Invasive Aspergillosis: Etiology, Clinical Presentation, Laboratory Diagnosis and Treatment
Aspergillosis is an opportunistic infection, usually seen in the patients having underlying diseases especially acquired immuno deficiency syndrome (AIDS). The present review article highlights the mechanism of infection, virulence factors, latest diagnostic methods and treatment strategies of aspergillosis in a precise manner.
Introduction
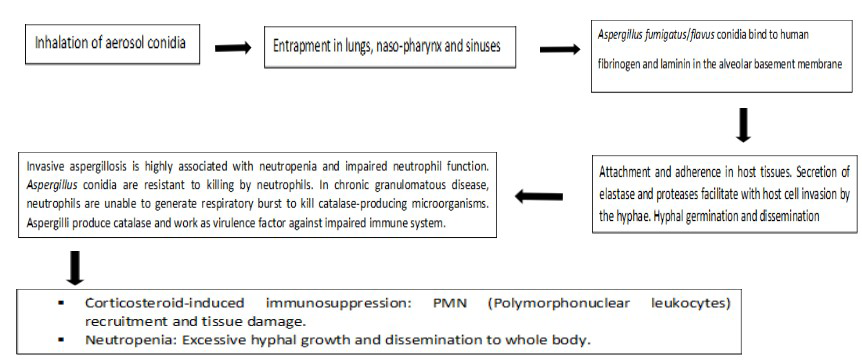
Fungal pathogens cause opportunistic infections [1, 2, 3, 4, 5]. The patients who are having underlying diseases usually present with these infections [6, 7]. The major cause is due to their impaired immune system. Aspergillus is an ubiquitous fungus that forms conidia (airborne spores). When these conidias are inhaled by an immunosuppressed individual, it leads to invasive aspergillosis [8, 9, 10]. In normal individuals with healthy immune system, these airborne spores are promptly cleared by the cells of the pulmonary immune system. However, the outcome is completely different in patients with suppressed immune system. Invasive aspergillosis is a cause of major morbidity and mortality in
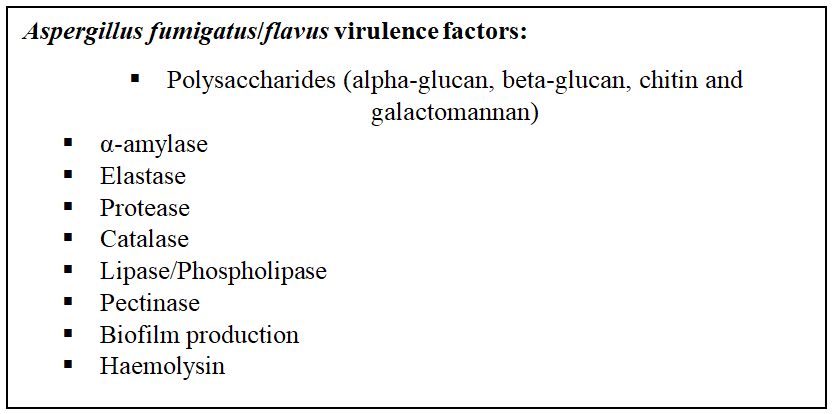
Virulence Factors
patients with immunocompromised states like patients with organ transplantation and AIDS (Figure 1) [11, 12, 13, 14, 15].
Invasive aspergillosis primarily involves lungs with necrotizing pneumonia being the key manifestation. As already mentioned, pathogenesis involves underlying conditions that weakens the immune system of the body. Few classic conditions associated with invasive aspergillosis are prolonged neutropenia, allogeneic hematopoietic cell transplant, receipt of high doses of corticosteroids and conditions associated with impaired cellular immune responses. Histologically, invasive aspergillosis is characterized by vascular invasion, consequent infarction and necrosis [16].
Mechanism of Infection (Figure 1)
Systemic Involvement and Clinical Presentation
Invasive aspergillosis typically involves the lungs. The clinical presentation involves fever, shortness of breath, hemoptysis and chest pain. On chest imaging studies, it could present in myriads of way: bronchopneumonia (patchy areas of consolidation), tracheo-bronchitis, single or multiple nodules and peri-bronchial infiltrates [17, 18].
When angio-invasive pattern is seen, the spread of infection goes much beyond lung; it spreads to multiple organs, including liver, skin, eyes, and kidneys. Dissemination to multiple organs carry poor prognosis. Disseminated aspergillosis can also involve the central nervous system; presenting with seizures and focal neurologic signs. Mycotic aneurysm formation can also be seen in the central nervous system [19, 20].
It can also involve heart, particularly endocardium. It would lead to development of endocarditis. Other than candida species, Aspergillus species are the well-known cause of mycotic endocarditis. Endocarditis caused by Aspergillus species is common in patients with prosthetic cardiac valves. Such patients typically present clinically with fever and embolic phenomenon; shedding of emboli is common due to friable nature of the vegetations [16, 21].
Ocular presentation with endophthalmitis is a distinctive disorder associated with disseminated, invasive aspergillosis. It could result in severe ocular pain and rapid visual loss. Gastrointestinal involvement, though rare, could present with appendicitis, entero-colitis and colonic ulcers. Cutaneous aspergillosis is common in patients with surgical trauma, burn injury and traumatic inoculation [16].
Histopathological Features
Histologically, invasive aspergillosis is characterized by vascular invasion and consequent areas of ischaemic necrosis, resulting infarction [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21].
Laboratory Diagnosis
The diagnosis of invasive aspergillosis can be made by following methods:
Imaging
Chest X-ray and CT (Computerized tomographic) scan provide proper detailed examination and help in the diagnosis. The fungal ball, aspergilloma can be visualized and is the specific presentation of the disease [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21].
Sputum Staining and Culture
The morning time sputum (Usually three samples) collected from the patient and transferred into appropriate culture medium (Potato dextrose agar) for culturing of the pathogen, Fig. 2a. This is performed to check and confirm that Aspergillus filaments are present in the sample. For identification of fungal pathogen the sputum staining can also be performed, especially the lactophenol cotton blue staining helps in the identification of Aspergilli conidia and hyphae In-vitro. This staining has its own limitations due to various factors (Figure 2b) [16, 17].
Blood test
Blood test is useful for examination of the viable fungal spores in the blood. The blood sample collected in BacTec
bottles and incubated at 370C for the growth of Aspergilli hyphae in the blood sample. Fungaemia, denotes the possible invasive aspergillosis in immunocompromised patients.
Biopsy/BAL (Broncho-alveolar lavage)
The fungus identified in histo-pathologic sections with septate hyphaes dichotomous acute angle branching. Special stains, like PAS (Periodic acid Schiff) or gomori methanamine silver are used to identify the hyphae and spores of the fungi. The cell wall made up of galactomannan and chitin and act as major antigen [16, 17].
Antigen Detection
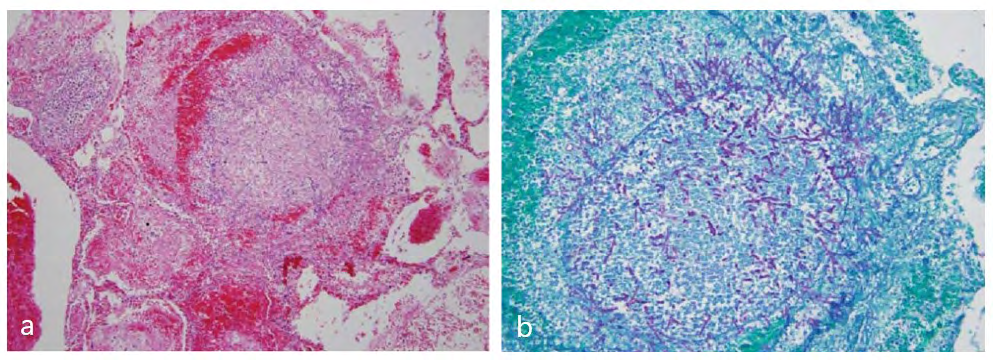
Galactomannan antigen detection in BAL (Broncho- alveolar lavage) fluid has been proven useful; particularly, in lung transplant recipients (Figure 3a & 3b, Figure 2) [16, 19].
![Figure 3: Invasive pulmonary aspergillosis. a) Pulmonary parenchyma with necrosis and pulmonary haemorrhage and Aspergillus hyphae (Haematoxylin and Eosin). b) Branching Aspergillus hyphae involving lung parenchyma (Grocott Methenamine Silver fungus stain) [16].](/fulltextimages/5704/fig_3.png)
Treatment and Control
A large number of drugs are recommended by the WHO and found effective for the treatment of invasive aspergillosis such as voriconazole, itraconazole, caspofungin, amphoteracin B and posaconazole. Most of the drugs inhibit ergosterol synthesis, which is a major component of cell membrane in fungal pathogens [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21].
Conclusion
Fungi usually cause opportunistic infection in humans.
The immunocompromised patients especially AIDS (Acquired immuno deficiency syndrome) patients reported with invasive aspergillosis.
Proper personel hygiene and healthier practices can minimize these kind of infections.
Authors’ Contributions
Both of the authors have contributed to the preparation of this review and editing of manuscript.
Conflicts of Interest
There are no conflicts of interest exists.
Authors’ Funding
No funding provided from organization or project.
References
-
Saghrouni F, Youssef YB, Gheith S, Bouabid Z, Abdeljelil JB, et al. (2011) Twenty-nine cases of invasive aspergillosis in neutropenic patients. Med Mal Infect 41(12): 657-662.
-
Sugui JA, Kwon-Chung KJ, Juvvadi PR, Latgé JP, Steinbach WJ (2014) _Aspergillus fumigatus_ and related species. Cold Spring Harb Perspect Med 5(2).
-
Barnes PD, Marr KA (2006) Aspergillosis: Spectrum of disease, diagnosis, and treatment. Infect Dis Clin North Am 20(3): 545-561.
-
Krishnan S, Manavathu EK, Chandrasekar PH (2009) _Aspergillus flavus_: An emerging non- fumigatus Aspergillus species of significance. Mycoses 52: 206-222.
-
Mosquera J, Warn PA, Morrissey J, Moore CB, Gil- Lamaignere C, et al. (2001) Susceptibility testing of _Aspergillus flavus_: Inoculum dependence with itraconazole and lack of correlation between susceptibility to amphotericin B in-vitro and outcome in- vivo. Antimicrob Agents Chemother 45(5): 1456-1462.
-
Chakrabarti A, Chatterjee SS, Das A, Shivaprakash MR (2011) Invasive aspergillosis in developing countries. Med Mycol 49: S35-S47.
-
Pasqualotto AC (2009) Differences in pathogenicity and clinical syndromes due to _Aspergillus fumigatus_ and _Aspergillus flavus_. Med Mycol 47(Suppl 1): S261-S270.
-
Hyde KD, Al-Hatmi AMS, Andersen B, Boekhout T, Buzina W, et al. (2018) The world’s ten most feared fungi. Fungal Divers 9: 161-194.
-
Engel TGP, Erren E, Melchers WJG, Reijers MH, Merkus P, et al. (2019) Aerosol transmission of _Aspergillus_ _fumigatus_ in cystic fibrosis patients in the Netherlands. Emerg Infect Dis 25(4): 797-799.
-
Abdalla MH (1988) Prevalence of airborne _Aspergillus_ _flavus_ in Khartoum (Sudan) airspora with reference to dusty weather and inoculum survival in simulated summer conditions. Mycopathologia 104(3): 137-141.
-
Adhikari A, Sen MM, Gupta-Bhattacharya S, Chanda S (2004) Airborne viable, non-viable, and allergenic fungi in a rural agricultural area of India: A 2-year study at five outdoor sampling stations. Sci Total Environ 326(1-3): 123-141.
-
Gupta SK, Pereira BM, Singh AB (1993) Survey of airborne culturable and non-culturable fungi at different sites in Delhi metropolis. Asian Pacific J Allergy Immunol 11(1): 19-28.
-
Chakrabarti A, Kaur H, Savio J, Rudramurthy SM, Patel A, et al. (2019) Epidemiology and clinical outcomes of invasive mould infections in Indian intensive care units (FISF study). J Crit Care 51: 64-70.
-
Al-Hatmi AMS, Castro MA, de Hoog GS, Badali H, Alvarado VF, et al. (2019) Epidemiology of _Aspergillus_ species causing keratitis in Mexico. Mycoses 62(2): 144-151.
-
Van de Veerdonk FL, Kolwijck E, Lestrade PPA, Hodiamont CJ, Rijnders BJA, et al. (2017) Influenza-associated aspergillosis in critically ill patients. Am J Respir Crit Care Med 196(4): 524-527.
-
Saubani AO, Tadi R, Kousha M (2011) Pulmonary Aspergillosis: a clinical review. Eur Respir Rev 2011; 20(121): 156-174.
-
Lueg EA, Ballagh RH, Forte V (1996) Analysis of the recent cluster of invasive fungal sinusitis at the Toronto Hospital for Sick Children. J Otolaryngol 25(6): 366-370.
-
Arnow PM, Sadigh M, Costas C, Weil D, Chudy R (1991) Endemic and epidemic aspergillosis associated with in- hospital replication of _Aspergillus_ organisms. J Infect Dis 164(5): 998-1002.
-
Schauwvlieghe AFAD, Rijnders BJA, Philips N, Verwijs R, Vanderbeke L, et al. (2018) Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir Med 6(10): 782-792.
-
Rotjanapan P, Chen YC, Chakrabarti A, Li RY, Rudramurthy SM, et al. (2018) Epidemiology and clinical characteristics of invasive mould infections: A multicenter, retrospective analysis in five Asian countries. Med Mycol 56(2): 186- 196.
-
Huang L, Zhang N, Huang X, Xiong S, Feng Y, et al. (2019) Invasive pulmonary aspergillosis in patients with influenza infection: A retrospective study and review of the literature. Clin Respir J 13(4): 202-211.
- Management of Ear Keloid with Ksharsutra: A Case Study
- Yoga and Global Sustainability: A Holistic Path to One Earth, One Health
- Autoimmune Diseases in Ayurveda: A Narrative Review with Classical and Modern Perspectives
- Management of Cluster Headache Associated with Pituitary Apophysitis by CERT (Chakrasiddh Energy Release Technique): A Case Report on Energy Rebalancing
- Zygophyllum Geslini Coss : Biochemicals and Antioxidant Activity
- Observations of a Beginner Vaidya