Clinical Efficacy of Katutrikadya Churna in the Management of Post-Operative Care in Bhagandara w.s.r to Fistula in Ano: A Comparative Study
In Ayurveda, there are eight branches. Ayurveda has eight branches. Because of its rapid action, use of surgical instruments (Yantra & shastra), Kshar & Agni, and inclusion of characteristics common to other branches, Shalyatantra is regarded as a notable branch. anushastra treats a wide range of illnesses (Para-surgical measures). The treatment of Bhagandara serves as the most significant, practical illustration of how anushastra, or ksharsutra, is used (Fistula-in-ano). Ayurveda classifies several disorders as “Mahagada” based on their severity and problematic behaviors. One of these is called Bhagandara (Fistula-inano). Many surgeons employ ksharsutra, with some somewhat successful outcomes. A lot of discomfort is experienced by the patient both during and after ksharsutra treatment. They are therefore afraid to change the kshar sutra later. In this study, katutrikadya churna with anupana of kulattha kwath, medications in compound formulation (30 patients), and Control group (30 Patients) were chosen. This group was given tab. diclofenac sodium as treatment. After meals, each group receives their particular medication twice daily. When the applied kshar-sutra has been changed with new kshar-sutra, follow-up is done every seventh day (weekly) for twenty days in a row. Aim: To Study the clinical efficacy of katutrikadya churna in the management of postoperative care W.S.R to bhagandara. Objectives • To assess the effect of compound formulation of katutrikadya churna after kshara-sutra application w.s.r to bhagandara. • To assess the agnidipan, vatanulomana property of katutrikadya churna. • Comparison in between the effect of katutrikadya churna and diclofenac sodium after kshar-sutra application w.s.r to bhagandara. • This clinical investigation was comparative, open, randomized, and study. The study's findings demonstrated that katutrikadya churna is a potent vedanasthapan aushadhi (analgesic) in the pain experienced over the anal region during the administration of kshar-sutra for the treatment of bhagandara. Not only does katutrikadya churna heal the symptoms of ailments, but it also addresses their root causes.
Materials and Methods
Research Design
- A Randomized Control Trial Participant
- Patients: After ksharsutra application in bhagandara.
- Gender-Both Male and Female
- Age-From 18 yrs-60 yrs of age.
Sampling Procedure
Comparative, Open, Random sampling
| Groups | No. of patients | Age | Gender | Intervention | Anupan | Dose/day | Duration |
|---|---|---|---|---|---|---|---|
| Group A-Interventional | 30 | 18 yrs to 60 yrs | Male and Female | Katutrikadya churna | luke warm kulattha kwath | 4 gms orally twice a day after breakfast and then at | Three follow ups were taken once in a week. |
| bed time after dinner. | |||||||
| Group B -Control Group | 30 | 18 yrs to 60 yrs | Male and Female | Tb.Diclofenac sodium | water | 50 mg orally BD | Three follow ups were taken once in a week. |
Table 1: Grouping.
Selection of Cases
Patients after ksharsutra application in bhagandara with classical signs and symptoms after postoperative procedure were selected after clinical & objective examination. I had selected 60 patients of postoperative bhagandara. These patients were selected randomly. Follow-up assessment was done by specially prepared case record forms of every patient to meet all baseline requirement. Follow-up signs & symptoms were recorded.
Method of Selection of Patients
Inclusion Criteria
- Age 18 - 60 yrs.
- Patients were selected irrespective of gender, caste & religion.
- The Patients of fistula in ano, whose fistulous tract already ligated with plane thread, were selected for kshar sutra application.
- After application of kshar sutra application. After application of kshar sutra patient suffering with pain
Drug
were selected.
Exclusion Criteria
- The participants were not selected below the age of 18 years and above the age of 60 years.
- The patients suffering from bhagandara but associated with malignancy, uncontrolled diabetes mellitus, uncontrolled hypertension, prolonged bleeding and clotting time, severe anaemia and critically ill patients were not selected for the study.
- Patients who had discontinued the treatment during follow up and
- Patients who had developed any serious complications were dropped out from the study.
Investigations
- Blood Investigations: CBC with ESR,
- Random blood sugar level,
- Bleeding time and clotting time.
| Sr. No. | Name | Latin name | Part |
|---|---|---|---|
| 1 | Shunthi | Zinziber officinale | 1 part |
| 2 | Marich | piper nigrum | 1 part |
| 3 | Pippali | Piper longum | 1 part |
| 4 | vacha | Acorus calamus | 1 part |
| 5 | Hingu | Ferula narthex | 1 part |
| 6 | Ajmoda, | Carum Roxburghianum | 1 part |
| 7 | Saindhava | Rocksalt | 1 part |
| 8 | Kulattha | Dolichos biflorus | 1 part |
Table 2: Contents of _Katutrikadya churna_.
Method of Preparation
Katutrikadya churna (KC) was prepared in the laboratory by following classical method described in ‘Ayurvedic Formulary of India’. In addition, its main ingredients include traditional medicinal herbs [9]. All the ingredients of were procured from the local market. All these drugs were taken in powdered form in equal proportion to form “Katutrikadya Churna.”
Standardization of “Katutrikadya Churna”
- Description - Greenish brown colour powder
- Loss on drying - 8.86 %W/W
- Total ash - 32.93 %W/W
- Acid insoluble ash - 6.86 %WW
- Water soluble extractive - 16.57 %W/W
- Alcohol soluble extractive - 0.18 %W/W Diet: All Pathyakar ahar vihar mentioned in Bhagandara. Pathya: Munga Dal, Balmulak, Patola, Shignu, Anabhishyandhi and Pathya diet. Apathya: Amla, Lavana and Katu Rasa Pradhan Dravya, Madya, Cured, Maash, Cold water, Vyayama, Maithuna, Krodha, Prishthayan (traveling), excessive sitting, excessive walking, excessive standing, Ratrijagarana, Divaswap. Follow up: (1) Symptomatic improvement, after every week up to 21 days. Case Record Form: Record, of all patients included in trial is documented & follow up is mentioned in case record forms. Clinical examination: Complete clinical examination from the point of view of bhagandara to diagnose & assess the condition of patient. Criteria of assessment: Assessment of patients was done subjectively as well as objectively. Subjective: Pain alleviation was the primary criterion used to evaluate improvement in the pain. For this reason, the level of pain was graded based on how it felt when sitting, moving, sleeping, and how long it persisted.
| Sr. No | Parameters | Symptoms | Scoring |
|---|---|---|---|
| 1 | Severity of pain | Excruciating | 5 |
| Horrible | 4 | ||
| Distressing | 3 | ||
| Discomforting | 2 | ||
| Mild Pain | 1 | ||
| No pain | 0 | ||
| Duration of persistence of pain | > 1 hr after application of Kshar-Sootra. | 5 | |
| <1 hr after application of Kshar-Sootra. | 4 | ||
| <45 mins after application of Kshar-Sootra. | 3 | ||
| <30 mins after application of Kshar-Sootra. | 2 | ||
| <15 mins after application of Kshar-Sootra | 1 | ||
| No pain | 0 | ||
| 3 | Size of mandalas | 2cm | 4 |
| 1.5cm | 3 | ||
| 1cm | 2 | ||
| 0.5cm | 1 | ||
| 0cm | 0 | ||
| 4 | Agnimadya | Present and not relieve even with the use of appetizer. | 3 |
| Present but relieve with the use of appetizers. | 2 | ||
| Translantly present | 1 | ||
| Absent | 0 | ||
| 5 | Malapravritti | Malavarodha (Not passing stool > 1 day) | 3 |
| Mild Malavarodha (Not passing stool since 1 day) | 2 | ||
| Passing stool daily but having painful de defecation | 1 | ||
| Samyak | 0 | ||
| 6 | Mutraipravritti | Mutravarodha | 3 |
| (Not passing urine since last 8-12 hrs) | |||
| Asamyak-Sadaha and Sakashta | 2 | ||
| Asamyak-Sadaha | 1 | ||
| Samyak | 0 | ||
| 7 | Gastric Irritability | Score 2+ Vomiting | 3 |
| Score 1+ Abdominal pain | 2 | ||
| Flatulence, Belching, Heart burn | 1 | ||
| Absent | 0 | ||
| 8 | Pus Discharge | Profuse discharge | 3 |
| (needs more than 3 pads / day) | |||
| Moderate discharge | 2 | ||
| (needs 2-3 pads / day) | |||
| Mild discharge (needs single pad/day) | 1 | ||
| No discharge | 0 |
Table 3: Gradations of practically observed symptoms.
Total effects of therapy
The percentage of symptom and sign alleviation for each patient will be as follows, and they will be categorized as either “cured,” “markedly improved,” “improved,” or “unchanged” according to the definition provided.
- Cured: if all indications and symptoms have disappeared completely, coupled with specific lab results, and the condition has persisted for about a year without medication.
- Marely improved: Significantly improved - A 50% or
Observation and Results
greater reduction in the patient’s signs and symptoms as well as specific changes in physical and biochemical parameters will be regarded as significant improvements.
- Improved: Signs and symptoms must be reduced by 25% to 50% to meet the assessment criteria in order to be judged improved.
- Unchanged: Patients who do not see any improvement in their signs, symptoms, or test results will be regarded unaltered. Additionally, the patient who has improved by less than 25% is still included in this category.
| Sr.no | Range of Age | Experimental Group | Control Group | ||
|---|---|---|---|---|---|
| No. of patients Gr. | % | No. of patients Gr. B (n=30) | % | ||
| A(n=30) | |||||
| 1 | 18-39 | 18 | 60.00 % | 14 | 43.33% |
| 2 | 40-60 | 12 | 40.00% | 17 | 56.66% |
| Total | 30 | 100% | 60 | 100% |
Table 4: Showing Age Wise Distribution in 60 patients of bhagandara.
| Sr.no | Gender | Experimental Group | Control Group | ||
|---|---|---|---|---|---|
| No. of patients Gr. | % | No. of patients Gr. B (n=30) | % | ||
| A(n=30) | |||||
| 1 | Male | 23 | 76.67 % | 25 | 83.33% |
| 2 | Female | 7 | 23.33% | 5 | 16.67% |
Table 5: Showing Gender wise Distribution in 60 patients of Bhagandara.
| Sr.no | Gender | Experimental Group | Control Group | ||
|---|---|---|---|---|---|
| No. of patients Gr. | % | No. of patients Gr. B (n=30) | % | ||
| A(n=30) | |||||
| 1 | Veg | 4 | 13.33 % | 5 | 16.67% |
| 2 | Mixed | 26 | 86.67% | 25 | 83.33% |
Table 6: Showing Ahara wise Distribution in 60 patients of bhagandara.
| Sr.no | Prakriti | Experimental Group | Control Group | ||
|---|---|---|---|---|---|
| No. of patients Gr. | % | No. of patients Gr. B (n=30) | % | ||
| A(n=30) | |||||
| 1 | Vata-pittaj | 17 | 56.67 % | 10 | 33.33% |
| 2 | Pittaj-kaphaj | 6 | 20.00% | 5 | 16.67% |
| 3 | Vata-kaphaja | 7 | 23.33% | 15 | 50.00% |
| Sr.no | Bowel habits | Experimental Group | Control Group | ||
| No. of patients Gr. | % | No. of patients Gr. B (n=30) | % | ||
| A(n=30) | |||||
| 1 | Regular | 10 | 33.33 % | 14 | 46.67% |
| 2 | Irregular | 20 | 66.67% | 16 | 53.33% |
Table 7: Showing prakriti pattern distribution in 60 patients of bhagandara.
- Sr no symptoms
- Group A
- Group B
- BT
- AT
- Diff.
- % RELIF
- BT
- AT
- Diff.
- % RELIF
- 1
- Pain on walking
- 86
- 31
- 55
- 64%
- 74
- 3
- 71
- 96%
- 2
- Pain on sitting
- 77
- 19
- 58
- 75%
- 58
- 6
- 52
- 90%
- 3
- Pain during sleep
- 60
- 4
- 56
- 93%
- 24
- 1
- 23
- 96%
- 4
- Duration of pain
- 71
- 28
- 43
- 61%
- 63
- 14
- 49
- 78%
- 5
- Agnimandya
- 52
- 4
- 48
- 92%
- 48
- 60
- -12
- -25%
- 6
- Malapravritti
- 38
- 4
- 34
- 89%
- 49
- 32
- 17
- 35%
- 7
- Mutrapravritti
- 12
- 3
- 9
- 75%
- 9
- 1
- 8
- 89%
- 8
- Gastric Irritability
- 32
- 12
- 20
- 62%
- 30
- 45
- -15
- -50%
- 9
- Pus discharge
- 49
- 5
- 44
- 90%
- 52
- 6
- 46
- 89%
- Average score
- 53
- 12.22
- 40.77
- 77.885
- 45.22
- 18.66
- 26.55
- 55
Table 8: Table showing effect on Symptoms Score of 60 Patients of Bhagandara.
| Sr.no | Bowel habbits | Experimental Group | Control Group | ||
|---|---|---|---|---|---|
| No. of patients Gr. | % | No. of patients Gr. B (n=30) | % | ||
| A(n=30) | |||||
| 1 | Shataponak | 2 | 6.67% | 1 | 3.33% |
| 2 | Ustragriva | 10 | 33.33% | 15 | 50.00% |
| 3 | Paristravi | 18 | 60.00% | 14 | 46.67% |
| 4 | Sambukavarta | 0 | 0.00% | 0 | 0.00% |
| 5 | Unmargi | 0 | 0.00% | 0 | 0.00% |
Table 9: Table showing effect on Symptoms Score of 60 Patients of Bhagandara.
Effect of therapy on symptoms score
Overall, it was shown that Group A (77.88 percent) had more alleviation than Group B. (55.00 %). In this series,
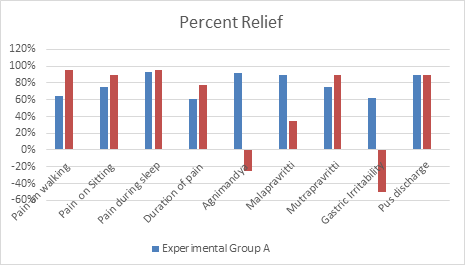
every symptom was examined in the manner shown in the table. In Group A, there is a greater percentage of remission from sleep-related discomfort symptoms.
Discussion
Comparative Clinical Efficacy of Katutrikadya Churna in the Management of Post-Operative Care W.S.R to Bhagandara: was the title of a study that was conducted. On the basis of observations made in the form of tables and graphs and in- depth discussion in the preceding chapters, the following conclusions can be taken at the end of the research.
- The age range of 18 to 39 years was shown to have a higher incidence of bhagandara (Fistula-in-ano) and a lower incidence in the age range of 40 to 60 years. This study’s average age of 35 demonstrates that Bhagandara is more common in middle age. More exposure to the etiological variables for Bhagandara might be the cause. The sickness of middle age is bhagandara (fistula-in- ono), according to literature.
- More males than females were found to have Bhagandara. This may be due to the fact that males are more likely than females to have anal glands. The social structure of the society may also have contributed to this outcome. Additionally, according to the literature, fistula in-ano occurs less frequently seen in females as compared to male. (Goligher).
- Patients who followed a mixed diet had more symptoms than those who were vegetarians only, according to Diet Wise Distribution. Spicy foods are typically preferred by patients on mixed diets, which may encourage excessive effort and worsen discomfort. Less patients were engaged in sedentary employment, while the majority of patients were engaged in active labour. The Vata dosha, which encourages discomfort, is increased by physical work.
- Patients with vata pittaj prakriti were more prevalent in the research, followed by those with Vata kaphaj and Pitta kaphaj. It demonstrates that after receiving Kshara Sutra, significant Vata Pitta patients have more discomfort. The participation of Prakriti and Dosha may be the cause.
- While some individuals had regular bowel movements, the majority of the patients had irregular bowel movements. Patients with bowel irregularities must strain when defecating, which hurts and makes them more vulnerable to anal gland infection, which results in Bhagandara.
- Paristrvi bhagandara was the most common treatment, followed by ushtragriva bhagandara, with very few patients receiving shataponak bhagandara and none receiving shambukavarta or ummargi bhagandara [10].
Effect of Therapy
- In pain on walking: The percent relief in pain on walking by katutrikadya churna was 64% and that of diclofenac sodium was 96%. That means that both the drugs are effective in pain on walking but diclofenac sodium is more potent than katutrikadya churna for the symptom.
- In pain on sitting: The percent relic in pain on sitting by katutrikadya churna was 75% and that of diclofenac sodium was 90%. It means that both the drugs are effective in pain on silting but diclofenac sodium is more potent than katutrikadya churna for the symptom.
- In pain during sleep: The percent relief in pain during sleep by katutrikadya churna was 93% and that of diclofenac sodium was 96%. It means that both the drugs are effective in pain during sleep but diclofenac sodium is more potent than katutrikadya churna for the symptom.
- In duration of persistence of pain: The percent relief in persistence of pain by katutrikadya churna was 61% and that of diclofenac sodium was 78%. It means that both the drugs are effective in duration of persistence of pain but diclofenac sodium is more potent than katutrikadya churna for the symptom.
- Agnimandya: The percent relief in agnimandya by katutrikadya churna was 92% and that of diclofenac sodium the symptom is increased by 25%. It means that both katutrikadya churna is reducing agnimandya whereas diclofenac sodium is increasing agnimandya.
- Vatanuloman: The percent relief in malapravritti and mutrapravritti by Katutrikadya churna was 89% & 75% respectively whereas that by Diclofenac sodium was 39% & 89%. It means that for vatanuloman property Katutrikadya churna is more potent than Diclofenac sodium.
- Gastric irritability: The percent relief in gastric irritability by katutrikadya churna was 62% whereas there is increase in the symptom by 59% by diclofenac sodium.
- Pus discharge: The percent relief in Pus discharge by katutrikadya churna was 90% and that of diclofenac sodium was 89%. It means that both the drugs are about equally effective for the symptom.
- Probable Mechanism of Katutrikadya Churna’s pain- relieving effects: Guru, ushna, and snigdha drays’ are the main ingredients of Katutrikadya Churna, which would lessen the elevated vata dosha. Additionally, because of its vatanuloman function, it lessens constipation, which lessens straining during urination, one of the factors contributing to discomfort. Additionally, it raises jatharagni. Due to the sangyasthapan feature of vacha, it also lessens pain intensity and avoids a condition of shock brought on by extreme pain.
Conclusion
According to the findings of the current study, katutrikadya churna is a potent vedanasthapan aushadhi (analgesic) for discomfort that develops over the anal area when bhagandara is treated with kshar-sutra. By possessing agnidipan and vatanuloman properties, katutrikadya churna not only soothes pain but also addresses the primary causes of the ailments, namely agnimandya and malavarodha. It also lessens pus discharge and irritation. Additionally, unlike the modern allopathic painkiller (Diclofenac sodium), it does not cause stomach irritation. (With the exception of people who already have hyperacidity and other irritable stomach issues).
References
-
Shastri KA (2007) Sushruta Samhita of Maharishi Sushruta. Chaukhambha Bharati Academy, Uttarsthan, Varanasi, India, pp: 92.
-
Yadavai Trkam (2008) Yadavai Trkam Acharya Ashtanga Hridaya Arunadatta. Hemadri commentary, Chaukhamba Sanskrit Pratishthan, Uttarasthana, Varanasi, India, pp: 754.
-
(2004) Madhava Nidana. Part 2, Nidanasthana, pp: 210.
-
(2005) Bhavaprakasha. Madhya khandam, pp: 657.
-
(1993) Yogaratnakar. 5th(Edn.), Uttarardha, Ksudrarognidanam, pp: 273.
-
Acharya YT (2003) Charaka Samhita with chakrapani Ayurveda dipika commentary. Vol. 1, Sutra Sthana, Chaukhambha Surhartai, Varanasi, India, 1: 78.
-
Chakradatta (2002) Kshudrarogadhikara. 4th(Edn.), pp: 315-318.
-
(2005) Bhaishajyaratnavali. 8th(Edn.),Kshudra roga Chikitsa, pp: 956.
-
Shastri KA (2007) Sushruta Samhita of Maharishi Sushruta. Chaukhambha Bharati Academy, Uttar sthan, Varanasi, India, pp: 465.
-
Acharya YT (2008) Ashtanga Hridaya Arunadatta- hemadri commentary. Chaukhama Sanskrit Pratisthan, Uttarasthana, Varanasi, pp: 756-758.
- Management of Ear Keloid with Ksharsutra: A Case Study
- Yoga and Global Sustainability: A Holistic Path to One Earth, One Health
- Autoimmune Diseases in Ayurveda: A Narrative Review with Classical and Modern Perspectives
- Management of Cluster Headache Associated with Pituitary Apophysitis by CERT (Chakrasiddh Energy Release Technique): A Case Report on Energy Rebalancing
- Zygophyllum Geslini Coss : Biochemicals and Antioxidant Activity
- Observations of a Beginner Vaidya