Roles of Melatonin and Phyto-Melatoninas an Anti-Cancer Molecule: An Evolutionary Perspective
Etymologically, melatonin (N-acetyl-5-methoxytryptamine) can be traced back to the origin of life. The first origin of melatonin was detected in cyano-bacteria. As considering the endosymbiont hypothesis, cyanobacteria were engulfed by the animal and plant cells. Later on, these bacteria performed the roles of mitochondria and chloroplastids in animals and plant cells respectively. Inner matrices of these organelles are having melatonin and probable function of this intra-organelle melatonin is to protect the organelles from the detrimental effects from free radicals (Reactive Oxygen Species; ROSs and Reactive Nitrogen Species; RNSs). In higher animals, melatonin is synthesized and secreted by the pineal gland mainly during the night, since light exposure suppresses its production. Other than pineal gland, melatonin is secreted from several different organs like retina, gastro-intestinal tract. The secretion of this hormone is regulated by several environmental factors like photo-period, temperature, humidity etc. Melatonin can exert its function either by as a free molecule or by its membrane bound receptors MT1 and MT2 respectively. Modulations of melatonin receptors results in stimulation of apoptosis, regulation of pro-survival signaling, inhibition on angiogenesis, metastasis, and induction of epigenetic alteration. Melatonin could also be utilized as adjuvant of cancer therapies, through reinforcing the therapeutic effects and reducing the side effects of chemotherapies or radiation. Melatonin could be an excellent candidate for prevention and treatment of several cancers, such as breast cancer, prostate cancer, gastric cancer and colorectal cancer. This review summarized the anticancer efficacy of melatonin, based on the results of epidemiological, experimental and clinical studies.
Introduction
Melatonin Synthesis and Pathophysiology
Melatonin (N-acetyl-5-methoxytryptamine) was first isolated and identified by Lerner, et al. from bovine pineal gland [1, 2]. It is the main neurohormone secreted during the dark hours in the dark by the vertebrate pineal body. Tryptophan is the precursor for melatonin biosynthesis, and is haunted from the circulation then converted into serotonin. Serotonin is then converted into N-acetylserotonin by the enzyme arylalkylamine-N-acetyl transferase (AANAT) while N-acetylserotonin is metabolized into melatonin by the enzyme hydroxyindole-O-methyltransferase (HIOMT, 2) Once formed, melatonin is released into the capillaries and in higher concentrations into the cerebrospinal fluidand is then rapidly distributed to most body tissues [3, 4]. Intravenously administered melatonin exhibits biexponential decay with a primary distribution half-life of two min and a second metabolic half-life of 20 min [5]. Circulating melatonin is metabolized mainly in the liver where it is first hydroxylated by cytochrome P450 mono-oxygenases and then conjugated with sulfate to form 6-sulfatoxymelatonin [6]. Melatonin is also metabolized by oxidative pyrole-ring cleavage into kynuramine derivatives. The primary cleavage product is N1-acetyl-N2-formyl-5-methoxykynuramine (AFMK), which is deformylated, either by arylamine formamidase or hemoperoxidases to N1-acetyl-5-methoxykynuramine [7, 8].
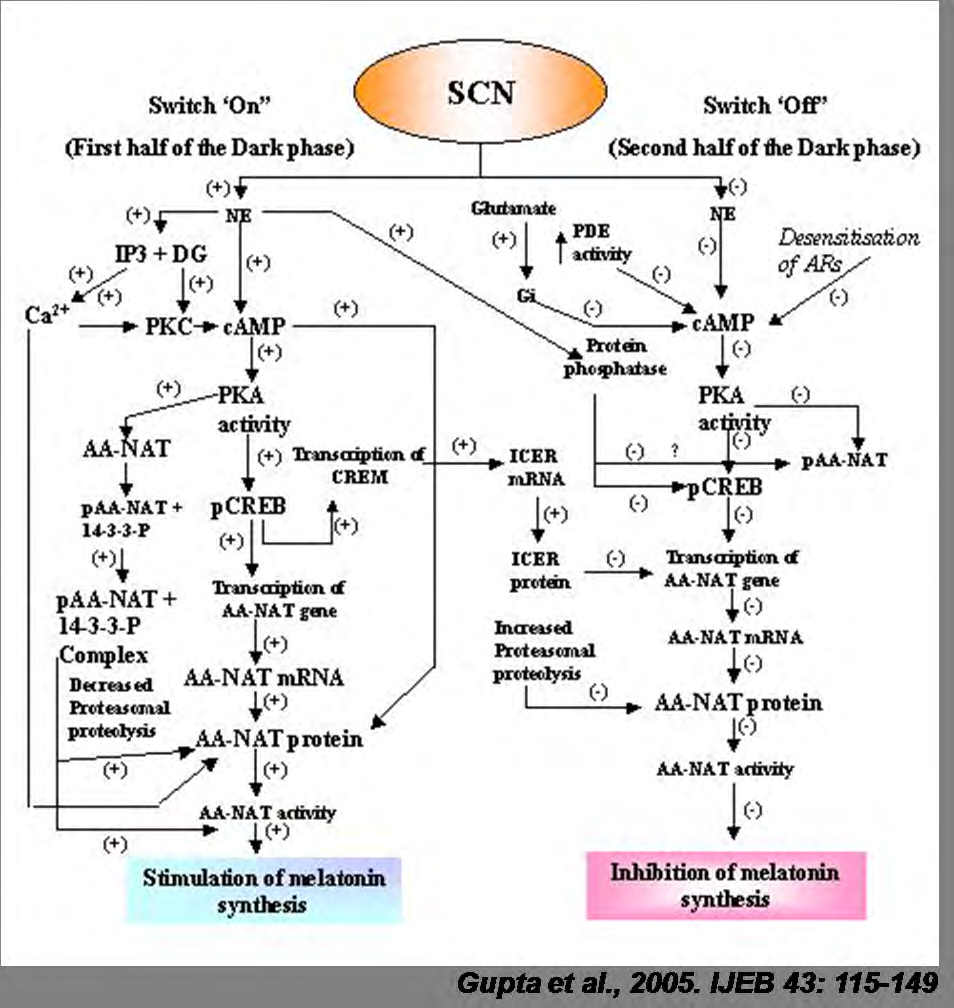
Some evidence has suggested that pyrrole ring cleavage contributes to about one-third of the total melatonin catabolism, but the percentage may be even higher in certain tissues. It has been proposed that AFMK is the primitive and primary active metabolite of melatonin [9]. The circadian pattern of pineal melatonin secretion is regulated by the mechanism that resides in mammals within the hypothalamic suprachiasmatic nucleus (SCN) of the hypothalamus. Lesions in the SCN abolish the rhythm of pineal melatonin production in mammals [10]. The SCN is synchronized to the environmental light–dark cycle by light perceived by the retina, acting mainly on a subgroup of retinal ganglion cells (RGCs) that contain the photo-pigment melanopsin [11]. These RGCs hook up with the SCN via the retino-hypothalamic tract. The SCN regulates pineal gland’s function through a polysynaptic network involving the paraventricular nucleus of the hypothalamus. Descending polysynaptic fibers from these regions project through the medial forebrain bundle and reticular formation takes place to the inter-medio-lateral horns of the cervical segments of the spinal cord [12]. Postganglionic sympathetic fibers from the superior cervical ganglia reach the pineal gland and regulate melatonin biosynthesis through the presynaptic release of nor-epinephrine (NE). NE release occurs during the “night” portion of the circadian pacemaker cycle provided that this occurs in a dark environment.
Activation of the pineal β-adrenergic receptors by NE results in increased 3′, 5′-cyclic adenosine monophosphate (cAMP) concentration that promotes the biosynthesis of melatonin [13]. α1-Adrenergic receptors potentiate β-adrenergic activity by producing a sharp increase in intracellular Ca2+ and activation of protein kinase C (PKC) and of prostaglandin synthesis [14, 15, 16]. The subcellular mechanisms involved in increase and turnoff of AANAT activity have been elucidated in great detail [17]. Cyclic AMP stimulates AANAT expression and phosphorylation via protein kinase A, which also allows AANAT to be stabilized by binding of 14-3-3 proteins [18, 19]. The nocturnal exposure to bright light suppresses melatonin production immediately by degradation of pineal AANAT [20]. It has now been demonstrated that melatonin is produced by many organs aside from the pineal body. These include the retina gastrointestinal tract skin lymphocytes and bone marrow [21, 22, 23, 24, 25]. Because pineal melatonin production occurs during the dark phase and is acutely suppressed by light, and, further, because melatonin is quickly cleared from the circulation following the cessation of its production, the time and duration of the melatonin peak reflect the environmental night period [26]. Plasma melatonin exhibits a circadian rhythm with high levels at night, and low levels during the day, attaining peak concentrations of plasma melatonin between 02:00 and 04:00 h. Longer nights are associated with a longer duration of melatonin secretion [26]. Hence melatonin is a signal of darkness that encodes time-of- day and length-of – day information to the brain including the SCN, brain and peripheral organs [27]. In mammals, melatonin is critical for the regulation of seasonal changes for various physiological, neuroendocrine and reproductive functions [28]. These actions of melatonin are processed in nuclei of the hypothalamus and in the pars tuberalis (PT) of the pituitary [29]. The following illustration as suggested by Gupta, et al. [30] shows the synthesis and regulation of synthesis of melatonin (Figure 1).
Different Functions of Melatonin
Melatonin is reported to have a role in sleep initiation as the trigger for opening the circadian “sleep gate”, acting as a sleep regulator [27]. Other actions of the hormone include inhibition of dopamine (DA) release in the hypothalamus and retina involvement in the aging process and pubertal development blood pressure control free-radical scavenging and regulation of the immune response [24]. If given during the day, when it’s not present endogenously, melatonin has soporific effects which resemble its action in the dark , i.e., it lowers blood heat and induces fatigue while concomitantly producing a brain activation pattern resembling that which occurs during sleep [31, 32, 33, 34, 35, 36, 37].
Melatonin production decreases with age and in certain diseases, e.g., certain malignancies, Alzheimer’s disease (AD) and cardiovascular disease [38, 39]. This decrease in melatonin output has been linked to insomnia in older patients and to a higher prevalence of cancer [40, 41].
Melatonin and Cancer
Overview of Role Of Melatonin in Cancer Development
Melatonin has been known to affect the expansion of tumors, and its secretion corresponds with the presence of sunshine and a biological time. The relationship between melatonin secretion, light, and cancer suggests that a rise within the prevalence of varied sorts of cancer corresponds with industrialization and exposure to more sorts of artificial light, thus leading to lower levels of nocturnal melatonin. In animals, pineal suppression and pinealectomy stimulate the growth and metastasis of experimental cancers of the lung, liver, ovary, pituitary, and prostate [42]. Mouse studies using different melatonin administration protocols showed that the drug decreased the incidence and size of mammary adenocarcinomas and lung metastases [43].
Melatonin and Breast Cancer
Clinical evidence and research have also shown the potential use of melatonin as a treatment for carcinoma patients. It was found that in women with carcinoma, the melatonin levels both in morning and evening were abnormal. Nocturnal melatonin levels were low while morning urine samples of breast cancer patients displayed high melatonin levels, the opposite of what is expected in healthy individuals [44]. Melatonin can bind to many receptors including MT1 and MT2, which are located in lymphocytes, platelets, prostatic cells, renal tubules, and cardiac myocytes and may also bind to nuclear receptors [45]. Binding to nuclear receptors allows melatonin to alter the transcription of genes and inhibit cell proliferation [45]. Pre-treatments with melatonin in estrogen receptor-alpha (ER alpha positive) MCF-7 human breast cancer cells reduced ER alpha trans- activation and binding activity and decreased the elevation of cAMP levels [46]. Decreased cAMP levels suppress the uptake and metabolism of linoleic acid (LA) and results in a reduction of the activation of the epidermal growth factor pathway and thus tumor growth inhibition [47]. In two studies conducted by Lissoni, et al. [48] melatonin was administered to breast cancer patients to observe the effects on tumor regression and other side effects. Women with metastatic carcinoma who had not skilled tamoxifen (TMX) alone got TMX at noon and melatonin within the evening. Final reports showed a reduction of lesions and a decrease in insulin-like growth factor (IGF-1) in patients [45]. A second trial was conducted to guage the consequences of high-dose melatonin in carcinoma patients receiving chemotherapy, which thanks to its high toxicity limited the frequency of treatment. After four cycles, the melatonin administered was observed to normalize platelet levels during a majority of the test subjects and cause tumor regression in 5 out of 12 patients with little toxicity reported [49].
Melatonin in Prostate and Colorectal Cancer
Melatonin has also been shown to enhance survival rates in patients with prostate and colorectal cancer. Studies have shown that men with primary localized malignant prostate tumors have extremely low levels of nocturnal melatonin that decrease with a rise in tumor growth [50]. Patients with unoperated colorectal carcinoma were found to have a significantly lower nocturnal plasma melatonin level compared to controls [51]. However, a second study conducted by Kvetnaia, et al. [52] found a higher nocturnal urinary metabolite 6-sulfatoxymelatonin (aMT6s) excretion in operated, untreated males. In one study of 54 patients with metastatic lung and colorectal tumors, the melatonin regimen resulted in stabilization of cancer and improved quality of life for roughly 40% of the recipients [42, 53]. As specified previously, the consequences of melatonin supplementations can change consistent with the time of administration. Melatonin injections given within the morning are found to stimulate cancer growth while injections within the evening contribute to tumor regression. Afternoon injections have no apparent effect [42].
Melatonin in Organ Specific Cancer
Melatonin has also been shown to affect tumor growth within the thyroid, bronchi, and stomach among other sorts of cancer. In female patients with thyroid cancer, the amount of aMT6s were extremely low and didn’t differ from patients with benign thyroid diseases, indicating that thyroid growth negatively affects the proper regulation of the pineal gland [53]. In contrast to this finding, Hunt, et al. [54] found significantly elevated levels of aMT6s in thyroid cancer patients [50]. Similarly, several found depressed nocturnal aMT6s-excretion in early stage male bronchial cancer patients while others reported high morning and nighttime melatonin levels of late-stage patients [55]. Furthermore, male patients with primary, un operated stomach cancer displayed a depletion of the nocturnal urinary excretion of aMT6s. Results from other melatonin-cancer studies achieved similar results: some studies reported reduced nocturnal aMT6s levels while other studies reported high levels. Results from various studies show that melatonin has a clear effect on cancer development, but the discrepancies among the studies prompt further research into the connection between melatonin and cancer.
Relationship Between Melatonin and Cancer Risk
With industrialized society drifting more towards a life situated within the presence of 24-hour light, the occurrence of sleep disorders and abnormal sleep patterns continues to extend. As a result, circadian rhythms regulating cellular and physiological processes, like the secretion of melatonin, have taken a big toll on the power to synchronize to the environment. Extended periods of exposure to light further inhibit the assembly and secretion of melatonin from the pineal body through proteasomal proteolysis. Decreased endogenous secretion of melatonin has been shown through various clinical and mouse studies and has been linked to a better risk of certain sorts of cancer. Recent epidemiological studies have shown that ladies working night shifts are at a greater risk of breast, endometrial, and colorectal cancer while male night shift workers are at a significantly increased risk of developing prostatic adenocarcinoma presumably thanks to their increased exposure to light in the dark [47]. Individuals with various tumor types exhibited depressed nocturnal melatonin concentrations or nocturnal excretion of the main metabolite, 6-sulfatoxymelatonin [56]. There has been a particularly close link between melatonin levels and the risk of breast cancer. Data collected from the ladies involved in epidemiological studies included urinary melatonin levels (measuring specifically levels of 6- sulfatoxymelatonin), sleep duration, and shift work [57]. The results from the many studies conducted throughout the world, however, displayed contradicting information. Breast cancer risk was found to be elevated with decreased urinary melatonin levels within the Nurses’ Health Study II, but results from the united kingdom Guernsey Cohort study showed very little significant association between levels of urinary melatonin and therefore the risk of carcinoma [58, 59].
Melatonin and the Prevention of Cancer Growth
Cancer patients in controlled trials conducted by Wang et al. further showed that melatonin significantly improved complete and partial remission, was related to a 1-year survival rate, and dramatically decreased radio-chemotherapy-related side effects including thrombocytopenia, neurotoxicity, and fatigue [60]. Mouse studies have demonstrated the inhibition of the development of breast cancer models by melatonin as well as the growth of tumors in rodents with exposure to long periods of sunshine via a melatonin-induced suppression of tumor linolic acid uptake and its metabolism to the mitogenic signaling molecule 13-HODE [61]. Due to melatonin’s ability to suppress cAMP formation, it inhibits the uptake of LA and its metabolism to 13-HODE by a MEL receptor-mediated mechanism found in rat hepatomas and human breast cancer xenografts Travis RC, [60] Endothelin-1 (EDN1) is an angiogenic factor that promotes the growth of tumors in the blood vessels. To combat this factor, melatonin inhibits the synthesis of endothelin-1 to dam the expansion of cancer cells [45]. There is evidence that the administration of melatonin alone or in combination with interleukin-2 or chemo-radiotherapy in patients with advanced tumors is associated with tumor regression and improved survival rates [62]. Melatonin prevents the proliferation of cancer cells by reducing telomere length and telomerase activity, both of which are responsible for the development of unhealthy cells and high levels of the hormone, suppressing the tumor- promoting gene TP53 [45]. Additional data from clinical studies further establishes that the utilization of melatonin has minor side effects, and thus it’s a hormone growing in popularity for the event of cancer treatments.
Adverse Effects of Melatonin as an Anti-Cancer Treatment
Clinical trials using melatonin as an anti-cancer treatment and studies conducted on the role of melatonin within the prevention of cancer development show the surging potential of melatonin as a therapeutic medication to combat sleep disorders, cancer, and therefore the side effects of chemotherapy. As seen in both animals and humans, melatonin features a very low level of toxicity, and even in relatively high doses, it typically doesn’t cause major side effects [42]. Minor side effects, however, include headaches, dizziness, and drowsiness as well as nausea and apathy combined with weight gain [63, 64]. Melatonin treatment in children, however, can be sustained long-term without severe deviations of normal development, such as sleep quality, puberty, and mental health [64]. Although melatonin has been successfully utilized in cancer and disorder treatments, improper timing of use may result in negative outcomes. Melatonin injections within the morning can stimulate tumor growth; doses within the afternoon exhibit no effect, and doses within the evening have retarding effects [42]. Animal studies have shown that large doses of melatonin increased light-induced damage to retinal photoreceptors (ganglion cells, rods, and cones) [65]. Furthermore, administration of melatonin that elongates the normal nocturnal melatonin pattern has been shown to exacerbate SAD, bipolarity, and classic depression [42]. Melatonin is an easily accessible drug provided as an over-the-counter supplement. With its various roles in physiology and cellular processes, it can also interact with many other drugs, like anticoagulants, interleukin-2, and antidepressant medications [65]. Studies show that melatonin can increase the risk of bleeding from anticoagulant medications such as warfarin, increase tumor regression and survival rates of cancer in conjunction with IL-2, and reduce antidepressant effects of medicine like desipramine [66, 67].
Conclusion
The pineal hormone and drug supplement, melatonin, plays a major role in maintaining circadian rhythms throughout the body. Not only is it involved in the normalizing of biological rhythms, but it is also observed to function in the immune system, in the reproductive system, as an antioxidant, and as an anti-cancer treatment. Through a series of apoptosis pathways and interactions with the immune system, chemotherapy, and anti-cancer drugs, melatonin can help increase tumor regression in cancer patients. Melatonin has been shown to induce many positive effects to protect the body and cells from damage, but improper administration can culminate in hazardous effects, including the stimulation of tumor growth. The studies conducted until now have shown great potential for the clinical use of melatonin to target certain diseases; however, more research must be completed to establish the precise role of melatonin in the body and its range of effects on physiology and behavior.
Acknowledgements
There is no acknowledgement
Consent for Publication
Not Applicable.
Conflict of Interest
The author confirms that this chapter contents have no conflict of interest.
References
-
Lerner AB, Case JD, Takahashi Y, Lee TH, Mori W, et al. (1958) Isolation of melatonin, a pineal factor that lightens melanocytes. J Am Chem Soc 80(10): 2587.
-
Axelrod J, Wurtman RJ (1968) Photic and neural control of indoleamine metabolism in the rat pineal gland. Adv Pharmacol 6: 157-166.
-
Tricoire H, Moller M, Chemineau P, Malpaux B (2003) Origin of cerebrospinal fluid melatonin and possible function in the integration of photoperiod. Reprod Suppl 61: 311-321.
-
Cardinali DP, Pevet P (1998) Basic aspects of melatonin action. Sleep Med Rev 2(3): 175-190.
-
Claustrat B, Brun J, Chazot G (2005) The basic physiology and pathophysiology of melatonin. Sleep Med Rev 9(1): 11-24.
-
Skene DJ, Papagiannidou E, Hashemi E, Snelling J, Lewis D F, et al. (2001) Contribution of CYP1A2 in the hepatic metabolism of melatonin: studies with isolated microsomal preparations and liver slices. J Pineal Res 31: 333-342.
-
Hardeland R, Reiter RJ, Poeggeler B, Tan D X, et al. (1993) The significance of the metabolism of the neurohormone melatonin: antioxidative protection and formation of bioactive substances. Neurosci Biobehav Rev 17(3): 347-357.
-
Tan DX, Manchester LC, Terron MP, Flores LJ, Reiter RJ, et al. (2007) One molecule, many derivatives: a never- ending interaction of melatonin with reactive oxygen and nitrogen species? J Pineal Res 42(1): 28-42.
-
Tan DX, Manchester LC, Reiter RJ, Karbownik M, Calvo JR, et al. (2000) Significance of melatonin in antioxidative defense system: reactions and products.Biol Signals Recept 9(3-4): 137-159.
-
Klein DC, Moore RY (1979) Pineal N-acetyltransferase and hydroxyindole-O-methyltransferase: control by the retinohypothalamic tract and the suprachiasmatic nucleus. Brain Res 174(2): 245-262.
-
Berson DM, Dunn FA, Takao M (2002) Phototransduction by retinal ganglion cells that set the circadian clock. Science 295(5557): 1070-1073.
-
Buijs RM, Hermes MH, Kalsbeek A (1998) The suprachiasmatic nucleus paraventricular nucleus interactions: a bridge to the neuroendocrine and autonomic nervous system. Prog Brain Res 119: 365- 382.
-
Klein DC, Weller JL, Moore RY (1971) Melatonin metabolism: neural regulation of pineal serotonin: acetyl coenzyme A N-acetyltransferase activity. Proc Nat Acad Sci USA 68(12): 3107-3110.
-
Vacas MI, Lowenstein P, Cardinali DP (1980) Dihydroergocryptine binding sites in bovine and rat pineal glands. J Auton Nerv Syst 2(4): 305-313.
-
Ho AK, Klein DC (1987) Activation of alpha 1-adrenoceptors, protein kinase C, or treatment with intracellular free Ca2+ elevating agents increases pineal phospholipase A2 activity. Evidence that protein kinase C may participate in Ca2+ dependent alpha 1-adrenergic stimulation of pineal phospholipase A2 activity. J Biol Chem 262(24): 11764-11770.
-
Krause DN, Dubocovich ML (1990) Regulatory sites in the melatonin system of mammals. Trends Neurosci 13(11): 464-470.
-
Maronde E, Stehle JH (2007) The mammalian pineal gland: known facts, unknown facets. Trends Endocrinol Metab 18(4): 142-149.
-
Schomerus C, Korf HW (2005) Mechanisms regulating melatonin synthesis in the mammalian pineal organ. Ann N Y Acad Sci 1057: 372-383.
-
Ganguly S, Weller JL, Ho A, Chemineau P, Malpaux B, et al. (2005) Melatonin synthesis: 14-3-3-dependent activation and inhibition of arylalkylamine N acetyltransferase mediated by phosphoserine-205. Proc Natl Acad Sci USA 102(4): 1222-1227.
-
Gastel JA, Roseboom PH, Rinaldi PA, Weller JL, Klein DC, et al. (1998) Melatonin production: proteasomal proteolysis in serotonin N-acetyltransferase regulation. Science 279(5355): 1358-1360.
-
Cardinali DP, Rosner JM (1971) Metabolism of serotonin by the rat retina ‘‘in vitro’’. J Neurochem18(9): 1769- 1770.
-
Raikhlin NT, Kvetnoy IM (1976) Melatonin and enterochromaffine cells. Acta Histochem; 55(1): 19-24.
-
Slominski A, Fischer TW, Zmijewski MA, Wortsman J, Semak I, et al. (2005) On the role of melatonin in skin physiology and pathology. Endocrine 27(2): 137-148.
-
Vico CA, Calvo JR, Abreu P, Lardone PJ, Mauriño SG, et al. (2004) Evidence of melatonin synthesis by human lymphocytes and its physiological significance: possible role as intracrine, autocrine, and/or paracrine substance. FASEB J 18(3): 537-539.
-
Conti A, Conconi S, Hertens E, Sonta ks, Markowska M, et al. (2000) Evidence for melatonin synthesis in mouse and human bone marrow cells. J Pineal Res 28(4): 193- 202.
-
Cardinali DP, Furio AM, Reyes MP, Brusco LI (2006) The use of chronobiotics in the resynchronization of the sleep–wake cycle. Can Causes Cont 17: 601-609.
-
Perumal PSR, Zisapel N, Srinivasan V (2005) Melatonin and sleep in aging population. Exp Gerontol 40(12): 911- 925.
-
Reiter RJ (1980) The pineal and its hormones in the control of reproduction in mammals. Endo Rev 1(2): 109-131.
-
Lincoln GA (2006) Melatonin entrainment of circannual rhythms. Chronobiol Int 23(1-2): 301-306.
-
Gupta BBP, Spessert R, Vollrath L (1995) Molecular components and mechanism of adrenergic signal transduction in mammalian pineal gland: regulation of melatonin synthesis. Ind J Exp Biol 43(2): 115-149.
-
Zisapel N (2001) Melatonin-dopamine interactions: from basic neurochemistry to a clinical setting. Cell Mol Neurobiol 21(6): 605-616.
-
Karasek M (2004) Melatonin, human aging, and age- related diseases. Exp Gerontol 39(11-12): 1723–1729.
-
Salti R, Galluzzi F, Bindi G, Perfetto F, Tarquini R, et al. (2000) Nocturnal melatonin patterns in children. J Clin Endocrinol Metab 85(6): 2137-2144.
-
Scheer FA, Montfrans VGA, Someren VEJ, Mairuhu G, Buijs RM et al. (2004) Daily night time melatonin reduces blood pressure in male patients with essential hypertension. Hypertension 43(2): 192-197.
-
Grossman E, Laudon M, Yalcin R, Zengil H, Peleg E, et al. (2006) Melatonin reduces night blood pressure in patients with nocturnal hypertension. Am J Med 119(10): 898-902.
-
Tan DX, Manchester LC, Di Mascio P, Martinez GR, Prado FM, et al. (2007) Novel rhythms of N1-acetyl-N2- formyl- 5-methoxykynuramine and its precursor melatonin in water hyacinth: importance for phyto-remediation. The FASEB J b 21(8): 1724-1729.
-
Gorfine T, Zisapel N (2007) Melatonin and the human hippocampus, a time dependant interplay. J Pineal Res 43(1): 80-86.
-
Girotti L, Lago M, Ianovsky O, Elizari MV, Dini A, et al. (2003) Low urinary 6-sulfatoxymelatonin levels inpatients with severe congestive heart failure. Endocr 22(3): 245-248.
-
Perumal PSR, Srinivasan V, Poeggeler B, Hardeland R, Cardinali DP, et al. (2007) Drug insight: the use of melatonergic agonists for the treatment of insomnia focus on ramelteon. Nat Clin Pract Neurol 3(4): 221-228.
-
Leger D, Laudon M, Zisapel N (2004) Nocturnal 6-sulfatoxymelatonin excretion in insomnia and its relation to the response to melatonin replacement therapy. Am J Med 116(2): 91-95.
-
Bartsch C, Bartsch H (2006) The anti-tumor activity of pineal melatonin and cancer enhancing life styles in industrialized societies. Can Causes Cont 17(4): 559- 571.
-
Malhotra S, Sawhney G, Pandhi P (2004) The therapeutic potential of melatonin: A review of the science. Med Gen Med 6(2): 46.
-
Anisimov VN, Alimova IN, Baturin DA, Popovich IG, Zabezhinski MA, et al. (2003) The effect of melatonin treatment regimen on mammary adenocarcinoma development in HER-2/neu transgenic mice. Int J Cancer 103(3): 300-305.
-
Bartsch C, Bartsch H, Jain AK,Laumas KR, Wetterberg L, et al. (1981) Urinary melatonin levels in breast cancer patients. J Neural Transm 52(4): 281-294.
-
Agrawal A, Darbari S, Rai TP, Kulkarni GT (2016) Role of Melatonin in the Pathophysiology of Cancer. J Chron DD 7: 1-6.
-
Keifer T, Ram PT, Yuan L, Hille S M (2002) Melatonin inhibits estrogen receptor transactivation and cAMP levels in breast cancer cells. Breast Cancer Res Treat 71(1): 37-45.
-
Blask DE (2009) Melatonin, sleep disturbance and cancer risk. Sleep Med Rev 13(4): 257-264.
-
Lissoni P, Barni S, Tancini G, Ardizzoia A, Rovelli F, et al. (1993) Immunotherapy with subcutaneous low-dose interleukin-2 and the pineal indole melatonin as a new effective therapy in advanced cancers of the digestive tract. Br J Cancer 67(6): 1404-1407.
-
Kaczor T (2010) An overview of melatonin and breast cancer. Nat Med Journal 2: 2.
-
Bartsch C, Bartsch H, Fluchter St H (1993) Depleted pineal melatonin production in primary breast and prostate cancer is connected with circadian disturbances: possible role of melatonin for synchronization of circadian rhythmicity. In: Touitou Y, et al. (Eds.), Melatonin and the Pineal Gland - From Basic Science to Clinical Application, New York 311-316.
-
Khoory R, Stemme D (1988) Plasma melatonin levels in patients suffering from colorectal carcinoma. J Pineal Res 5(3): 251-258.
-
Kvetnaia TV, Kvetnoy IM, Bartsch H Bartsch C, Mecke D (2001) Melatonin in patients with cancer with extra- reproductive location. In: Bartsch C, et al. (Eds.), The Pineal Gland and Cancer: Gland and Cancer. Springer, Berlin, Heidelberg 177-196.
-
Dogliotti L, Berruti A, Buniva T, Torta M, Bottini A, et al. (1990) Melatonin and human cancer. J Steroid Biochem Mol Biol 37(6): 983-987.
-
Hunt AE, Al-Ghoul WM, Gillette MU, Dubocovich ML (2001) Activation of MT (2) melatonin receptors in rat suprachiasmatic nucleus phase advances the circadian clock. Am J Physiol Cell Physiol 280(1): C110-C118.
-
Viviani S, Bidoli P, Spinazze S, Rovelli F, Lissoni P, et al. (1992) Normalization of the light/dark rhythm of melatonin after prolonged subcutaneous administration of interleukin-2 in advanced small cell lung cancer patients. J Pineal Res 12(3): 114-117.
-
Sánchez Hidalgo M, Guerrero JM, Villegas I, Packham G, de la Lastra CA (2012) Melatonin, a natural programmed cell death inducer in cancer. Curr Med Chem 19(22): 3805-3821.
-
Rondanelli M, Faliva MA, Perna S, Antoniello N (2013) Update on the role of melatonin in the prevention of cancer tumorigenesis and in the management of cancer correlates, such as sleep-wake and mood disturbances: review and remarks. Aging Clin Exp Res 25(5): 499-510.
-
Schernhammer ES, Hankinson SE (2005) Urinary melatonin levels and breast cancer risk. J Natl Cancer Inst 97(14): 1084-1087.
-
Travis RC, Allen DS, Fentiman IS, Key TJ (2004) Melatonin and breast cancer: a prospective study. J Natl Cancer Inst 96(6): 475-482.
-
Ye-min W, Bao-zhe J, Ai F, Chang-hong D, Yi-zhong L, et al. (2012) The efficacy and safety of melatonin in concurrent chemotherapy or radiotherapy for solid tumors: a meta-analysis of randomized controlled trials. Cancer Chemother Pharmacol 69(5): 1213-1220.
-
Blask DE, Dauchy RT, Sauer LA (2005) Putting cancer to sleep at night: the neuroendocrine/circadian melatonin signal. Endocrine 27(2): 179-88.
-
Cutando A, López-Valverde A, Arias-Santiago S, DE Vicente J, DE Diego RG, et al. (2012) Role of Melatonin in Cancer Treatment. Anticancer Res 32(7): 2747-2753.
-
Bauer BA (2013) Melatonin side effects: What are the risks? Psychlinks Psychology and Mental Health Support Forum.
-
Van Geijlswijk IM, Mol RH, Egberts TCG, Smits MG (2011) Evaluation of sleep, puberty and mental health in children with long-term melatonin treatment for chronic idiopathic childhood sleep onset insomnia. Psychopharmacol (Brel) 216(1): 111-120.
-
Wiechmann AF, O’Steen WK (1992) Melatonin increases photoreceptor susceptibility to light-induced damage. Invest Ophthalmol Vis Sci 33(6): 1894-1902.
-
Penn State Hershey. Possible Interactions with: Melatonin.
-
University of Maryland Medical Center. Possible Interactions with: Melatonin.
- Management of Ear Keloid with Ksharsutra: A Case Study
- Yoga and Global Sustainability: A Holistic Path to One Earth, One Health
- Autoimmune Diseases in Ayurveda: A Narrative Review with Classical and Modern Perspectives
- Management of Cluster Headache Associated with Pituitary Apophysitis by CERT (Chakrasiddh Energy Release Technique): A Case Report on Energy Rebalancing
- Zygophyllum Geslini Coss : Biochemicals and Antioxidant Activity
- Observations of a Beginner Vaidya