Detection of Plasmodium Falciparum and Pfmdr Gene Among HIV Patients Attending Clinic in a Tertiary Hospital in South-South Nigeria Using a Nested PCR Technique
In this study, the prevalence rate of falciparum malaria, the risk factors associated with HIV and CD4 count level in association with malaria parasite were determined while the Pfmdr mutant resistant gene of falciparum species was detected in HIV patients attending Clinic in a Tertiary Hospital in South-south Nigeria. Subjects were purposively selected as they came for treatment and screened for falciparum malaria. Of the 67 subjects enrolled in the study, 35% were HIV positive adults, while 32% were HIV negative adults (Controls). They were in the age range of 20-56 years with a mean age of 34.84±9.86 standard deviation (SD). Out of 35 HIV adult patients, 25%t of the HIV patients were on treatment for HIV and other opportunistic infections. Twenty-one percent admitted that they took anti-malaria drugs every three months, 31% attested to the use of long lasting insecticide treated nets while 4% did not use treated nets. Microscopic examination revealed 5.7% of falciparum malaria, while Nested PCR detected 8.7% falciparum malaria in the DNA extract sample of these patients. A total of five HIV positive patients were infected with falciparum malaria, giving a prevalence rate of 14.2% of co-infected patients with malaria parasite. None of the HIV negative subjects had falciparum malaria. This is probably due to their regularly sleeping under long lasting insecticide treated nets. There was no significant difference between malaria parasite infection by gender (P = 0.88), age group (P=0.17), and CD4+ count (O.R:1.0, P=0.81). Plasmodium falciparum multidrug resistant gene (Pfmdr) analysis did not undergo mutation. Based on the result it is recommended that HIV patients regularly sleep under long lasting insecticide treated nets. There is need to improve the quality of health care, especially as regards malaria prevention and treatment offered to HIV patients.
Introduction
Malaria and HIV constitute major public health challenges to developing African countries [1]. Sub-Saharan Africa has the most serious HIV and AIDS epidemic in the world [2]. In 2013, an estimated 24.7 million people in Africa were living with HIV, accounting for 71% of global total [3]. In the same year, there were an estimated 1.5 million new HIV infections and 1.1 million AIDS related deaths [4] while in 2015, there were about 214 million malaria cases that led to 438,000 deaths [5].The geographical overlap in sub-Saharan Africa and South America has led to similarities in co-infection with Plasmodium and HIV, this results in the quick progression and severity of both diseases particularly among the poor, and contributes to the poverty of sub-Saharan African nations by taking a toll on young people who contribute greatly to the workforce of the economy [6]. These two infectious diseases have been documented to account for massive morbidity and mortality rates in sub-Saharan Africa [3].
Malaria and Human Immunodeficiency Virus (HIV) often coexist in patients in many parts of the world due to geographical overlaps of these two diseases. Presently, most data on HIV infection with malaria are derived from P. falciparum endemic regions of sub-Saharan Africa, Nigeria inclusive. These two infections interact bi-directionally and synergistically with each other. Thus, HIV infection can increase the risk and severity of malaria infection and parasite burden which may facilitate higher rates of malaria transmission. Individuals in malaria endemic areas are considered semi-immune to malaria and can develop clinical malaria, if they are untreated. Currently, the use of molecular diagnostic procedures in detecting and quantifying the mutant resistant gene of Plasmodium species, especially P. falciparum in HIV positive patients have provided a new set of tools that facilitates both epidemiological investigation and patients’ treatments. However, there is paucity of data on molecular detection of P. falciparum in HIV-infected patients and thus efficient treatment options.
The sensitivity and accuracy of PCR in detecting and quantifying of P. falciparum mutant resistant gene in the human blood is not widely known. Accurate molecular data of P. falciparum have been ignored in most parts of Nigeria. This study was aimed to detect and characterise P. falciparum in patients infected with and without HIV in a Tertiary Hospital in South-south Nigeria.
Methodology
Study Design
This study was a cross-sectional hospital based study consisting of HIV infected adult patients, and non HIV infected adults attending a Tertiary Hospital in South-south Nigeria for treatment.
Study Area
This study was carried out at the HIV Clinic of a Tertiary Hospital in South-south Nigeria. This is one of the testing and treatment Centre for persons infected with HIV in Uyo, Nigeria and is accessed by about 60 clients each day.
Study Population
Persons confirmed to be infected with HIV who consented to participate in this study were included. HIV negative participants were recruited from the General Outpatient Clinic as controls.
Ethical Consideration
Approval from the Ethical Review Board of the Tertiary Hospital in South-south Nigeria was obtained prior to the inception of this research work. Permission was granted by participants through informed consent before the commencement of inclusion in the study.
Collection of Sample
A sterile Multi sample needle was used to draw 5ml of intravenous blood sample into an EDTA Vacutainer glass tubes. A 15-point structured questionnaire was used to collect data on socio-demographic characteristics and risk factors for malaria infection.
HIV testing and CD4+Count
HIV status was confirmed using the Unigold Cassette kit. CD4 was determined by Flow Cytometry using the Counter Machine for CD4+.
Malaria Microscopy
Thick and thin blood films were made on glass microscope slides. Thin films were fixed using absolute methanol and stained with 10% of Giemsa stain. Parasite identification was performed by a WHO Certified Malaria Microscopist.
DNA Extraction and Loci Detection
DNA was extracted by adding 400µl of Genomic Lysis Buffer to 100µl of blood sample and transferred to a Zymo- SpinTM Column in a collection tube. A total of 200µl of DNA Pre-Wash Buffer was added to the spin column and centrifuged at 10,000g x for one minute. The spin column was transferred to a clean micro-centrifuge tube and 500µl elution Buffer was added to the spin column and incubated for 2-5 minutes at room temperature [7].
Pfmdr gene Amplification was carried out sequentially through Primary Nested PCR Technique using Thirty-five (35) PCR tubes and an additional 32 were labelled as controls (HIV Negative) and placed in an Ice rack. A calibrated pipette of 1.0 µl was used to draw up a master mix and transferred to a 1.5µl Eppendorf tube. This was followed by adding 0.4µl Pfmdr primers- (Forward IMDR1/F and reverse R IMDRI/R) 0.5µl Mgcl2, 5mM DNA template and a high molecular grade water of 3.29µl to dilute the other reagent in their correct concentrations. The primary nested PCR final volume (20µl) was taken from PCR cocktail and then transferred into the labelled PCR tubes for amplification by a Bio system PCR machine.
Secondary Nested PCR Technique
All PCR tubes were labelled like that of the Primary stage of Nested PCR and placed in an Ice rack. A calibrated pipette of 12.5 was used to draw up a master mix and transferred to a 1.5µl Eppendorf tube. This was followed by adding 0.2µl Pfmdr primers (Forward IMDR1/F and reverse R IMDRI/R) 0.5µl MgCl2, 0.5µl DNA template, and an 11.1µl High molecular grade water to dilute the other reagent in their correct concentrations. The Primary and Secondary Nested PCR final volume (25µl) was taken from PCR cocktail and then transferred into the labelled PCR tubes for amplification by a Bio system PCR machine. The Secondary PCR process was carried out by using the amplicons from the Primary Nested PCR to carry out the Secondary Nested PCR process to ascertain the desired DNA gene of interest (Pfmdr). Agar gel Electrophoresis was then carried out to separate the DNA gene molecule (Pfmdr) of interest.
Restriction Fragment length Polymerization
A mixture addition of 1µl of Afl iii (Restriction enzyme solution), 1µl of buffer solution, 5µl of Polymerase product and 3µl of high molecular water was calculated to give a 10µl final volume to be used for RFLP experiment before incubation for 3 Hours at 37ºC [8, 9, 10]. DNA from clones 3D7 and Dd2 were employed as controls.
Statistical Analysis
All data were entered into SPSS version 24. The statistical parameters for the analysis of data were Pearson’s Chi- Square Test. All charts were created using Microsoft Excel software application. Sensitivity and specificity of malaria microscopy in comparison with Pfmdr PCR were calculated.
Results
Thirty-five HIV positive and 32 HIV negative patients participated in this study. In all, there were a total of 34 males and 66 females that participated. The risk factors for malaria infection among the participants are shown on Table 1. Among the 100 participants, 22% admitted to the use of insecticide treated nets, while 78% said they used indoor insecticides. Only 72% demonstrated knowledge about importance of clean environment while 83% knew about the aetiological agent of malaria.
| No (%) | Yes (%) | Total (%) | |
|---|---|---|---|
| Use of insecticide treated bed nets | 31(31) | 69(69) | 100 |
| Use of indoor insecticides | 22(22) | 78(78) | 100 |
| Knowledge about clean Environment | 28(28) | 72(72) | 100 |
| Knowledge about etiological agents of malaria | 17(17) | 83(83) | 100 |
| Anti-malarial therapy | 14(14) | 86(86) | 100 |
Table 1: Risk factors predisposing participants to malaria in a Tertiary Hospital in South-south Nigeria.
Table 2 presents the result of CD4+ count level and the prevalence of malaria amongst HIV infected adults. Participants with less than 200µl CD4 count were 13%, which consisted of 4% Males and 9% Females. Two participants tested positive to malaria parasite. Participants with CD4+ count greater than 500µl were 22, and they all tested negative to malaria parasite.
| CD4+ count cells/µL | Total (%) (n=100) | Number of Positive malaria Cases (%) (n=5) | |
|---|---|---|---|
| <200 | 13(13.5) | 2(15.3) | |
| 200-300 | 27(27.0) | 0(0) | |
| 300-400 | 23(23.0) | 0(0) | |
| 400-500 | 15(15.0) | 3(20.0) | |
| >500 | 23(23.0) | 0(0.0) | |
| Total | 100 | 5 | |
| Age Grouping (in years) | Malaria Positive (%) (n=5) | Malaria Positive (%) (n=100) | Total (%) (n=100) |
| 20-29 | 0(0.0) | 42(44.2) | 42(42.0) |
| 30-39 | 3(60.0) | 35(36.8) | 38(38.0) |
| 40-49 | 2(40.0) | 18(18.9) | 20(20.0) |
| >50 | 0(0.0) | 0(0.0) | 0(0.0) |
| Total | 5(100.0) | 95(100.0) | 100(100.0) |
Table 2: Relationship between CD4 count and malaria infection among adult HIV adult patients in a Tertiary Hospital in South- sou
Table 3 presents the prevalence of malaria according to age range. Age range of 20-29 was all negative.
Table 4 presents the prevalence rate of malaria parasite according to Marital Status. All the single women tested negative to malaria, while five married participants were positive to malaria parasite.
| Males (%) | Females (%) | Number of Positive Cases (%) | |
|---|---|---|---|
| Single | 0 | 0 | 0 |
| Married | 2(40.0) | 3(60.0) | 5(100.0) |
| Widow | 0 | 0 | 0 |
| Widower | 0 | 0 | 0 |
| Total | 2 (40.0) | 3(60.0) | 5(100.0) |
Table 3: Prevalence rate of malaria based on marital status in a Tertiary Hospital in South-south Nigeria.
Figure 1 represents an Agar gel electrophoresis used to determine the presence and the migration of Plasmodium falciparum multi drug resistance (pfmdr) gene. Lane11, 21, c
23, 24, 30 all showed visible bands after examined with an Ultra violet transilluminator. Dd2 and 3d7 are the mutant and Wild type controls, respectively.
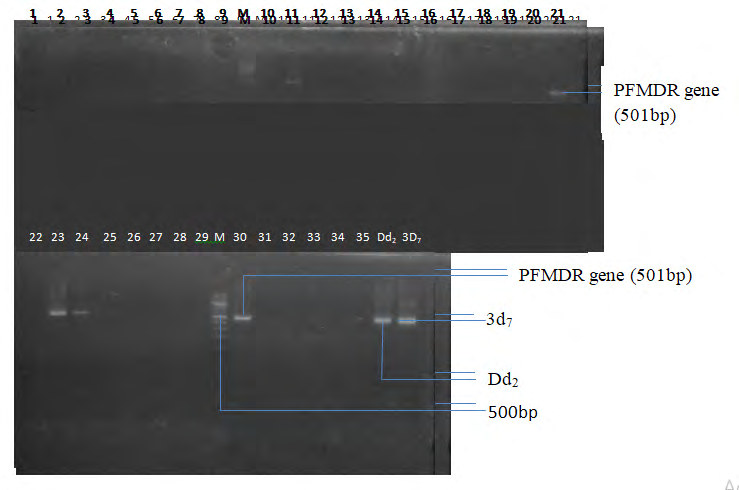
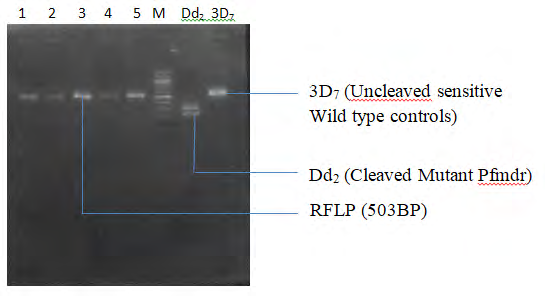
Figure 2 represents the Restricted Fragment Length Polymorphism of Pfmdr gene, after an Afl iii enzyme digestion. Lane1 to Lane 5 were all un cleaved wild type PFMDR gene. Lane M represents the Quick-Load 100bp molecular ladder. Lane Dd2 represents the cleaved mutant PFMDR while 3D7 represents the un cleaved sensitive Wild type controls, respectively.
Discussion
Recent studies have shed light on the link between HIV and malaria and the potential public health implications of co-infection [11]. Human Immunodeficiency Virus (HIV) infected adults in malaria endemic areas are at increased risk of contracting malaria, as HIV infection increases the incidence and severity of clinical malaria. The infection has been found to roughly double the risk of malaria parasitaemia in clinical malaria [12]. In this study, involving 35 HIV positive adult patients and 32 HIV negative adult participants attending a Tertiary Hospital in South-South Nigeria, five positive cases of falciparum malaria were detected in HIV positive adult patients, while 32 HIV negative adult participants were negative to falciparum malaria. The prevalence rate of falciparum malaria among HIV positive patients in this study was 14.2%. A lower prevalence rate of 2.11% was obtained in a cohort study of HIV infected patients in Benin City, Nigeria by Akinbo, et al. [13]. A higher prevalence rate of 45.4% was recorded among HIV positive adult patients in Sokoto, North-western Nigeria by Unata, et al. [14]. The possible reason for the prevalence rate obtained in this study when compared to that of Unata, et al. [14] may be due to consistent intake of ACTs by these HIV patients. In this particular study, 21% of HIV positive adult patients admitted to have taken ACTs most times whenever signs and symptoms of malaria arise. However, five of these patients who took ACTs most times still had re-occurrence of malaria parasite, which might be because of the daily intake of Anti- retroviral drugs by these patients. This might have interfered with the drug action of ACT drugs against malaria parasite. Studies have shown that artesunate and artemether are metabolized to dihydroatemisinin by CYP3A4 and this may decrease concentrations and anti-malarial efficacy – CYP3A4, especially in antiretroviral drugs like Nivrapine. This can be seen as a treatment failure of these Anti-malarial drugs due to interference by anti-retroviral drugs [15].
HIV positive subjects within the age group 30-39 years were mostly affected by the falciparum malaria, 3(8.5%) subjects, while the least affected age group was 40-49 years with 2(5.7%) subjects. This could be because the patients within this age bracket are very active outdoors, and also preferred staying out late at night. This agrees with the findings obtained in a study carried out in Kaduna by Abioye, et al. [16], who also reported a high prevalence rate in the same age group. There was no significant difference between age, gender/pregnancy and increase in incidence of parasitaemia among these patients. Therefore, the null hypothesis is accepted. Thus, there is no significant relationship between age (χ2 = 6.13, df = 3, P = 0.17), gender (χ2 = 0.02, df = 1, P = 0.88) /pregnancy and parasitaemia among HIV patients. Of the five positive malaria cases detected, 8.5% were females and 5.7% were males. This apparently showed that females were mostly affected by the parasite. This is similar to the result obtained by Abioye, et al. [16] who reported a prevalent rate of 65.4% among females. The high prevalence of malaria parasite in females could be as a result of malaria transmission determined in large part by social, economic and cultural factors, which intersect with sex-specific and gender-specific vulnerabilities to impact women’s ability to prevent malaria infection. Women’s traditional household roles, such as cooking the evening meal outdoors or waking up before sunrise to prepare the household for the day, may also put them at greater risk of malaria infection [17].
Investigation on risk factors of malaria parasite in HIV patients in this study showed that there was no significant difference in relationship between the level of CD4+, gender, and age group and malaria parasite. Subjects in this study were aware of the outcome of malaria illness if exposed to mosquito bites indoors and outdoors. Of the subjects in this study, 31% adhered to the usage of long lasting insecticide treated nets. This can be compared to a study in Bamenda, Cameroun that reported the use of long lasting insecticide treated nets amongst HIV positive infected adults to be 28.8% based on good sensitization on using long lasting insecticide treated nets [17]. The non-utilization of long- lasting insecticide treated bed net by four HIV positive adult patients is also a reason for the transmission of falciparum malaria. These four subjects did not sleep under insecticide treated nets and complained that they were not comfortable with bed nets because they felt it caused body heat thus affecting their sleep at night.
Two subjects with lesser CD4+ count of <200 cells /µl had malaria parasite, while three other subjects with CD4+ counts ≥ 400 cells/µl also had malaria parasite. The patients in our study followed the HAART regimen (Lamivudine, Tenofovir and Efavirenze) which helped increase the CD4+ count of more than half of the subjects. This explained why the results showed no significant relationship between low CD4+ T-cell count and increased parasitaemia in these patients (χ2 = 0.056, df = 1, P = 0.81). Hence, the null hypothesis is accepted which states; there was no significant difference between low CD4+ T-cell counts and increased parasitaemia. This is because both subjects that had higher and lesser CD4+ of <200 cells /µl counts had parasitaemia in the peripheral blood. This is dissimilar to that obtained in a study by Chavale, et al. [18], which showed that there is a significant relationship between high amount of parasitaemia and decreased CD4+ T-cell count in HIV positive patients. A possible reason for this difference could be that patients in the former study were neither taking antiretroviral nor anti-malaria drugs. This situation gets worse if both diseases are left untreated. This explains the significance of lower CD4+ T-cell count and high amount of parasitaemia in the study by Chavale, et al. [18].
Method of diagnosis of malaria using microscopy continues to be the gold standard for laboratory confirmation [19]; however, a molecular technique, Nested Polymerase Chain Reaction (PCR) was used in this study. This technique detected three positive cases compared to two cases earlier detected through microscopy. This was not surprising because Nested PCR was more sensitive and accurate than thick and thin film smears [20]. The Nested PCR has been reported to be preferable to other PCR techniques because the target sequence would be more abundant than the original solution before the first PCR is performed [21].
Molecular analysis of the five positive falciparum parasites detected from the blood and DNA extract samples of the HIV positive patients, showed the presence of P. falciparum multidrug resistance (Pfmdr) genes. These are expressed as visible lanes on an Agarose gel electrophoresis slab after Pfmdr gene amplification by Nested PCR technique. Lanes without bands did not have the Pfmdr genes. The visible lanes (11, 12, 23, 24, and 30) on the agarose gel slab were analysed by an Ultraviolet transilluminator (Figure 1). The molecular weight of the Pfmdr genes was 501bp as revealed by Agarose Gel Electrophoresis. The five lanes were all uncleaved wild type Pfmdr gene. This study showed that there were no breaks in the lanes (11, 12, 23, 24, and 30), all five lanes maintained a base pair size of 501bp after conducting a Restriction Fragment Length Polymorphism test (Figure 2). Inferences drawn from these mean that though the Pfmdr genes were detected, they did not express mutation after inoculating Afiii restricted enzyme as a digestive marker for mutation detection. The detection of five successful unmutated positive Pfmdr gene was dissimilar to that of a previous study by Folarin, et al. [22], who reported the presence of point mutation by Pfmdr_1 N86Y as mutant alleles in 33% of isolate in South-west Nigeria. The possible reason of unmutated _Pfmdr detected in this present study, could be that Pfmdr_1 was not responsible for the re- occurrence of _falciparum malaria, but this re-occurrence may be due to chance or the presence of another resistant gene.
Conclusion
In conclusion, this study revealed that prevalence rate of malaria in HIV patients as co-infection at a Tertiary Hospital in South-south Nigeria was high. Majority of the patients had healthy CD4+ count levels which helped to prevent them from illness such as falciparum malaria. Subjects with lower CD4+ of 200cells/µl were associated with an increased risk of having malaria parasite. Though females had more positive cases, males were likely to have more parasitaemia in the peripheral blood.
Molecular analysis revealed that the Pfmdr gene in the P. falciparum did not undergo mutation. This brings us to the question, is there no mutation by Pfmdr or is there another gene that is responsible for the re-occurrence of malaria parasite in the positive malaria cases in this study? This also could mean that, there is a possibility of an interference of anti-malaria drug treatment.
Acknowledgement: Technical Assistance offered by Mr. Samuel Anietie in Medical Microbiology Laboratory, University of Uyo Teaching Hospital (UUTH), Uyo.
References
-
Nwauche CI (2014) Malaria/HIV Interaction in Nigeria-A Review. Nigerian Health Journal 14(3): 97-106.
-
Averting HIV and AIDS (2016) HIV and AIDS in Sub- Saharan Africa Regional Overview.
-
Blair C (2015) Co-Morbidity of HIV and Malaria. pp: 1-6.
-
(2014) The Gap Report. UNAIDS.
-
(2016) UNICEF Data: Monitoring the Situation of Children and Women.
-
Hochman S, Kim K (2009) The Impact of HIV and Malaria Co-Infection: What is known and Suggested Viruses for Further Study. Interdiscip Perspect Infect Dis 617954.
-
Uni-gold (2017) Procedure for HIV Testing.
-
(2016) University of Uyo Teaching Hospital Safety Operation Procedure. CD4 T-cell enumeration. Antretroviral therapy laboratory Specimen Testing Document, ST-SOP-3, pp: 7-3.
-
Srinivas K (2019) Malaria Testing.
-
Zymo Research Corp (2016) Protocol Manual Quick g-DNATM MiniPrep.
-
Longdoh AN, Henri LFK, Nsagha DS, Jules CNA, Kwenti TE (2012) Low Malaria Prevalence in HIV-Positive Patients in Bamenda, Cameroon. Journal of Microbiology Research 2(3): 56-59.
-
Pantanik P, Jere CS, Miller WC, Hoffma IF, Wirima J, et al. (2005) Effects of HIV-1 RNA Concentration and CD4+ Cell Count on the Incidence of Malaria Infection in a Cohort of Adults in Rural Malawi. J Infect Dis 192(6): 984-991.
-
Akinbo FO, Omoregie R (2012) Plasmodium falciparum Infection in Highly Active Antiretroviral Therapy (HAART) in Benin City, Nigeria. J Res Health Sci 12(1): 15-18.
-
Unata IM, Nura MB, Olasumbo FA, Aminu A, Nafiu F (2015) Prevalence of Malaria Parasites among HIV/AIDS Patients Attending HIV Clinic in Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria. International Journal of Novel Research in Life Sciences 2(2): 39-43.
-
Fehintola FA, Maponga CC, Adewole IF, MA Q, Morse GD, et al. (2011) Drug Interaction in Treatment and Chemoprophylaxis of Malaria in HIV Infected Individuals in Sub-Saharan Africa. Curr Drug Metab 12(1): 51-56.
-
Abioye JOK, Adullahi DK, Ako AA (2014) Prevalence of Malaria among HIV Patients in 44 Nigeria Army Reference Hospital Kaduna (44 NARHK). International Journal of Advanced Biological Research 4(4): 412-415.
-
United Nations Development Programme (2015) Discussion Paper. Gender and Malaria: Making the Investment Case for Programming that Addresses the Specific Vulnerabilities and needs of both Males and Females who are affected by or at Risk of Malaria.
-
Chavale H, Santos Oliveria JR, Da Cruz AM, Enosse S (2012) Enhanced T-Cell Activation in Plasmodium falciparum Malaria-Infected Human Immunodeficiency Virus-1 Patients from Mozambique. Mem Inst Oswaldo Cruz 107(8): 985-992.
-
(2016) Malaria Diagnostic Tests. Centres for Disease Control and Prevention.
-
Bourgeois N, Boutet ABD, Bousquet PJ, Douard EH, Charachon S, et al. (2010) Enhanced T-Cell Activation Activation in Plasmodium Species Infection. Clin Microbiol Infec 16: 1305-1311.
-
Hafez HM, Hauck, R, Luschow D, McDougald L (2005) Comparison of the Specificity and Sensitivity of PCR, Nested PCR, and Real-Time PCR for the Diagnosis of Histomoniasis. Avian Dis 49(3): 366-370.
-
Folarin OA, Gbotoscho GO, Sowunmi A, Olorunsogo OO, Oduola Am, et al. (2008) Chloroquine Resistant Plasmodium falciparum in Nigeria: Relationship between Pfcrt and Pfmdr1 Polymorphisms, In-Vitro Resistance and Treatment Outcome. Open Trop Med J 1: 74-82.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda