Carica Papaya Root Extract in Management of Urolithiasis
These days urolithiasis is on progressive rise due to increased urinary solute and altered electrolyte biokinetics. In addition change in dietary composite also made the women equally vulnerable for the presentation. Though surgical removal and lithotripsy are measures available for alleviation of uroliths Clinical manifestation, but recurrence is very common posing encumbrance and agonizing discomfort. In present scenario of available various indigenous drug composite, clinical evaluation of Carica papaya root extract 10-25 ml with Piper nigrum 1-3 daily in empty stomach ensure relief of abdominal colic and passage of uroliths per urethra in majority cases with complete absence of uroliths in USG of KUB or in urine and no recurrence on weekly one dose in 2 yrs of post therapy follow up without any adversity.
Avinash Shankar1*, Amresh Shankar2 and Anuradha Shankar3
recurrence on weekly one dose in 2 yrs of post therapy follow up without any adversity.
Keywords: Urolithiasis; Electrolyte Biokinetics; USG; KUB
Introduction
Progressive increase in the incidence of calcium oxalate, phosphate calculi of the upper urinary tract during the 20th century [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14] is due to changed dietary composition posing an increase in urinary solute load, not only due to altered nutrition resulting from use of irrational food constituent, presentation and storage of food remain full of noxious chemical use, which not only generate non dietary constituent but also generate some enzymes inhibitor to compete with various body enzyme intends altered ionic exchange and urine crystallization. In addition recurrent urinary tract infection due to increasing misuse of broad spectrum antibiotics and declined water intake, predispose for urolithiasis due to presence of urea splitting bacteria. In addition carbohydrate rich dietary habit increases urinary calcium and magnesium excretion [15, 16, 17]. Considering the efficacy of therapeutics in vogue and option for surgical removal or lithotripsy is not only a costly affair but also encumbrance due to recurrence. Thus to check recurrence and alleviate presentation and elimination of crystal, check infection, a clinical evaluation of watery extract of Carica papaya root and Piper nigrum berries been done at RA. Hospital & Research Centre, in association with Centre for Indigenous Medicine & Research, Warisaliganj (Nawada) Bihar.
Material & Methods
Patients of urolithiasis and abdominal colic (due to uroliths) attending medical OPD of RA. Hospital & Research Centre, Warisaliganj (Nawada) Bihar during last 3 years were selected and evaluated by Centre for Indigenous medicine & Research for clinical response of watery extract of Carica papaya root with Piper nigrum berries (Figure 1).

Index for Selection of Patients
- Agonising abdominal pain, in the loin, suprapubic region and back.
- Frequency of micturation and gritting sensation
- Any history of passage of crystal per urethra or hematuria
- Any history of surgery or lithotripsy for stone removal.
Selected patients (or parent of the patient) were interrogated, examined and investigated for presence of uroliths i.e, urine for crystals, X-ray, KUB, IVP, USG for KUB to ascertain presence of crystal, its size, location and sequelae.
In addition serum Creatinine, serum calcium, serum uric acid and blood urea been assessed to adjudge the safety profile in terms of hemato, hepato-renal status. All the patients of urolithiasis without consequent adversity affecting renal function been considered for evaluation of clinical efficacy of watery extract of Carica papaya root and Piper nigrum berries in empty stomach daily for 3 months and patients were followed during the therapy to observe the-
- Relief in clinical presentation
- Any adversity
- History of passage of crystal per urethra
- Any disease related sequel While during post therapy follow up for 2 years, patients were observed for-
- Any recurrence of presentation
- Any untoward effects (as long term toxicity).
For the purpose a follow up card been issued to every patient or parent or MSW covering the patients group and been advised to enter all the details or observation by the patient or parent i.e, passage of crystal, blood in urine, agonizing pain during micturation, inability to pass urine or retention of urine with distended bladder. Pre, Post and during the therapy each patient’s renal functions been duly assessed to adjudge the safety profile of the drug.
Based on the Observation Clinical Response was Graded as (Table 1)
| Grades of Clinical Efficacy | Characteristics |
| Grade I | Complete relief of pain in abdomen, absence of crystals in urine and USG with or without history of passing crystal per urethra and without any recurrence and untoward effects. |
| Grade II | Complete relief of pain and other presentation, absence of crystal in USG but presence of crystal Flecks in the urine, without any untoward effect and recurrence during follow up |
| Grade III | Relief of pain with frequent recurrence, dysuria, presence of crystal in the urine but of reduced size no untoward effects |
| Grade IV | No response |
Table 1: Grades of Clinical Efficacy/Characteristics.
Observation
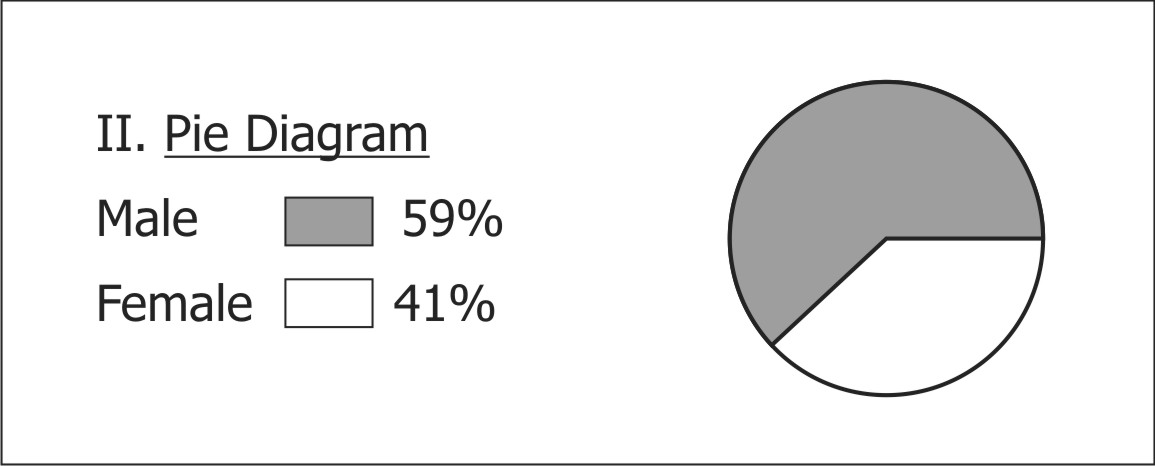
- Among the selected patient 59% were male and 41% female of age group <5yrs-35yrs, 11% patients were of age <5 yrs, 18% of age group 5-10years while 17% cases were of 30-35years (Table 2).
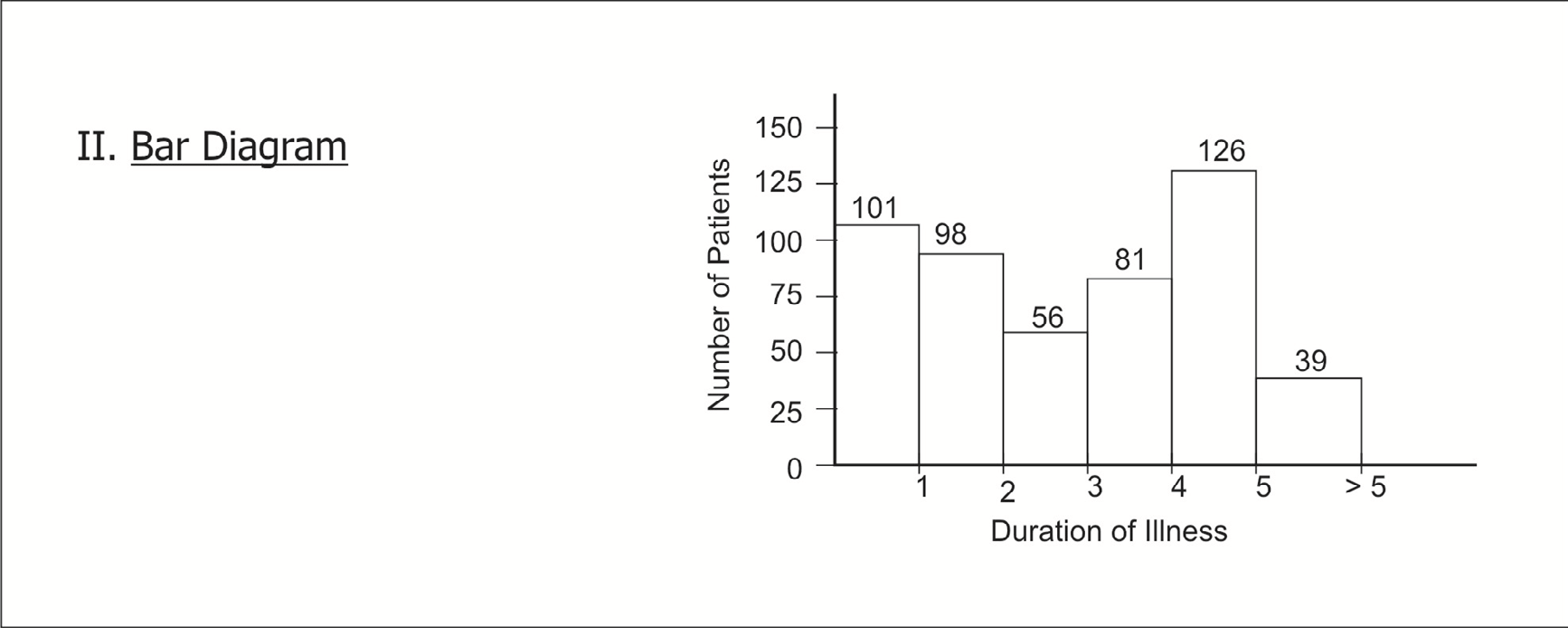
- 20% patients were suffering from <1 year while 8% from >5 years(Bar diagram) (Figures 2 & 3).
- 36% patients had history of passing crystal per urethra, 57% recurrent UTI and 20% with painful hematuria (Tables 4).
- Out of all 56% was newly detected case of uroliths while 13% and 65% were cases of uroliths removal by surgery and lithotripsy respectively (Tables 5).
| Age group | Number of patients | ||||
|---|---|---|---|---|---|
| (Age in Years) | Male | Female | Total | % | |
| < | 5 | 32 | 21 | 53 | 11 |
| 5- | 10 | 52 | 40 | 92 | 18 |
| 10- | 15 | 42 | 30 | 72 | |
| 15- | 20 | 48 | 29 | 77 | |
| 20- | 25 | 38 | 22 | 60 | |
| 25- | 30 | 36 | 24 | 60 | |
| 30- | 35 | 50 | 38 | 88 | 17 |
Table 2: Distribution of Patients as Per Age & Sex.
| Presenting feature | Number of patients | |
|---|---|---|
| Agonizing abdominal pain | 502 | |
| Frequency of micturation | 502 | |
| Gritting sensation during urination | 490 | 98% |
| Retention of urine | 234 | 47% |
| Backache | 282 | 56% |
| Painful micturation | 480 | 96% |
| Passage of uroliths | 182 | 36% |
| Painful hematurea | 98 | 20% |
| Recurrent pyrexia | 288 | 57% |
Table 3: Distribution of Patient as Per Presentation.
| Number of patient | % | |
|---|---|---|
| Newly detected case | 282 | 56 |
| Treated medically with recurrence | 088 | 18 |
| Treated surgically with recurrence | 064 | 13 |
| Lithotripsy with recurrence | 034 | 06.5 |
| On non-conventional measures | 034 | 06.5 |
Table 4: Distribution of Patient as per their Therapeutic Status.
| Particulars | Number of patients |
| Relief in presenting complaint | |
|---|---|
| Complete | 488 |
| Marked | 014 |
| Passage of uroliths per urethra | 403 |
| Ultrasonography for KUB | |
| Absence of crystals | 488 |
| Decline in size of crystal | 014 |
| With desend | |
| Safety profile | |
| Blood urea | 488 |
| Unchanged | 014 |
| Raised | 014 |
| Serum Creatinine | |
| <1.5 mg | 502 |
| >1.5mg | Nil |
Table 5: Outcome of the Study.
Results
- 97% patients had clinical relief within 48 hours of therapy and had complete relief of the presenting feature while 13% had marked improvement in 15 days of therapy.
- 80% patient’s revealed passage of uroliths through urine after 45 days of therapy and after 2 month 97% patient’s USG revealed absence of stone while 3% show marked regression of size and change in site of the stone.
- No patient revealed any alteration in hemato, hepatic and renal function or any other side effects or recurrence of presentation during 2 years of post-therapy follow up.
- 97% patient had Grade I clinical response while 3% Grade II response.
Discussion
In India incidence of urolithiasis varies regionally and in spite of available measures for urolith removal i.e. surgery and lithotripsy [18, 19, 20, 21], recurrence is very rampant due to changed mineral biokinetics due to changing dietary strategy. In addition various indigenous composite formulations are in vogue and possess proved efficacy and no ancient literature affirm the use of common home plant Carica papaya root extract in management of urolithiasis but present study affirms its equipotency with high safety profile and this clinical supremacy can be attributed to [22, 23, 24]. Lithotriptic action of glucohydrolase, butanic acid while cryptoglavin as a potent antibacterial constituent of Carica papaya and Pergunodiene, isopiperolene and trachiene of Piper nigrum, effective against common urinary pathogen Escheresia coliI, Alloxanthine, Cis valloxanthin of Carica papaya acts as a diuretic and help expel the calculi. Musculo relaxant action of Piperin relieves abdominal colic synergized by local anesthetic action of Carpaine. Piperidine acting as an anti- oxidant prevents aggregation of urinary flecks in Urinary path way.
Conclusion
All patients had clinical relief and passage of uroliths without any recurrence and untoward effects thus this must be considered as a boon for the patients of urolithiasis
References
-
Moe OW (2006) Kidney stones: pathophysiology and medical management. Lancet 367(9507): 333-344.
-
Tiselius HG (2003) Epidemiology and medical management of stone disease. BJU Int 91(8): 758-767.
-
Devuyst O, Pirson Y (2007) Genetics of hypercalciuric stone forming diseases. Kidney Int 72(9): 1065-1072.
-
Knoll T (2007) Stone disease. Eur Urol Suppl 6: 717-722.
-
Worcester EM, Coe FL (2008) Nephrolithiasis. Prim Care 35(2): 369-391.
-
Khan SR, Glenton PA, Backov R, Talham DR (2002) Presence of lipids in urine, crystals and stones: implications for the formation of kidney stones. Kidney Int 62(2): 2062-2072.
-
Pandeya DR, Adhikari D, Risal S, Baxi J, Singh PP (2006) Epidemiology and etiopathogenesis of urinary calculi in western Nepal (Pokhara) Nepal Med Coll J 8(3): 190-193.
-
Sharma N, Furber A, Lemaster J (2004) Study on urinary bladder stone cases at Okhaldhunga Hospital, Nepal. 1988-1994. Nepal Med Coll J 6(1): 49-52.
-
Stamatelou KK, Francis ME, Jones CA, Nyberg LM, Curhan GC (2003) Time trends in reported prevalence of kidney stones in the United States: 1976-1994. Kidney Int 63(5): 1817-1823.
-
Colobawalla BN (1971) Incidence of urolithiasis in India: ICMR Tech Rep Series No 8: 42-51.
-
Bakane BC, Nagtilak SB, Bhaidas p (1996) Urolithiasis in Satpura region: A Tribal Experience. International Med J 3: 215-217.
-
Ansari MS, Gupta NP, Hemal AK, Dogra PN, Seth A, et al. (2005) Spectrum of stone composition: structural analysis of 1050 upper urinary tract calculi from northern India. Int J Urol 12(1): 12-26.
-
Bakane BC, Nagtilak SB, Patil B (1999) Urolithiasis: A Tribal Scenario. Indian J Pediatr 66: 863-865.
-
Tiselius HG (2000) Stone incidence and prevention. Brazilian Journal of Urology 26(5): 452-462.
-
Coll DM, Varanelli MJ, Smith RC (2002) Relationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. AJR Am J Roentgenol 178(1): 101-103.
-
Park S, Pearle MS (2007) Pathophysiology and management of calcium stones. Urol Clin North Am 34(3): 323-334.
-
Miller NL, Evan AP, Lingeman JE (2007) Pathogenesis of renal calculi. Urol Clin North Am 34(3): 295-313.
-
Pendse AK, Singh PP (1986) The Etiology of Urolithiasis in Udaipur (Western Part of India). Urol Res 14: 59-62.
-
Coe FL, Parks JH, Asplin JR (1992) The pathogenesis and treatment of kidney stones. N Engl J Med 327(16): 1141- 1152.
-
Nabi G, Downey P, Keeley F, Watson G, McClinton S (2007) Extra-corporeal shock wave lithotripsy (ESWL) versus ureteroscopic management for ureteric calculi. Cochrane Database Syst Rev 24(1).
-
Tombolini P, Ruoppolo M, Bellorofonte C, Zaatar C, Follini M (2000) Lithotripsy in the treatment of urinary lithiasis. J Nephrol 13(3): S71-S82.
-
Chatterjee A, Pakrashi SC (2005) The Treatise on Indian Medicinal Plants, 2nd (Edn.), New Delhi: National Institute of Science Communication and Information Resources.
-
Khare CP (2003) Indian Herbal Remedies: Rational Western Therapy, Ayurvedic, and Other Traditional Usage, Botany. New Delhi: Springer, pp: 194-195.
-
Shankar A (2005) Pharmacological Basis of Indigenous Therapeutics, 1st [Edn.], Bhalani publication House, Mumbai.
- Management of Ear Keloid with Ksharsutra: A Case Study
- Yoga and Global Sustainability: A Holistic Path to One Earth, One Health
- Autoimmune Diseases in Ayurveda: A Narrative Review with Classical and Modern Perspectives
- Management of Cluster Headache Associated with Pituitary Apophysitis by CERT (Chakrasiddh Energy Release Technique): A Case Report on Energy Rebalancing
- Zygophyllum Geslini Coss : Biochemicals and Antioxidant Activity
- Observations of a Beginner Vaidya