Impact of Lebanese Accreditation Process on Hospital Profitability: Case Study
Accreditation has become a significant feature in health care systems worldwide and a quality improvement tool that enhanced its standing in the health sector. It played a role in developing the quality of care and patient safety, nevertheless, the accreditation process implies an important financial burden on healthcare institutions. The purpose of this study is to identify the impact of Lebanese accreditation on hospital profitability by analyzing costs of accreditation, its impact on staff using SEAM (Socio-Economic Approach of Management) approach, and its influence on patient satisfaction. This study was designed to be qualitative: the first part of the study is interventional. Interviews in a hospital in Lebanon were done with staff from all levels and departments. The second part is related to the comparison of financial indicators (return on investment and contribution margin per hour), number of patients, and their satisfaction rate before and after accreditation (2010-2012). The results presented a considerable financial weight for accreditation. Lebanese accreditation has led to a positive impact on hospital profitability through quality of care increasing patient satisfaction, leading to patient retention and acquisition. On the other hand, accreditation has also manifested a negative effect on the health of staff by stressing them out through the heavy workload.
Introduction
Accreditation became an essential element in health care systems: a trademark of quality [1]. Its potential to strengthen the qualification of care has been recognized worldwide, added to its competing strategy in the health sector [2].
Healthcare accreditation has enhanced its position over the past few years [3]. An external assessment process to determine if the organization meets a set of standards settled to improve quality of care, attained by the government in some nations (France, Lebanon) or by independent accrediting agencies in others (United States, Canada) [4, 5].
Many benefits from healthcare accreditation are claimed: organizing and strengthening patient safety and quality of care, enhancing community confidence in treatment and services, contributing in the competitive marketplace, developing risk management and reduction, decreasing liability insurance costs, enhancing staff safety and development, providing tools to strengthen organizational structure and management and look after a high quality of performance [6].
Lebanon is a middle-income Mediterranean country populated by almost 4.5 million citizens and residents. After the civil war that damaged the country in 1970s, the Lebanese government engaged considerable efforts on the health system [7]. The growth of the health sector, rapidly leading to further increase of the hospital sector happened in an uncontrollable aspect, resulting in an excess of services diffused over 136 private hospitals and 28 public hospitals.
In 1999, the national hospital accreditation program has been set by the Ministry of Public Health (MOPH), derived from different accreditation programs adapted in developed countries such as Canada, USA, Ireland, France, Australia, New Zealand and UK. Three national surveys were done by the Ministry of Public Health: Survey I between September 2001 and July 2002 with 47 accredited hospitals, Survey II in 2004 with 85 accredited hospitals, and Survey III in 2011. In the second and the third surveys, hospitals were more anticipated and more familiar with the requirements and procedures, with 128 accredited hospitals in Lebanon. The implementation of accreditation in the healthcare organizations encouraged the initiation of a quality improvement environment, quality assurance, and risk management [1].
Accreditation imposes on hospitals an important financial burden: starting from planning for a survey and through all the process. The preparations of the hospital in order to comply with the standards have considerable costs [1].
Another classification of costs is suggested with two categories: visible and hidden costs. Visible costs or “standard costs” are expenses spent on quality improvement actions. According to a previous study in Lebanon, the sections of preparations imposing the highest increase of costs are the following: maintenance of infrastructure and new equipment. Upgrade of available property, recruitment and orientation of new staff, training of current and new staff, salary adjustments, and benefits admitted to staff, housekeeping services, laundry services, dietary services, administrative services, and consultant costs [1].
On the other hand, hidden costs corresponding to the second category of costs are introduced by the Socio Economic Approach to Management by Henry Saval and his colleagues. SEAM is founded since 1973, established in the Socio-Economic Institute of Firms and Organizations Research (ISEOR) in Lyon, France. It’s a mode of management, which includes management methods prioritizing the organization’s human development for a short and long term efficiency and persistence. It provides a methodic way to evaluate the hidden costs in the institution, while recognizing such costs is not usually practiced in management systems. It’s an association between the social condition of an organization and its economic performance [8].
In 2010, SEAM was introduced in Lebanon and implemented in three hospitals, belonging to the same religious order of Catholic Sisters. The first hospital was a middle-sized hospital with 460 employees, 150 physicians and 180 beds; the second was also a middle-sized hospital with 300 employees, 150 physicians and 150 beds, while the third hospital was a small-sized hospital with 240 employees, 100 physicians and 66 beds. Their accreditation level was identical with class A; aside political and economic instabilities in the country mentioned previously. The health care systems were affected by external and internal challenges: the complexity of the health care systems, the demographic changes in the Middle East, the differences of cultures and patients demands, the competition in the health sector on a regional and national level. The load of facing these challenges leads to multitude of dysfunctions [9].
A healthcare organization’s strength is related to profit and return on investment and the efficiency of its management. As a measure of success, profitability is essential in the health market today: in order to endure, a hospital must earn profit. Profits give the organization favorable circumstances to succeed and avoid failure. “Profit is like health. You need it, and the more you have the better. But it’s not why you exist”.
Profitability indicators support the measurement of financial return needed for assets replacements [10]. The first type of profitability indicators includes margins and returns on assets/investment.
Over the past years, patient satisfaction has become an important element of measurement of the quality of care in the health care sector: a quality dimension [11]. It has an important role in reflecting patient’s perceptions of the way the delivery of care met their expectations [12].
When patients give their opinion in any service that they had encountered, they are automatically evaluating the quality of care [13]. High quality resulting in high satisfaction will induce the attraction of new patients, the retention of current patients and in some cases the persuasion of other hospital’s patients. When patients reveal a positive assessment and effective impressions to others, they recommend the healthcare services to their friends and relatives. This word-of-mouth advertising technique is highly important for the health care organizations. Satisfied patients recommending a specific hospital with positive intentions is an influential source of information in health care marketing [14].
Accreditation represents today a significant tool for quality improvement in the health care sector. It offers beneficial development of the structure, process, and outcome in health care organization. In Lebanon, the healthcare system introduced accreditation in 2001, followed by two consecutive national surveys in 2004 and 2011. The MOPH installed a reimbursement system for hospitals, representing a financial inducement for hospitals in Lebanon. Therefore, preparations for accreditation have an important financial burden in order to comply with the standards. The expenses of accreditation are classified in two categories: visible and hidden costs. Hidden costs, according to SEAM approach are related to specific dysfunctions in the organization, while visible costs represent the areas where expenses are the highest.
Improvements of quality of care engender patient satisfaction, leading to patient retention and acquisition, highly related to hospital profitability.
Methodology
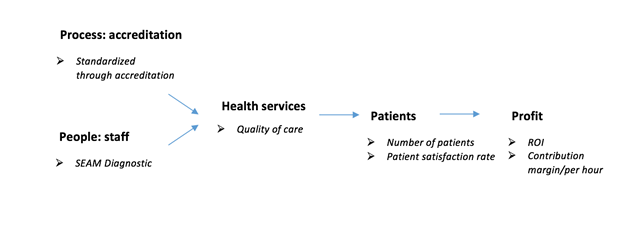
The methodology of this study is interventional and qualitative. The interventional process was done in a private, middle sized university hospital in Lebanon with 220 beds. The diagnostic phase according to SEAM intervention. The second part of the study is a comparison of the profitability represented by costs and revenues, a year before and a year after accreditation to perceive if it has an impact of increase or decrease (Figure 1).
The diagnostic process through interviews is done on a sample of 15 people in the hospital. The selection of the people covered all levels employee from strategic management, to supervisory management and staff from different departments: board of directors, therapeutic services, diagnostic services, information services and support services. The duration of the interviews was between 30 minutes to 1 hour. The interviews were based on open questions focusing on working conditions, dysfunctions, and issues faced by the institution during the last accreditation process in 2011. The diagnostic intervention reflects the impact of accreditation on healthcare workers that will automatically affect the productivity.
Therefore, the financial indicator affected consequently by staff productivity is the contribution margin per hour: a profitability measure corresponding to payment to the hospital minus variable costs. As a first measure of profitability, the contribution margin per hour will be compared a year before accreditation, during accreditation and a year after it: from 2010 to 2012.
Patient satisfaction represents a key parameter reflecting quality of care in a healthcare institution; therefore, a comparison of patient satisfaction rate and number of patients from 2010 to 2012 is done, in order to determine an increase or decrease due to accreditation. In addition, a comparison of number of patients is done from 2010 to 2012, with verification of the patient mix and the identification of refugees.
According to a previous study done in Lebanon, the highest expenses of accreditation were on the following areas: infrastructure maintenance, new equipment, available property upgrade, recruitment of new staff, training of current staff, salary adjustment, administrative services, dietary services, staff benefits, housekeeping services, laundry services and consultant costs. These costs of accreditation will be evaluated in this study.
Results
Seam Results
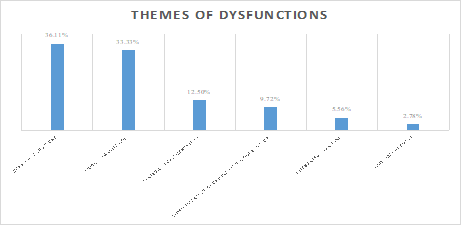
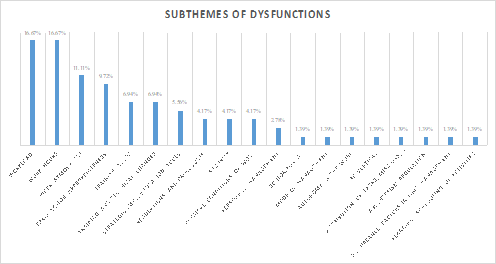
As shown in figures 2 and 3, 36.11% of the dysfunctions during the accreditation phase are related to working conditions with 11.11% work atmosphere, 16.67% work hours, 4.17% security and 4.17% physical conditions of work. In addition, 33.33% of the dysfunctions are related to work organization with 16.67% of workload, 4.17% regulations and procedures, 1.39% autonomy in the work, 1.39% distribution of tasks, missions, functions, and
1.39% absenteeism regulation. Furthermore, 12.5% of the dysfunctions refer to strategic implementation with 5.56% strategic implementation tools, 2.78% personnel management, and 1.39% modes of management. While the dysfunctions associated with communication-coordination- cooperation represent 9.72%, dysfunctions relevant to integrated training represent 5.56%. Finally, 2.78% of dysfunctions concern time management [15].
Financial Results
Costs of accreditation
| 2010 | 2011 | Total(LBP) | Total($) | |
|---|---|---|---|---|
| Infrastructure maintenance | LBP 302,602,134 | LBP 714,637,474 | LBP 1,017,239,608 | $676,941.22 |
| New Equipment | LBP 2,892,835,909 | LBP 809,091,989 | LBP 3,701,927,898 | $2,463,517.52 |
| Available property upgrade | LBP 511,049,005 | LBP 750,565,114 | LBP 1,261,614,119 | $839,564.83 |
| Recruitment of new staff | LBP 20,535,000 | LBP 15,755,000 | LBP 36,290,000 | $24,149.86 |
| Training of current staff | LBP 33,311,977 | LBP 23,637,000 | LBP 56,948,977 | $37,897.77 |
| Salary adjustment | LBP 245,511,000 | LBP 203,445,000 | LBP 448,956,000 | $298,766.21 |
| Administrative services | LBP 92,717,933 | LBP 78,356,098 | LBP 171,074,031 | $113,844.43 |
| Dietary services | LBP 114,682,619 | LBP 277,395,211 | LBP 392,077,830 | $260,915.56 |
| Staff benefits | LBP 149,359,250 | LBP 154,533,750 | LBP 303,893,000 | $202,231.31 |
| Housekeeping services | LBP 139,214,848 | LBP 245,782,802 | LBP 384,997,650 | $256,203.92 |
| Laundry services | LBP 203,458,500 | LBP 225,305,000 | LBP 428,763,500 | $285,328.73 |
| Consultant costs | LBP 67,808,109 | LBP 42,461,250 | LBP 110,269,359 | $73,380.82 |
| Total | LBP 4,773,086,284 | LBP 3,540,965,688 | LBP 8,314,051,972 | $5,532,742.18 |
| Total ($) | $3,176,340.00 | $2,356,402.19 |
Table 1: Costs of accreditation in 2010 and 2011.
According to a previous study done in Lebanon, the areas that had a great impact on the cost of accreditation with the highest financial burden are represented in table 1. The infrastructure maintenance had a total cost $676,941.22 during the preparation period for accreditation (2010-2011). However, new equipment represented the highest expense, which cost 2,463,517.52$. The upgrade of the available property required $839,564.83. Concerning the recruitment of new staff, the costs were $24,149.86, and the training of current staff cost $37,897.77. The salary adjustment that includes all the overtime spent by the employees at work cost $298,766.21. The expenditures of administrative services were $113,844.43. The dietary services required $260,915.56, in addition to the housekeeping services that cost $256,203.92. The expenses on staff benefits had a value
Contribution margin/hour
of $202,231.31. The laundry services cost $285,328.73. Finally, the consultant costs were $73,380.82.
Overall, the accreditation process has a total cost of 5,532,742.18$ for both years 2010 and 2011 (Table 2).
Return on investment
| 2010 | 2012 |
|---|---|
| 21.50% | 24% |
Table 2: Return on investment of the hospital in 2010 and 2012. As shown in table 3, in 2010 the return on investment was 21.5%;
| 2010 | 2012 | |
|---|---|---|
| Revenue | LBP 18,338,552,000.00 | LBP 25,225,643,385.00 |
| Variable costs 1 | LBP (12,550,788,000.00) | LBP (18,815,032,835.00) |
| Variable costs 2 | LBP (16,738,050.00) | LBP (41,346,249.00) |
| Contribution margin (LBP) | LBP 5,771,025,950.00 | LBP 6,369,264,301.00 |
| Contribution margin ($) | $3,814,419.62 | $4,209,831.48 |
| Contribution margin/Hour | $35.46 | $39.13 |
Table 3: Contribution margin per hour of the hospital in 2010 and 2012.
As shown in table 4, the contribution margin increased from $3,814,419.62 in 2010 to $4,209,831.48 in 2012. Consequently, the contribution margin/hour increased by 3.67$ from 35.46$ in 2010 to 39.13$ in 2012.
As shown in table 5, the number of patients increased by 1617 patients from 12,100 in 2010 to 13,717 in 2011. It increased again by 2245 patients from 13,717 in 2011 to 15,962 in 2012.
Patient satisfaction rate/Number of patients
| 2010 | 2011 | 2012 | |
|---|---|---|---|
| Patient satisfaction rate | NA | 86% | 89% |
| Number of patients | 12,100 | 13,717 | 15,962 |
Table 4: Patient satisfaction rate and number of patients in the hospital (2010-2012).
Concerning the patient satisfaction rate, it is compared between 2011 and 2012, since in 2010 the rate was not available. It increased by 3% from 86% in 2011 to 89% in 2012.
| 2010 | 2011 | 2012 | |
|---|---|---|---|
| Number of patients refugees | 0 | 0 | 76 |
| Percentage of refugees | 0% | 0% | 3.40% |
Table 5: Rate of patients refugees from 2010 to 2012 in the hospital.
The hospital received 76 patient refugees in 2012, representing 3.4% of the new admitted patients in the hospital during this year.
Conclusion
According to SEAM and the interviews analysis method, the diagnostic step highlights a negative impact of accreditation on staff. The main dysfunctions during this preparation period before accreditation were related to working conditions and work organization. Employees worked under pressure in a stressful atmosphere, in order to comply with all the standards of the Lebanese accreditation. The workload and required tasks of preparations from employees induced fatigue and exhaustion, the priority of work was for accreditation. During interviews, healthcare professionals from different departments emphasized on the weight of paper work during preparations for the process. In addition, the demand of meetings and trainings increased during this phase, leading to overtime and overconsumption.
On the other hand, this period presented a positive influence due to staff dedication, cooperation and collaboration between them, between managers and staff and between managers. Preparing for accreditation engendered motivation for healthcare providers to improve their skills and knowledge through trainings and upgrades.
Largely speaking, according to the interviews with staff from all levels at the hospital, the impact of accreditation on staff was mostly negative even though it has advantages for healthcare professionals.
Furthermore, the process of accreditation, was quietly standardized, and had a positive influence on the performance and operations in the hospital. The documentation system, policies, and procedures enhanced the regulations and organization of the hospital. The preparations for accreditation that included upgrades and renovations presented a considerable financial burden of $5,532,742.18 for the rural, 220 beds hospital. These costs involved the infrastructure maintenance, new equipment, available property upgrade, recruitment of new staff, training of current staff, salary adjustment, administrative services, dietary services, staff benefits, housekeeping services, laundry services and consultant costs during the period of preparations 2010-2011.
The quality of care was automatically affected progressively, leading to an increasing rate of patient satisfaction. From 2011 to 2012, the patient satisfaction rate in this study increased from 86% to 89% (3%), which confirms a positive impact of accreditation on value of care and patient safety. It reveals a general assessment about the structure, process and outcome of care. Their satisfaction induces their return to the same healthcare institution when needed, in addition to the recommendations for friends and relatives, leading to patient retention and loyalty. Patient satisfaction represents an important consideration in a healthcare competitive market. Additionally, the increased number of patients confirms further the positive impact of accreditation on quality of care.
In terms of profitability, the financial indicators used in this study showed a positive impact of accreditation on hospital’s revenue. After accreditation, the return on investment increased by 2.5%. This showed efficiency in the investment of accreditation in spite of high costs of accreditation. The expenditures are beneficial on the long run and not particularly for accreditation, but for the hospital’s improvement: the lifetime of upgraded/new equipment and infrastructure, knowledge, and skills enhancement of staff, and services renovations.
The contribution margin per hour increased after accreditation, which presented a positive impact of accreditation on profitability and productivity.
Despite the negative impact of accreditation on staff, the productivity rate increased by 3.67$: it reveals that even with unfavorable working conditions made up of stress and exhaustion, the healthcare professionals managed to increase productivity.
In this case study, the Lebanese accreditation in 2011 shows an indirect positive impact on hospital profitability despite of the significant financial burden of preparations. The standardized process of accreditation affects effectively the quality of care and healthcare performance, leading to patient satisfaction and an increase in number of patients, generating higher revenue for the organization. Therefore, according to SEAM diagnostic process, it presents practically a negative impact on staff due to distressing working conditions loaded with stress and overwork, physical and moral tiredness.
The limitations of this study are the following:
- Confidentiality of the financial data that restricted the financial indicators of the study.
- The difficulty of access to sufficient data in order to calculate hidden costs and add them to visible costs.
- The study was restrained to one hospital.
- Due to the fact that interviews were done 7 years after accreditation (2011-2018), the perception of staff may be distorted and their views on accreditation would be less accurate.
References
-
Saleh SS, Sleiman JB, Dagher D, Sbeit H, Natafgi N (2013) Accreditation of hospitals in Lebanon: is it a worthy investment?. International Journal for Quality in Health Care 25(3): 284-290.
-
Oliveira J, Gabriel C, Fertonani H, Matsuda L (2017) Management changes resulting from hospital accreditation. Revista Latino-Americana de Enfermagem.
-
Grepperud S (2014) Is the hospital decision to seek accreditation an effective one?. The International Journal of Health Planning and Management 30(1).
-
Melo S (2016) The impact of accreditation on healthcare quality improvement: a qualitative case study. Journal of Health Organization and Management 30(8): 1242-1258.
-
Jovanovie B (2005) Hospital accreditation as method for assessing quality in healthcare. Arch Oncol 13(3-4): 156-157.
-
JCI (2017) Benefits of Joint Commission Accreditation.
-
World Health Organization (2010) Country Cooperation Strategy for WHO and Lebanon 2010– 2015.
-
Conbere J, Heorhiadi A (2011) Socio-Economic Approach to Management: A Successful Systemic Approach to Organizational Change. OD Practitioner 43(1).
-
Tabchoury P (2016) Applying Socio‐Economic Approach to Management in Lebanon: Challenges, Design, and Results. In: Conbere J, Savall H, Heorhiadi A, et al. (Eds.), Decoding the socio- economic approach to management. Charlotte, NC: Information Age Publishing, Inc.
-
Pink GH, Holmes GM, Dalpe C, Strunk LA, Mcgee P, et al. (2006) Financial Indicators for Critical Access Hospitals. The Journal of Rural Health 22(3): 229- 236.
-
Ford RC, Bach SA, Fottler MD (1997) Methods of Measuring Patient Satisfaction in Health Care Organizations. Health Care Management Review 22(2): 74-89.
-
Haj-Ali W, Karroum LB, Natafgi N, Kassak K (2014) Exploring the relationship between accreditation and patient satisfaction the case of selected Lebanese hospitals. International Journal of Health Policy and Management 3(6): 341-346.
-
Astuti HJ, Nagase K (2014) Patient loyalty to health care organizations: Strengthening and weakening (satisfaction and provider switching). Journal of Medical Marketing: Device, Diagnostic and Pharmaceutical Marketing 14(4): 191-200.
-
Arab M, Ghazi Tabatabaei SM, Rashidian A, Rahimi Forushani A, Zarei E (2012) The effect of service quality on patient loyalty: a study of private hospitals in Tehran, Iran. Iranian J Publ Health 41(9): 71-77.
-
Ministry of Public Heath & High Authority of Health (2008) The national accreditation procedure of healthcare organizations in Lebanon as of 1st January 2009.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda