Risks Affecting Quality in the New Clinic San Sebastian Girardot, Colombia
Introduction: In Colombia, as in the rest of the world, the aim is to articulate the entire health system in order to verify quality, and it is important to implement mechanisms and tools that constantly evaluate the quality offered by each of the actors. Objective: Determine the existing risks that affect the quality of hospital and emergency services in the new clinic San Sebastián Girardot, Colombia, based on current regulations in the sector, to obtain the organization’s accreditation. Methodology: A descriptive observational quantitative investigation was carried out, on primary sources, internal and external clients of Nueva ClÃnica San Sebastián, with secondary sources, the institution’s quality files, for the identification of risks. Was used to collect the information The SERVQUAL MODEL, Parasunaman model. To obtain the Service Quality Index, the model presents five dimensions also known as quality dimensioning indicators. Ethical aspects: According to the Declaration of Helsinki, 1975, Resolution 8430 of 1993 del and resolution 0413 of 2018, it is a research without risk, institutional consent was obtained. Results: The univariate analysis showed 62.3% for the expectations of the client and their perception in relation to the services provided, with great satisfaction and moderate satisfaction of 57%. With external clients, it was found that users have moderate satisfaction in all dimensions, the dimension of sensitivity or response capacity has a higher degree of satisfaction in users, in relation to meeting their expectations, with 85%, followed by the security dimension with 58%, and empathy with 57%. Conclusion: Research indicates that both internal and external clients report less than 50% satisfaction and in some cases they are totally dissatisfied, which constitutes a risk for the institution.
Introduction
Health care quality must be framed in the development of actions aimed at achieving a better quality of life for the population, this is achieved by placing a priority, in the center of the process to the human being, offering care that foster the balance their health, within a framework of the humanization of care services and its quality, which is oriented, based and characterized by strategic, missionary and institutional support processes, which allow the care provided to be of excellent quality [1, 2].
The Health System worldwide is based on four premises that lead it to get with the principles of safe and humanized care, Equity, Effectiveness, Efficacy, and Efficiency, which must be related to each other, not implying It fails in the processes that lead to NO quality of services, to the dissatisfaction of users, in which not only are patients considered, but all actors in care (internal and external clients) are included and intervened. Linked to these principles is the access to care, which is one of the main concerns of health policies, which in turn is a poorly defined concept, which is confused with terms such as accessibility, availability, or search attention [3, 4].
Two types of related trends are observed with access to care health services, those authors who define access as the fit between the characteristics of services and population and the ones who equating it with the use of services. Within this approach, one of the most widely used theoretical proposals is the one developed by Aday and Andersen, which distinguishes between realized access - effective use of services-and potential-factors that predispose and enable the use of services. The principles of the security system are the fundamental basis for excellent-quality health care that allows safe care and satisfaction for users [5]. The strategies for their evaluation have been based on two models, that of user satisfaction to starting from the concept of quality proposed by Donabedian, and the model of discrepancy or lack of confirmation proposed by Parasuraman [6, 7, 8].
It is important to review the context of quality in health services in Colombia, where according to the regulations it is intended to articulate the entire health system to guarantee quality in all its aspects, being important to implement mechanisms and tools that allow to constantly evaluating qualitatively and quantitatively the quality offered by each one of the actors [9]. The complexity of the network that represents the Colombian health system and the provision of the service itself means that there are two fundamental factors for each of the entities involved, efficiency and equity, which must be complementary for the proper functioning of the Health system to achieve efficiency in service provision [10].
Health institutions in Colombia are obliged to provide health care taking into account the individual as a whole, not atomizing it as care is currently carried out, where patients attending a hospital center are being affected by not reestablishing in the shortest possible time, the balance in their health and where all the actors of the system (owners, partners, internal and external clients), are also affected by the increase in costs by not providing comprehensive and quality services [11].
The Colombian health system has particular characteristics that make quality accreditation an almost mandatory strategy for the good performance of each of the organizations. Due to the demands and compliance with quality standards for the adequate provision of the service, the General System of Social Security in Health (SGSSS) is created, designed to correct deficiencies in the provision of health services, which constitutes an important factor for the identification of the risks that affect the provision of quality services and that in the future may affect the achievement of accreditation standards in a health institution [12].
For purposes of evaluating and improving the Quality of Health Care, the SOGCS must meet the following characteristics, accessibility, as the possibility for the user to use health services that guarantee the General System to the Social Security Health, possibility for the user to obtain the services he requires, without delays that put his life or health at risk. This characteristic is related to the organization of the supply of services about the demand, and to the level of institutional coordination to manage access to services, Security, set of structural elements, processes, instruments, and methodologies, based on evidence scientifically proven and approved, which aim to minimize the risk of suffering an adverse event in the health care process or mitigating its consequences, Continuity, such as the degree to which users receive the required interventions, through a logical and rational sequence of activities, based on scientific knowledge [13, 14].
For the evaluation of the care system in organizations, it is also important to identify other attributes under which quality levels in health services, efficiency, effectiveness, flexibility, participation, credibility, and trust can be evaluated, and the scientific-technical quality of the institution. Riley and Cols, consider that accreditation is one of the most important initiatives aimed at improving the quality of health services that are currently offered, point out that it has been the product of several years of collaboration and research, and maintain that accreditation it is a set of standards that allow the adequate provision of health services following the guidelines for quality, promotion, and prevention [14].
In turn, Toro and Cols argue that the search for new quality management systems in companies in the health sector is oriented towards the design of new indicators and indexes for the control and monitoring of all processes, as this guarantees in some way obtaining quality certifications and differentiation competitive with other organizations, so that results in conditions for the survival of the organization over time. Hence the importance of determining the costs of non-quality in the provision of services and optimizing the existing processes to improve the quality of health care [15].
Referencing the importance of risk management in the health sector can mention two types of risks, the existential and administrative, the first directly affect the patient during care, now known as adverse events and may reach affect people’s lives, leading the patient to suffer complications and lead them even to death, hence the importance of providing excellent quality services that lead the institution to be recognized nationally, which stands out from the other existing health institutions in the city, to consolidate it as a safe health institution, with the minimum risks in its healthcare processes, with a suitable healthcare staff that provides comprehensive patient care [16, 17, 18, 19, 20, 21].
Administrative risks affect the quality of caretaking legal implications with users, administrative with the EPS or with employers and financial by the impact-oriented in the billing process, the establishment of accounts and payment of care provided to users by the EPS, which are represented in the glosses, returns and non-payments of services, financially impacting the institution. These risks, whether healthcare or administrative in health care, are very important due to the social implications they have; it is people’s lives that are affected by different events or positive or negative risks in health care [22].
Managing risk in the new CLÍNICA SAN SEBASTIÁN- NCSS is performed in isolation and empirical in some care processes and administrative, without a systematic analysis to full integration of risk management across the organization. The research aims, determining the risks that affect the quality of hospital services and emergency in NCSS Girardot, based on the current regulations in the sector to obtain accreditation of the organization.
Materials and Methods
A descriptive observational quantitative investigation was carried out on primary sources, internal and external clients of Nueva Clínica San Sebastián, with secondary sources, the institution’s quality files, to identify the risks.
The SERVQUAL MODEL was used to collect information Parasunaman model. This is a method of evaluating the key factors to measure the quality of the services provided, is based on the classic client evaluation model, which considers that every client who acquires a service has expectations of it, the perception can change the result of many factors or dimensions. The difference between these two moments is known as the Customer Satisfaction Index and is the indicator obtained from the adequate treatment of the information that is achieved by applying this tool. This model has validity greater than 83, according to Combrach’s Alpha [23].
Customers’ expectations are guided by their needs, possible experiences of own or other past, which in one way or another limit the perception of the service. With the application of this model is sought to obtain a rating of the quality of service, Quality Index Service (ISC), determine what customers want, evaluate what they find taking care, their degree of dissatisfaction and finally allows ordering quality defects and risking determination, for prioritizing the implementation of improvement plans.
To obtain the Service Quality Index, the model presents five dimensions also known as quality dimensioning indicators, among which are:
Tangible Elements
Evaluate the appearance of facilities, equipment, and communication materials with which the organization has.
Reliability
Determines the ability to have the organization at the time of providing the promised service “as promised”, with zero errors. Evaluates the efficiency in the use of time and materials, the effectiveness with which the client obtains the service and the effectiveness with which the client obtains the service through a correct process that meets the expectations for which it was designed, its non-compliance generates an increase in costs for the organization.
Response capacity or response speed
Takes into account the desire to meet customer needs in a timely and efficient manner.
Security or warranty
Refers to the knowledge of the service provided, courtesy of employees, and their ability to convey confidence to the customer.
Empatia
It is individualized customer service; it is the connection between employee - user, essential to understanding the needs of another.
The Service Quality Index is equal to Perception - Expectation This ICS is obtained from the application of the Likert scale from 1 to 4, which when subtracting 3 general situations are observed: Positive quality index = PE = 4-2 = 2 Satisfied customer. You have perceived better service than you expected. Above zero on the scale Neutral quality index = PE = 3-3 = 0 The client feels good with the service, he gets what he expected. Zero position on the scale. Negative quality index = PE = 2-4 = -2 Dissatisfied customer, perceives something lower than expected. Negative position on the scale [2.3].
The study population was made up of 750 internal clients and 6,750 external clients, assistants to the emergency, and Hospitalization services of the San Sebastián clinic. The sample consisted of 440 external clients and 289 internal clients, through proportional sampling in the StalCal program, from the free software Epi-info 7.2. The questions were adapted for each of the two categories of clients and a pilot test was carried out to ensure understanding and clarity of each question. For the selection of the analysis units, a list of both populations was obtained, supplied by the institution and random numbers were assigned, the individuals were extracted one by one, until completing the sample. In a personal way, one of the researchers applied the instrument to the total of both samples.
Ethical aspects
According to the ethical standards according to the Declaration of Helsinki and subsequent revisions and Resolution 8430 of 1993 of the Ministry of Health of Colombia, and resolution 0413 of 2018 of the Ministry of Science and Technology of Colombia, it is research without risk, institutional consent was obtained from the legal representative of the institution and informed consent was applied to each analysis unit, the right to privacy was protected, sensitive data was not recruited from the analysis units.
Results
The univariate analysis allowed obtaining these data, according to the customer’s expectations and their perception about the services provided, 62.3% were found with great satisfaction and a moderate satisfaction of 57%. With external clients it was found that users have moderate satisfaction in all dimensions, the dimension of sensitivity or responsiveness, has a higher degree of satisfaction in users, concerning meeting their expectations, with 85%, followed by the security dimension with 58%, and empathy with 57%. The internal clients, Figure 1, have a moderate satisfaction in all dimensions except the tangible elements achieving great satisfaction with 43%, the dimension of sensitivity or responsiveness is having greater user satisfaction, with the fulfillment of their expectations with 100%, followed by the dimension of empathy with 63%, and security with 56%.
It was found that for both groups the expectations of care are affected by the sensitivity or response capacity dimension, which represents the highest percentage of dissatisfaction with 7% for the external client and 4% for the internal client. For the two groups expectations of care are affected by the dimension of sensitivity or responsiveness, which represents the highest percentage for little satisfaction with 15% for domestic customers and 14% for the external customer. The expectations as of care are affected by the dimension of sensitivity and responsiveness that represents the highest percentage for the median satisfaction with 51% for external customers and 40% for the domestic customer, followed by the security dimension with 35% for the external client and 22% for the internal client, with a close relationship with the empathy dimension with 35% for the external client and 25% for the internal client (Figure 1).
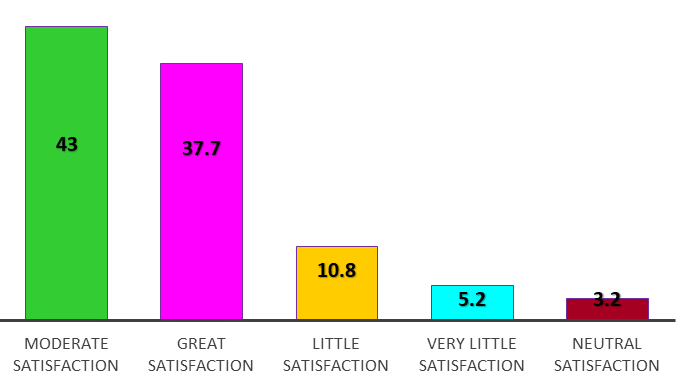
Figure 1: General satisfaction of users who attend the New Clinic San Sebastián, Girardot, Colombia In the dimension of tangible elements, the appearance of the facilities, equipment, and communication materials found in the Nueva Cínica San Sebastián de Girardot available for the attention of users were evaluated. It was found that 50 of 100 respondents have great satisfaction with the technology, resources, and communication methods of the institution, followed by a moderate satisfaction given by 40 every 100 respondents. When comparing internal and external customer satisfaction about the dimension of tangible elements, it was found that 60 out of 100 internal users have great satisfaction regarding the dimension, compared to 50 out of 100 External customer users, followed by moderate satisfaction found in 40 out of 100 external and internal customers.
The reliability dimension evaluates the efficiency in the use of time and materials, the efficiency with which the client obtains the service and the effectiveness in obtaining the service through a correct process that meets the expectations for which it was designed, according to the User response found that 40 out of 100 customers consider that the ability of the organization to provide the promised service, with zero errors, is good. According to the comparison of internal and external customer satisfaction concerning this dimension, it was found that 40 out of 100 internal and external users have moderate satisfaction, followed by great satisfaction in
40 out of 100 internal clients and 30 of each 100 external clients.
The sensitivity or responsiveness dimension takes into account the desire to meet customer needs in a timely and efficient manner. According to what is expressed in responses 40 out of 100 users, they have a good perception of attention, related to the opportunity. In both groups of clients, internal and external, it was found that 40 of every 100 have a moderate satisfaction on the dimension, compared to 30 of every 100 users of internal and external clients with great satisfaction.
The security or guarantee dimension refers to the knowledge of the service provided, the courtesy of the employees, and their ability to transmit confidence to the client. According to this definition, it was found that half of the users, (internal and external customers), consider that the attention provided by the employees was good. It was found that 50 out of every 100 external and internal users have a moderate satisfaction on the dimension, compared to 30 out of every 100 users of internal and external customers with great satisfaction.
The empathy dimension has as reference the individualized attention to the client, the connection between employee-user, fundamental communication to understand the needs of the other. According to what has been revealed by users, 40 out of 100 consider that internal customer empathy vs. External client is good.
According to the axes of accreditation, patient’s security is understood as a set of structural elements, processes, tools, and methodologies that seek to minimize the risk of an adverse event in the process of health care, according to the study conducted with internal and external New Clinic San Sebastián customers, we found that relative to this axis the 50% of internal users and 40% of the external users have a moderate satisfaction, followed by 40% of internal users and 30% of external users, who have great satisfaction. The axis of accreditation, humanization, refers to the existence of policies and programs aimed at the humanization of care, which they consider the dignity of the human being. As a result of the study, it was found that 40 out of 100 internal and external customers perceive moderate satisfaction, followed by 30 out of 100 external and internal users who perceive great satisfaction.
When analyzing the axis of technology management accreditation which is related to technology planning through a rational process of acquisition and use that benefits users and institutions, it was found that half of the internal and external users presented a great satisfaction, followed by 40% of external and internal users who presented moderate satisfaction. For health accreditation, the focus and risk management is of utmost importance, which is carried out through the provision of accessible and equitable health services, taking into account the balance between benefits, risks, and costs derived from the care of users, the study found that 50 out of 100 internal and external customers have medium satisfaction, followed by 30 out of 100, who have great satisfaction.
According to what was investigated, the work showed that 50% of internal clients and 40% external clients consider they have moderate satisfaction with the care of medical personnel and 30% have great satisfaction. According to the investigation the daring work than 50% of internal customers and 40% external customers considered to have moderate satisfaction with the care of nurses and 30% of internal and external customers have great satisfaction. According to the investigation work fearlessness than 50% of internal customers and 40% external customers considered to have moderate satisfaction with care of the administrative staff and 30% internal and external customers they have great satisfaction. The work showed that 50% of internal clients and 40% of external clients consider that they have great satisfaction with the administration of the clinic and 40 of each 100 internal and external clients have moderate satisfaction. The dissatisfaction percentage is less than 1, for these four components.
It was found that 46% show moderate satisfaction concerning the organization’s interest in solving users’ health problems, represented by half of the internal clients and 41% of external clients, 37%, had great satisfaction with 43% of internal clients and 31% of external clients, and 14%, have little satisfaction. According to comments or suggestions given by the users the facility must: “Better to provide better service, very few flaws in general care and service is good, I’ve felt satisfied sense with service, attention has been excellent, very good”.
Half of the users of the research population would recommend the institution to other users for their great satisfaction with the service received, while 40 of 100 users would for its moderate satisfaction, while 6% think or what would do for the little or very little satisfaction that they presented when receiving the services of the clinic.
When performing the bivariate analysis of the most relevant data, the p values, less than 0.05 obtained when crossing the variables and dimensions (Table 1), indicate that there is a probable statistical relationship between the dimensions of response capacity, elements tangible, empathy, reliability, and security, with the dissatisfaction of the internal client, as well as the external one and also with the low satisfaction of the internal client, for the external client, as well as for moderate satisfaction and great satisfaction, no possible relationship was found.
| Dimension | External customer dissatisfaction | Internal customer dissatisfaction | External customer satisfaction | Internal customer satisfaction |
|---|---|---|---|---|
| Answer’s capacity | 0.0168 | 0.0305 | 0.0627 | 0.0664 |
| Tangible elements | 0.0044 | 0.0054 | 0.0548 | 0.0216 |
| Empathy | 0.0074 | 0.0242 | 0.055 | 0.0487 |
| Reliability | 0.0096 | 0.0433 | 0.0984 | 0.04 |
| Security | 0.0066 | 0.0112 | 0.0438 | 0.496 |
Table 1: Cross between the perception of internal and external clients by dimensions of satisfaction, according to the value of p
When crossing the perception of internal and external clients, to assess their degree of satisfaction, according to the axes of accreditation (Table 2), a possible relationship was found between the risk approach, technology management, humanization patient care and safety, with the dissatisfaction of internal and external clients. No possible relationship was found with the other degrees of satisfaction.
| Axes of Accreditation | External customer dissatisfaction | Internal customer dissatisfaction |
|---|---|---|
| Risk approach | 0.015 | 0.026 |
| Technology management | 0.009 | 0.008 |
| Humanization of care | 0.039 | 0.052 |
| Patient safety | 0.016 | 0.046 |
Table 2: Perception crossing of internal and external clients by axes of accreditation, according to the value of p.
Faced with the intersection of perception of services and the degree of satisfaction of internal and external clients (Table 3), a possible relationship was found between the administration services of the clinic, administrative personnel, nursing personnel, medical personnel, and the dissatisfaction of both clients, internal and external. In the other degrees of satisfaction, no p-value was found, suggesting a possible association.
| Perception of services | External customer dissatisfaction | Internal customer dissatisfaction |
|---|---|---|
| Clinic administration | 0.009 | 0.033 |
| Administrative staff | 0.02 | 0.045 |
| Nursing staff | 0.024 | 0.0 45 |
| Medical staff | 0.023 | 0.034 |
Table 3: Crossing the perception of internal and external customers for services, according to the value of p.
Discussion of Results
When conducting the literature review, the researchers found no written reports from similar investigations, which made it difficult to contrast the results to strengthen the discussion. The work made it possible to determine the feeling of the users regarding the conditions of care in the institution, which facilitates the implementation of an improvement plan to intervene in each of the points by which internal and external clients feel unsatisfied.
The quality assessment has become an area of knowledge, supported by methods and techniques of the social sciences, with two aspects: an assessment from the perspective of professionals and users, being the first initially most used. Evaluation from the perspective of users has become relevant since health sector reforms. The strategies for their evaluation have been based on two models: that of user satisfaction based on the concept of quality proposed by Donabedian, and from the discrepancy or confirmation model proposed by Parasuraman.
Quality in health is a concept proposed by Donabedian, who established the definition around three important axes [4]: the structure, the process, and the result taking into account the variables that intervene in the provision of health services, whose model defined it “Quality of care is one that is expected to provide the user with the maximum and most complete well-being after assessing the balance of gains and losses that can accompany the process of all its parts” and describes satisfaction as a concept It groups three dimensions that are likely to generate satisfaction: the first is the technical component that is the application of science and technology in the management of a person’s problem so that it yields the maximum benefit without increasing its risks, it is also known as scientific-technical quality.
The second dimension is the interpersonal component and is a defined environment or like the relationship between people should follow the norms and values that govern the interaction of individuals in general. The third dimension is the Comfort Component given by all those elements of the user’s environment that provide more comfortable care. Each component intervenes generating actions, both for health personnel and the user in a service relationship. In this way, the interpersonal relationship and the characteristics of the place in which health service is provided must reflect respect, allow privacy and comfort, which decisively influences the acceptability, nature, and success of care and the benefits of the same, managing to find a balance between technical care and humane treatment 814.
The Parasuraman model is based on the idea that the client perceives the quality of service as the difference between what he expects from it and what he receives. This difference between the design and the provision of the service that is offered is due to communication problems between the client and the service provider and also due to the lack of harmony within the organization. Following this evaluation of the service, the risk is determined, which includes three elements: the event whose occurrence is to be modified, the multiple causal factors associated with the occurrence of the event, and the effects generated when the event occurs. In turn, causal factors can be grouped into factors external to people (dangers or threats) and internal factors to them (vulnerability or susceptibility). If the causal factors are modified, before the event occurs, the occurrence of the event is modified, whereas once the event has occurred, it is only possible to modify its effects [22].
According to the above Management, Risk has gained strength in all hospital institutions, in this case, it has been taken as the base model explaining Multi causality or model Swiss cheese, in this model has big importance the patient’ safety and the prevention of adverse events, contributing to the analysis of the failures that occur in the care system and their impact on patient safety. Its operation is based on identifying and putting into operation barriers or obstacles that serve the system so that patients are not harmed- adverse events-when at any time and for some reason these barriers or obstacles fail, patient safety is affected [24].
Health organizations are an example where risk management is imminent since they enable and provide citizens with medical and public health services in accordance with the degree of social, economic, and scientific development of the country. The term risk in the healthcare field immediately refers to a danger to the patient in the form of an unexpected and, almost always, unfavorable result. Consequently, for the management of health risk, a methodology is proposed that allows the mitigation of these events, in high-level health entities, centralized in Colombia, due to the lack of an Integral System that guarantees the correct actions for the risk management. The risk management methodology is introduced, in the context of public health system reforms, the safety of patients and professionals to reduce viable costs [25].
When reviewing the various works carried out on quality in health services in Colombia and worldwide, there are few documents at the national level on what has been done to identify and determine the importance of quality in health services Health Worldwide, there are works in Latin American countries such as Cuba, Mexico, Chile, Argentina, Brazil, United States and in European countries such as Spain, all of them have investigated the impact that quality has had in the provision of health services and many of them, it has been concluded that one of the most important benchmarks for evaluating the quality of health services is customer satisfaction [6, 11].
María E. Delgado Gallego, María L. Vázquez Navarrete, and Lygia de Moraes Vanderlei carried out a study comparing the health models between Colombia and Brazil due to the great similarities that exist in the two systems, one of their conclusions was, “Humanization attendance is significant for all actors interviewed. For users it is a dynamic dimension that is related to others: with the technical level of care (a good physical or clinical examination), with organizational accessibility (more time per patient) and with accurate, detailed, and understandable information in a cordial framework” [5].
In order to improve the quality in the provision of health services in the aspects of accessibility, opportunity, security, relevance, and continuity, Decree 2309 of October 15, 2002 was published. The Single Accreditation System is a component of the Quality Guarantee System, which is made available to health service providers, EPS, ARS, and prepaid medicine companies who voluntarily want to demonstrate compliance with high levels of quality, that is, above the minimum conditions established by the Unique Enabling System. The Single Accreditation System is oriented, in the management developed by ICONTEC, to establish the degree to which the institutions work, based on the operation of the Health Care Quality Guarantee System. Thus, ensuring superior levels of quality in the provision of its services and its constant improvement [22].
In the case of Colombia, the institutions that have managed to be accredited in the integrated quality systems and that have evolved in the health care of users, allowing them to be awarded by National and International institutions are: The Valle del Lili Foundation, who since 2007 has been accredited by Icontec. In November 2012, the Pablo Tobón Uribe Hospital received accreditation with a degree of excellence, which in 2005 was accredited in health and the scope of the quality management certificate was extended with the NTC ISO 9001 version 2000, to the processes of: Critical care patient care and urgent patient care. In 2006 was again the winner of the Colombian Award for Management Quality (PCCG), organized by the Quality Corporation and the Ministry of Industry and Commerce. In 2008, it applied to the Colombia Health Quality Award, organized by the Hospital Management Center, and is a winner in its gold category. It is re-accredited in health obtaining the highest category Accredited with Excellence [24, 25].
In the case of the present study, there is a great deficiency in the appreciation that the internal and external client has regarding the perception and expectations of the service provided in the New San Sebastián Clinic, where moderate satisfaction was evident in the users, where the internal client has increased dissatisfaction. Therefore, to reach the accreditation process as several institutions in Colombia have been able to do, it is important to give more force to the evaluation of the quality of health services, customer satisfaction, humanization of care, assertive communication, respectful relationships, dignified and equal treatment, and the ability to respond to complaints and claims.
The research achievements allow the implementation of an improvement program that facilitates the necessary changes to point towards accreditation. The greatest difficulty during the process was found in the divergence from the instrument historically used by the institution and adopted by the Ministry of Health [26, 27].
The overall conclusion of the research indicates that both internal and external clients report less than 50% satisfaction and in some cases is dissatisfied, which constitutes a risk for the institution.
Thanks
The researchers thank the clinic administration, patients, and workers for their kind collaboration during the work.
Conflicts of Interest
The authors have no conflict of interest.
References
-
Secanilla Campo E (2016) Percepción de la calidad de atención recibida por futuros padres en una casa de nacimientos. Duazary julio 13(2): 79-86.
-
Penchansky R, Thomas W (1981) The concept of access. Definition and relationship to consumer satisfaction. Med Care 19(2): 127-140.
-
Gold M (1998) Beyond coverage and supply: measuring access to healthcare in today’s market. Health Serv Res 33(3): 625-652.
-
Morelos Gómez J, Herrera TJF, Schmalbach JCV (2013) Application of discriminant analysis to evaluate the impact of accreditation in health in Colombia on profitability indicators. 15(1): 62-71.
-
Andersen RM (1995) Revisiting the behavioral model and access to medical care: does it matter?. J Health Soc Behav 36(1): 1-10.
-
OPS (2010) Metodología De Gestión Productiva De Los Servicios De Salud.
-
Delgado Gallego ME (2010) Quality in health services from the frameworks of meaning of different social actors in Colombia and Brazil. Public health rev 12: 533- 545.
-
Diprete Brown Lori MF (2010) Quality assurance of health care in developing countries. Washington.
-
Córdoba Villalobos J (2012) Comprehensive Health Quality System (SICalidad).
-
World Health Assembly 55th. WHA 55.18 (2002) Quality of care: patient safety.
-
Molina GCF (2011) Institutional management under the pressure of the competitive market in the Colombian health system, 2007-2008. Gale Onefile 24(1).
-
OMS (2017) Health and human rights.
-
Riley WBK (2012) Public Health Department Accreditation Implementation: Transforming Public Health Department Performance. American Journal of Public Health 102(2): 237-242.
-
Herraiz Bermejo L (2011) Quality of perception received by hospitalized patients through sensory therapeutic communication.
-
Salud OP (2019) Quality of Health Services.
-
Américas MD (2007) Agenda de Salud para las Américas 2008–2017.
-
Gómez Rivadeneira A (2014) Marco conceptual y legal sobre la gestión de riesgo en Colombia: Aportes para su implementacion. pp: 4-11.
-
Luengas Amaya SM (2009) Seguridad del paciente: conceptos y análisis de eventos adversos. Obtenido de víasalud número 48.
-
ICONTEC (2019) Accreditation in Health.
-
Martinez FRJ (2001) Health Risk Management Manual.
-
Ana CC, Nelson EM, Juan BM (2015) Vigilancia Tecnológica para la Gestión del Riesgo Tecnológico en el Sector Salud asociado a la norma ISO 31000. Revista Ingeniería Biomédica 9(18): 117-125.
-
ICONTEC (2019) Background in Colombia.
-
Monterrey D (2012) Application of the Servqual instrument and its interpretation.
-
Fundación Valle del Lili (2019) Accreditation in Health with Excellence Valle del Lili Foundation.
-
Uribe HP (2019) Quality management.
-
Centro Médico Imbanaco (2019) Achievements and Awards.
-
Sistema Único de Acreditación en Salud (2019) Unique System of Accreditation in Health.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda