 14(40%) | 11(31.5%) | 0 | 0 |
| Alteration in taste | Chlorhexidine mouthwash | 27(77.1%) | 8(22.9%) | 0 | 0 | 0 |
| Alteration in breath | Curry leaf mouthwash | 9(25.7%) | 22(62.9%) | 4(11.4%) | 0 | 0 |
| Alteration in breath | Chlorhexidine mouthwash | 21(60%) | 14(40%) | 0 | 0 | 0 |
| Burning sensation | Curry leaf mouthwash | 14(40%) | 19(54.3%) | 2(5.7%) | 0 | 0 |
| Burning sensation | Chlorhexidine mouthwash | 24(68.5%) | 11(31.4%) | 0 | 0 | 0 |
| Alteration in tooth color | Curry leaf mouthwash | 12(34.3%) | 14(40%) | 9(25.7%) | 0 | 0 |
| Alteration in tooth color | Chlorhexidine mouthwash | 28(80%) | 7(20%) | 0 | 0 | 0 |
| Systemic effects | Curry leaf mouthwash | 35(100%) | 0 | 0 | 0 | 0 |
| Systemic effects | Chlorhexidine mouthwash | 35(100%) | 0 | 0 | 0 | 0 |
Table 2: Response of participants towards the two mouthwashes Table 1: Response of participants towards the two mouthwashes Journ
Discussion
Dental diseases are highly prevalent in developing countries due to negligence, lack of awareness and scarcity of treatment as dental care services are often too costly and totally absent in the rural areas and concentrated mainly in urban areas. So, there is a great demand for alternate methods of prevention of dental diseases that are natural, safe, economical and effective. One such method used in this study was curry leaf in mouthwash form as mouthwashes are widely used nowadays and gaining attention in the market because of their easy to use method and the presence of active ingredients [16]. In the present study, two varieties of mouthwashes were taken, one was natural and the other was synthetic. First was curry leaf mouthwash (2.5%) and the other was chlorhexidine mouthwash (0.2%). Curry leaf or Murraya Koenigii, that belongs to Family Rutaceae is a very popular plant for its characteristic aroma and medicinal value. According to Math MV, chewing 2 to 4 fresh curry leaves with 10 to 15mls water, swishing for 5 to 7 minutes and then rinsing the mouth with water is very helpful in maintaining good oral hygiene [11]. This method was same as using mouthwash. The other mouthwash used was chlorhexidine mouthwash (0.2%). Chlorhexidine is considered as the ‘gold standard’ mouthwash. It also has evidence related to be used as anti-caries and anti-plaque agent but also has some side effects such as alteration of taste, tooth staining and desquamation of the oral mucosa [17]. Chlorhexidine mouthwash was available in two concentrations (0.12% and 0.2%). Carlos Alfredo Franco Neto, et al. stated that there is no difference in the efficacy of chlorhexidine between 0.12 to 0.2% hence, in the present study, 0.2% concentration of chlorhexidine mouthwash was used [18]. The present study was a parallel group randomised controlled trial using two different types of mouthwash. The outcome variables were mean salivary pH and mean tongue pH compared between and within both the groups at different point intervals of the study. The mean salivary pH and tongue pH was compared at different time intervals of the study between both the groups and it was found non-significant between both the groups, it implies that both the mouthwash did not have much difference regarding alteration in salivary and tongue pH. The results of our study are in contrary to a study conducted by Ramesh G, et al, in which a significant difference was observed between the three groups (curry leaf, mint leaf and tulsi leaf group) (p < 0.05) and also between the tulsi and curry leaf groups on the last assessment or final day with respect to mean tongue pH (p < 0.05) [13]. Mean salivary pH difference was compared within both the mouthwashes group and it was found significant at all the point intervals of the study. The results are in accordance with the study conducted by Ramesh G, et al. in which mean salivary pH difference between baseline and further intervals was found significant (p<0.05) within curry leaf mouthwash group [13]. Same results were obtained by Ashwini Y, et al. in which 0.2% chlorhexidine mouthwash was compared with neem and green tea mouthwash and the salivary pH was significant within the chlorhexidine group [19]. The increased value of mean salivary pH was found immediately after rinsing and 30 minutes after rinsing in both the groups. This can be explained by the fact that rinsing mouth with the mouthwash may increase salivary flow and in turn stimulates salivation which increases the saliva’s bicarbonate concentration and thus increases salivary pH [20]. Increased salivary pH has a lot of benefits in maintaining oral health as increased salivary pH actively reduces demineralisation and increases remineralisation of the enamel crystals damaged by an acid attack and in turn less probabilities of dental decay. In the present study, stimulated saliva was used to measure salivary pH. Stimulated saliva contains more calcium and bicarbonate and has a higher pH than unstimulated saliva, making it even more effective at remineralizing the enamel crystals. The mean tongue pH difference was found significant only at two point intervals (between baseline and immediately after rinsing and between baseline and 30 minutes after rinsing) in curry leaf mouthwash group whereas, non-significant in chlorhexidine mouthwash group. Tongue pH is a major indicating factor for the bad breath forming elements as increased tongue pH or alkalinity favours the production of odours while acidity or decreased tongue pH inhibit the production of such substances [21]. Bad breath forming elements that contributes to the alkalinity of tongue pH and hence halitosis includes odorivetores, which are the final products of proteolysis such as amines, ammonia, and urea [20].
Journal of Natural & Ayurvedic Medicine
On the last assessment day, participants of both the groups were asked to fill a questionnaire. There were five questions regarding taste, alteration in tooth colour, burning sensation etc. because of any of the two mouthwashes. Regarding alteration in taste, alteration in colour and burning sensation, maximum participants in the curry leaf mouthwash group answered that they observed slight alteration while in the chlorhexidine mouthwash group, majority of them reported that there was no alteration. Contradictory results were obtained by Prabhakar AR, et al. in which majority of the participants in the curry leaf mouthwash group (55.6%) reported no alteration in taste and breath and in a study conducted by Gupta D et al, subjects in the chlorhexidine group noticed slight alteration in taste [15]. Regarding burning sensation similar results were obtained in a study conducted by Prabhakar AR, et al. in which majority of the participants in the curry leaf mouthwash group (55.6%) reported low-moderate symptoms of burning sensation [14]. When the participants were asked about any symptoms of systemic effects because of any of the mouthwash, all the participants (100%) in both the groups reported no symptoms of any systemic effects. Same results were obtained by Prabhakar AR, et al. study, in which all the participants in the curry leaf mouthwash group (100%) reported no symptoms of any systemic effects [14].
Limitations
Since the sample size of the present study was seventy and the study duration was only 1 week, more studies with larger sample size and with longer duration on curry leaf mouthwash should be encouraged to assess the long term effectiveness.
Conclusion
In the present study, there was no significance regarding mean salivary pH and mean tongue pH between both the mouthwash groups. Within the curry leaf mouthwash group, mean salivary pH and mean tongue pH difference was found significant at various point intervals and within chlorhexidine mouthwash group, mean salivary pH difference was found significant only at two point intervals and non-significant with respect to mean tongue pH difference. Acknowledgement: The authors would like to thank the participants of the study for their kind cooperation throughout the study.
References
-
Van Nieuw Amerongen A, Bolscher JG, Veerman EC (2004) Salivary proteins: protective and diagnostic value in cardiology. Caries Res 38(3): 247-253.
-
Humphrey SP, Williamson RT (2001) A review of saliva: Normal composition, flow, and function. J Prosthet Dent 85(2): 162-169.
-
Lingstrom P, Van Ruyven FO, Van Houte J, Kent R (2000) The pH of dental plaque in its relation to early enamel caries and dental plaque flora in humans. J Dent Res 79(2): 770-777.
-
Chung JY, Choo JH, Lee MH, Hwang JK (2006) Anticariogenic activity of macelignan isolated from Myristica fragrans (nutmeg) against Streptococcus mutans. Phytomedicine 13(4): 261-266.
-
Prasan R Bhandari (2012) Curry leaf (Murraya koenigii) or Cure leaf: Review of its curative properties. Journal of Medical Nutrition and Nutraceuticals 1(2): 92-97.
-
History and Origin of Ayurvedic Medicine.
-
Nayak A, Mandal S, Banerji A, Banerji J (2010) Review on chemistry and pharmacology of Murraya koenigii Spreng (Rutaceae), Journal of Chemical and Pharmaceutical Research 2(2): 286-299.
-
Nadkarni KM (1976) Indian Materia Medica. 3rd (Edn.), Popular Prakashan, Mumbai, pp: 196.
-
Kirtikar KR, Basu BD (1981) Indian Medicinal Plants. 2nd (Edn.), Oriental Enterprises, Uttarchal Pradesh, pp: 473.
-
Nishan M, Subramanian P (2014-2015) Murraya koenigii (curry leave): A review on its potential. Int J Pharm Tech Res 7(4): 566-572.
-
Math MV, Balasubramaniam P (2004) Curry leaves. Br Dent J 197(9): 519.
-
Chowdhury BK, Jha S, Bhattacharyya P, Mukherjee J (2001) Two new carbazole alkaloids from Murraya koenigii. Indian Jour Chem 40B(6): 490-494.
-
Ramesh G, Nagarajappa R, AS Madhusudan, Sandesh N, Batra M, et al. (2012) Estimation of salivary and tongue coating pH on chewing household herbal Journal of Natural & Ayurvedic Medicine leaves: A randomized controlled trial. Anc Sci Life 32 (2): 69-75.
-
Prabhakar AR, Ahuja V, Basappa N (2009) Effect of Curry Leaves, Garlic and Tea Tree Oil on Streptococcus Mutans and Lactobacilli in Children: A Clinical and Microbiological Study. Pesq Bras Odontoped Clin Integr 9(3): 259-263.
-
Gupta D, Bhaskar DJ, Gupta RK, Karim B, Gupta V, et al. (2014) Effect of Terminalia Chebula Extract and chlorhexidine on salivary pH and Periodontal Health: 2 weeks Randomised Control Trial. Phytother Res 28(7): 992-998.
-
Alessandro LC, Ianny AR, Rafaela BL, Oliveira MC, Menezes KM, et al. (2010) Endogenous pH, Titratable acidity and total soluble solid content of mouthwashes available in the Brazilian market. Eur J Dent 4(2): 156-159.
-
Malhotra R, Grover V, Kapoor A, Saxena D (2011) Comparison of the effectiveness of a commercially available herbal mouth rinse with chlorhexidine gluconate at the clinical and patient level. J Indian Soc Periodontol 15(4): 349-352.
-
Franco Neto CA, Parolo CC, Rosing CK, Maltz M (2008) Comparative analysis of the effect of two chlorhexidine mouthrinses on plaque accumulation and gingival bleeding. Braz Oral Res 22(2): 139-144.
-
Balappanavar AY, Sardana V, Singh M (2013) Comparison of the effectiveness of 0.5% tea, 2% neem and 0.2% chlorhexidine mouthwashes on oral health: A randomized control trial. Indian J Dent Res 24(1): 26-36.
-
Kojima K (1985) Clinical studies on the coated tongue. Japanese J Oral Maxilofac Surg 31(7): 1659- 1676.
-
McNamara TF, Alexander JF, Lee M (1972) The role of microorganisms in the production of oral malodor. Oral Surg Oral Med Oral Pathol 34(1): 41-48.
- Management of Ear Keloid with Ksharsutra: A Case Study
- Yoga and Global Sustainability: A Holistic Path to One Earth, One Health
- Autoimmune Diseases in Ayurveda: A Narrative Review with Classical and Modern Perspectives
- Management of Cluster Headache Associated with Pituitary Apophysitis by CERT (Chakrasiddh Energy Release Technique): A Case Report on Energy Rebalancing
- Zygophyllum Geslini Coss : Biochemicals and Antioxidant Activity
- Observations of a Beginner Vaidya