Does Covid 19 Pandemic Challenge Decade of Healthy Ageing??
A pandemic, by definition, represents worldwide, simultaneous epidemics caused by a novel pathogen. The multinational nature of such an event inevitably leads to cross-national comparisons of epidemic growth, impact, and public health response. The intercountry comparisons are vulnerable to attribution of individual-level outcomes to aggregate exposures. Age is one such confounder known to be associated with COVID-19 severity and case fatality. As the countries like Japan, Italy, France, UK, USA have disadvantage of skewed population of elderly, India on the other hand has comparatively younger adults more. On 3 August 2020, the 73rd World Health Assembly endorsed 2020-2030 as ‘The Decade of Healthy Ageing’-a process of developing and maintaining the functional ability that enables wellbeing in older age. The 2020 observance is expected to promote a Global Strategy and Action plan and monitor the progress and challenges in their realization by countries. The SARS COV 2 virus that causes COVID-19 infects people of all ages. However, evidence to date suggests that two groups of people are at a higher risk of getting severe COVID-19 disease. These are older people over 60 years and those with underlying medical conditions. As per UN estimates the current (2019) share of population over the age of 60 in India is 8 % and is projected to increase to nearly 20 percent by 2050. The reported share of Covid 19 cases as of first week August 2020 was 12% and proportion of fatalities was 50% in that age group largest among all age cohorts. Those older than 75 form 2% of India’s population but account for 14% of the total Covid deaths. Covid 19 Pandemic worldwide is prolonging for more than 6 months, second peaks are being witnessed already in some countries and expected in India by December 2020 due winter and stubble burning in North India,. With no definitive treatment protocol, over-stretched health system and uncertainties of vaccine availability to common population. I suspect it will be a big challenge to the objective of Decade (2020-2030) of Health Ageing. This article presents an early overview of the observed and potential impacts of the COVID-19 on the Global Healthy Ageing Decade commitments. I argue that the effects of COVID-19 are determined mainly by anthropogenic factors. Most Public Health Professionals opine that the impact of higher case fatality among senior citizens will continue to have on the quality of the elderly at least for this decade. Most elderly with comorbidities will succumb and those who survive through the pandemic will continue to be healthier and be well equipped to face future pandemics if any. Materials & Methodology: For this paper, the National, Covid-19 cumulative unreleased data of infection, cases, and death by August 2020 from the MOH&FW, GOI has been used. I also accessed print media especially Times of India, Hindustan Times, and Live Mint, all state capital editions. Data of aged population was taken from UN estimation, age composition and Covid 19 data by countries from https://coronavirus.jhu.edu/ and CIA Factbook, 2020 has been used.
Introduction
Aging impacts several components of the immune system including innate and adaptive immunity. Understanding the mechanisms by which aging alters immunity may lead to novel therapies to improve immunity with aging, in particular the ability to clear viral infection. The development of such novel therapies is urgently needed as the number of older people in our society continues to rise, with increasing disease burden from viral infections. It is a known fact that older people are more susceptible to a variety of viral infections, including those that induce respiratory disease, resulting in higher morbidity and mortality than younger people [1].
The immune system is comprised of innate and adaptive arms, and both are involved in control of viral infections. Altered response to any viral infection have important consequences since failure to control this infection can lead to bacterial super-infection and exacerbations of cardiovascular diseases, Renal conditions, Diabetes, Cancers, and even Central Nervous system leading to strokes and sudden blindness. Ageing may impact both the innate and adaptive immune system to impair control of viral infections. Over the years, there has been a greater focus on how aging impacts the adaptive immune system with less known regarding the innate system [1].
Impact of Aging on Adaptive Immunity
Adaptive immunity is important for combating viral infection, in part by generating antigen specific immunity, leading to the development of protective immunologic memory. Aging & adaptive immunity: a) Humoral immunity and aging: Somatic hypermutation (SHM) is a key process for antibody generation and diversity and ageing impacts this process at multiple levels. I) B-cell germinal centres within the spleen and tonsils of aged individual’s exhibit preserved SHM, but in the circulating B-cell pool as well as germinal centres of Peyer’s patches, SHM decreases with age. ii) E47 is a transcription factor encoded by E2A that regulates many B cell functions. iii) The activation-induced cytidine deaminase (AID) induces class switch recombination (CSR) and Ig somatic hypermutation. Expression of E47 and AID Thus, aging impairs antibody generation by B cells at several levels to reduce humoral immunity. Both the number and proportion of peripheral B-cells decrease with age. This is likely a consequence of decreased total number of IgM memory B cells. Overall, aging impacts the B-cell pool with memory B-cells exhibiting reduced numbers while naïve B-cell pool size remains preserved. All these components of humoral immunity are affected by aging as B cells isolated from peripheral blood of older human subjects have decreased. Bacterial super-infection is a complicating factor, which worsens morbidity and mortality after respiratory viral infections, including influenza and Covid 19. On a functional level, aging impairs the ability to generate protective antibodies in response to both vaccination and infections [1].
b) Aging and T-cell function: Antigen-specific B cells require interactions with CD4+ T cells for subsequent expansion and differentiation and generation of T-cell dependent antibodies. Some studies have shown that aged CD4+ T cells have a reduced ability to form functional immunological synapses upon stimulation with peptide pulsed antigen presenting cells (APC) than young T cells, leading to defective T-cell receptor activation and poorer IL-2 production with ageing. Experimental studies suggest that this restricted repertoire may impair control of influenza or herpes simplex viral infection and may be suspected in case of Covid 19 infections.
Aging and Innate Immunity
Plasmacytoid dendritic cells (pDCs) are key cellular responders of viral infection. They are the most potent type I interferon (IFN) producing cells and this action initiates several host responses. This signalling pathway induces the upregulation of several signal adaptors, including IFN regulatory factor (IRF) 3, 5 and 7. There have been several studies that have documented that aging impairs pDCs to produce type I IFNs. Initial scientific work demonstrated that this defect with aging was critical for an impaired ability to clear herpes viruses in aging mice. Other experimental studies have found that aging can impair certain components of TLR responses in macrophages and conventional dendritic cells (DCs), the production of proinflammatory cytokines and upregulation of costimulatory molecules. It is recently found that an imbalanced innate cytokine response induced lethal immune pathology during viral infection using experimental models of herpes viral infection, including HSV and CMV. If such work is translated to humans, it will suggest that specific anti-inflammatory therapies may be beneficial in older people infected with influenza viral infections and Covid 19 [1].
The virus that causes COVID-19 infects people of all ages. However, evidence to date suggests that three groups of people are at a higher risk of getting severe COVID-19 disease. These are i) older people over 60 years old ii) those with underlying medical conditions (such as cardiovascular disease, diabetes, chronic respiratory disease, and cancer). The risk of severe disease gradually increases with age starting from around 40 years [2] and iii) Overweight and Obesity. The latest advisory from CDC Atlanta based on 2 studies in USA found that overweight patients were 40% more likely to die than healthy-weight patients, while obese patients were at 30% greater risk, compared with the healthy-weight patients [2].
There is a mix up in most of the Covid 19 worldwide data. The infection rates based on Rapid Antigen and RT-PCR tests, the symptomatic cases with different severity confirmed by RT PCR test, attack rates based on test positivity, case fatality rates among those hospitalized and post-mortally tested positive deaths. Biggest confusion is use of infection rates and case rates even though a large proportion of infections are asymptomatic, and worst is in association of deaths with comorbidity.
Globally Covid 19 mortality is to a large extent determined by access to and quality of health care. For seasonal influenza, mortality is usually well below 0.1% and for Covid it is around 1-2%. Over 95% of these deaths occurred in those older than 60 years. More than 50% of all fatalities involved people aged 80 years or older. Reports show that 8 out of 10 deaths are occurring in individuals with at least one comorbidity, those with cardiovascular disease, hypertension, and diabetes, but also with a range of other chronic underlying conditions [3].
Mortality for COVID-19 appears higher than for influenza, especially seasonal influenza. While the true mortality of COVID-19 will take some time to fully understand, the data we have so far indicate that the crude mortality ratio (CMR) or case fatality rates is between 1.5-4.5 %, globally with the exception of Mexico (10.4). The infection mortality rate (the number of reported deaths divided by the number of infections) will be lower (Figures 1-5).
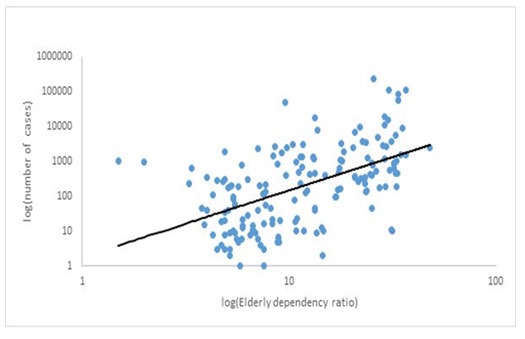
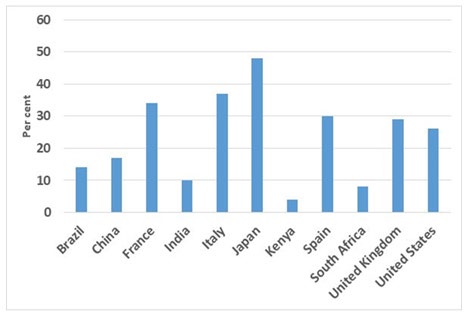
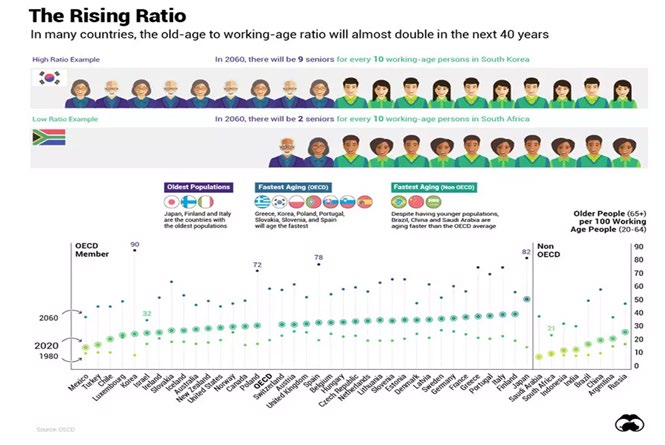
The novel Covid-19 is affecting the advanced countries disproportionately more than developing countries. Covid-19 casualty is higher in countries where there is a large ageing and overweight or Obese population. Looking at particularly the elderly dependency ratio which is the ratio of elderly population (ages 65+) per 100 people of working age (ages 15-64). source of the data for 2020 came from the CIA (Central Intelligence Agency) World Factbook--). Japan has the highest dependency ratio at 48%, Followed by Italy (36.6%), Spain (30.4%), France (33.7%), the UK (29.3%), and the US (25.6%). The developing world with higher fertility rates and lower life expectancy than developed countries have a lower elderly dependency ratio for example in India it is 8% [2]. What Does DATA Show The number of new cases per week has remained stable at 2 million for the past three weeks with the cumulative total of about 37 million cases in 235 countries. Over 1 million deaths have now been reported globally, of which the majority were reported in the Region of the Americas (55%), followed by Europe (23%). In the past week, the regions of the Americas, South-East Asia, and Europe account for 91% of new cases. India, the United States of America, Brazil, Argentina, and France reported 60% of new global cases week ended on 10th October 2020.
The relative risk of dying from COVID-19 is higher for men than for women in almost all age groups in all countries. The overall relative risk ranged from 1.1 to 1.9. The novel Covid-19 is affecting the advanced countries in the Western Hemisphere disproportionately more than developing countries. In most countries, sex differences increased until ages 60–69 years, but decreased thereafter with the smallest sex difference at ages 80+. [4]. When researchers associated the incidence of Covid-19 and fatality rates across the globe with the elderly dependency ratio, which is a reasonable proxy for the age composition of the population they found that the correlation coefficients1 which were 0.53 and 0.44
respectively, both significant at the 1% level as seen in the figures 2 & 3.
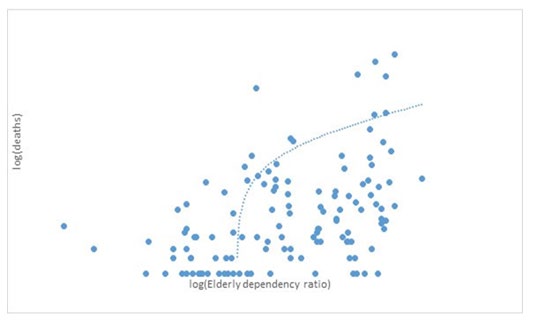
Covid-19 casualty is higher in those countries where we already have an ageing population, with older people requiring hospitalisation and subsequently die from infection. These correlations are strikingly different as the age profile of Covid-19 mortality is quite opposite to that of the Spanish flu (1918) pandemic where young working age adults were mostly the victims [1]. The recent advisory from CDC Atlanta based on two studies one in the UK and another in Brooklyn, US. The Brooklyn study, which observed over 500 patients hospitalised, found that overweight patients were 40% more likely to die than healthy-weight patients, while obese patients were at 30% greater risk, compared with the healthy-weight patients. The British study examined lifestyle risk factors among 760 had Covid-19 patients and found overweight people were roughly 30% more likely to be hospitalised upon infection.
Indian Data
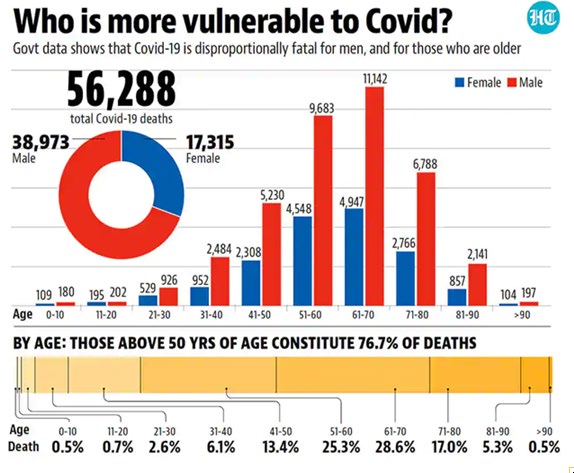
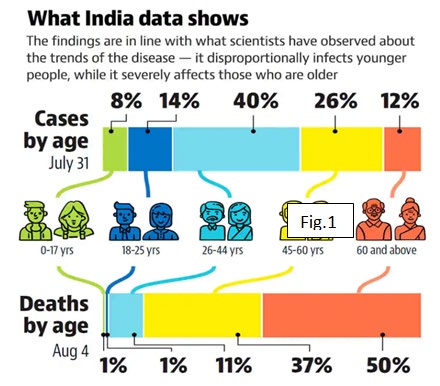
The unreleased case data from the Union ministry of health and family welfare, accessed by HT, shows that more than half (54%) of the people infected in India are between the ages of 18 and 44, while half (50%) the people who succumbed to the disease are above 60 years of age. Most deaths-50%-are in the age group of 60 years and above, followed by 37% deaths among people between 45 years and 60 years in age. About 11% of people who succumbed to the disease were between 26 and 44 years of age and 1% each belonged to the 18-25 years and below 17 years cohorts. The latest mortality data also shows 68% of the Covid-19 deaths in the country are among men and 32% are of women (Figures 1-7).
More than half the 56,292 Covid-19 deaths across states by August 22 were in the 50 -70 age group, with Covid-19 deaths being the highest in the 61-70-year age group among both genders. Twice as many men have died of the Covid-19 as women in India, with men accounting for 69% of all fatalities. By August 22, women accounted for 17,315 and men 38,973 of the total Covid-19 toll of 56,292. There were 301 Covid-19 deaths among people over the age of 90 years, who account for 0.5% of the total deaths. This is much lower than the global average, where people 85 years old and above account for 3.4% deaths [5].
With the results of the second round of Delhi’s SARS-CoV2 sero-prevalence survey released in the first week of October 2020 and other similar surveys in Mumbai and Ahmedabad showed the prevalence of infections was higher among women than among men, however the Pune sero-survey did not find such a gap (Tables 1-5).
| Surveyed City | Date of Survey | Sample Size | Sero-prevalence % among women | Sero-prevalence % among women | |
|---|---|---|---|---|---|
| DELHI | Aug-20 | 15,000 | 32 | 28 | |
| Mumbai | Jul-20 | 6936 | 43 | 38 | |
| Pune | July/August 20 | 1664 | 50 | 53 | |
| Ahmedabad | June/July 20 | 30054 | 18 | 17 | |
| Bhopal | July/August 20 | 9000 | 34.5 | 39.6 |
Table 1: Four City Sero- surveillance Data in India.
Both Pune and Bhopal surveys indicated a higher prevalence of seroprevalence of 64.5% in users of shared toilets compared to users of independent toilets (45.3%).
| Sex | Share among those | |
|---|---|---|
| Tested | Positive | |
| Female | 33 | 35.5 |
| Male | 67 | 64.5 |
Table 2: Reported cases.
In May, the Indian Council for Medical Research
published its analysis of over one million diagnostic tests for covid-19 conducted between January 22 and April 30. They found that while men made up most positive cases, women were slightly more likely to test positive than they were to be tested.
Reported Cases & Deaths
Based on the cases reported fewer women in the official case counts may be due to because fewer women are being tested, or because fewer women develop serious enough symptoms to warrant testing or hospitalization, the evidence thus far suggests that all three might be true [6].
| Up to 30% | 30----40% | 40-----50% | 50-----60% | 60----70% | ||
|---|---|---|---|---|---|---|
| 0-4 Yrs. | 48.5 | 51.5 | ||||
| 5-19 Yrs. | 39.7 | 60.3 | ||||
| 20-29 Yrs. | 34.9 | 65.1 | ||||
| 30-39 yrs. | 29.6 | 70.4 | ||||
| 40-49 Yrs. | 31.7 | 68.3 | ||||
| 50-59 Yrs. | 33.5 | 66.5 | ||||
| 60-69 Yrs. | 36.7 | 63.3 | ||||
| 70-79 Yrs. | 45.5 | 55.5 | ||||
| 80+ yrs. | 43.4 | 56.6 | ||||
| TOTAL | 34.3 | 65.7 |
Table 3: Covid 19 Cases Recorded Statistics-India.
Similarly, the officially data of deaths indicate that fewer women than men have died of Covid 19 in India and worldwide [6].
| PERU | India | China | Iran | Italy | UK | Spain | USA | South Korea | South Africa | |
|---|---|---|---|---|---|---|---|---|---|---|
| % male deaths | 70.8 | 69 | 63.5 | 59 | 57.6 | 57 | 56.6 | 53.9 | 53.2 | 52.6 |
| % Female Deaths | 29.2 | 31 | 36.5 | 41 | 42.4 | 43 | 43.4 | 46.1 | 46.8 | 47.4 |
Table 4: Proportion of Covid 19 Deaths by top 10 Countries.
| Share of males% | Share of females % | |
|---|---|---|
| 0-4 | 51.5 | 48.5 |
| 5--19 | 60.3 | 39.7 |
| 20-29 | 65.1 | 34.9 |
| 30-39 | 70.4 | 29.6 |
| 40-49 | 68.3 | 31.7 |
| 50-59 | 66.5 | 33.5 |
| 60-69 | 63.3 | 36.7 |
| 70-79 | 54.5 | 45.5 |
| 80+ | 56.6 | 43.4 |
| All | 65.7 | 34.3 |
Table 5: Share of Case Fatality Ratio in India by age & Sex.
If one looks at the age specific case fatality rates, international evidence points to potential biological advantages for women that get blunted by gender disadvantages of women in India in seeking care early resulting in a higher risk of mortality in India. There are various underlying factors for such patterns in India like Men suffer from several lifestyle risk factors, a large proportion of women in India have poor nutritional status including both underweight and overweight prevalence as well as micronutrient deficiencies, the circumstances of health care access and affordability are also important issues which are shaped by contextual factors such as household socioeconomic status and gender roles and women are less likely to be accurately counted in death statistics as evidenced by women being historically undercounted in death statistics [6].
Covid 19 Vaccination in Elderly
In a phase 1, dose-escalation, open-label trial of a messenger RNA vaccine, mRNA-1273, which encodes the stabilized prefusion SARS-CoV-2 spike protein (S-2P) in healthy adults, expanded to include 40 older adults, who were stratified according to age in two groups of 56 to 70 years and ≥71 years and given two doses of either 25 μg or 100 μg of vaccine administered 28 days apart. The 100-μg dose induced higher binding- and neutralizing-antibody titres than the 25-μg dose, which supports the use of the 100-μg dose in a phase 3 vaccine trial [7].
Discussions
Globally, the population aged 65 and over is growing faster than all other age groups. According to data from World Population Prospects: the 2019 Revision, by 2050, one in six people in the world will be over age 65 (16%), up from one in 11 in 2019 (9%). The global population aged 60 years or over numbered 962 million in 2017, more than twice as large as in 1980 when there were 382 million older persons worldwide. The number of older persons is expected to double again by 2050, when it is projected to reach nearly 2.1 billion. India is estimated to have had 6% of the population over 65 years in 2019 [8].
The age distribution of COVID-19 infections in India is biased towards younger adults more than the hypothesis of uniform attack rate and susceptibility across the whole population would predict (Table 4) [9]. Separating the roles of spatially non-uniform epidemic seeding, age stratified attack rates, co-morbidities, and other factors, needs more detailed data. This, observation can be combined with age stratified IFR to model the age distribution of fatalities [10]. Such a model agrees with observation. Since the observation is conditioned on the distribution of infections, no biases are expected. It is observed that women are half as likely to be infected by COVID-19 as men. There is an interesting age structure to this ratio, with significantly lower infection rates for women between puberty and menopause. The relative importance of sex-linked disease resistance and differential attack rates needs to be clarified with follow up studies. The data for the sex ratio of COVID-19 fatalities does not exhibit any age structure.
The age structure in the count of infections is not proportional to that in the population, indicating the role of either co-morbidity or differential attack rate. There is a strong age structure in the sex ratio of cases, with the female to male ratio being about 50% on average. The ratio drops between puberty and menopause. No such structure is visible in the sex ratio of fatalities. The overall age distribution of fatalities is consistent with a model which uses the empirical age structure of infections and a previous determination of age structured IFR. The average IFR for India is then expected to be 0.4% with a 95% CrI in [0.22%, 0.77%].
The age distribution of COVID-19 infections marginalized over sex is shown in Figure 1. For comparison, the age distribution from the 2011 census is also shown. Apart from the first two age bins, infections fall faster than the population. Past census data indicate a slight flattening of the age distribution over the years. Correcting for the years passed since the last census is therefore likely to mildly flatten the distribution further. As a result, there is a clear difference between the age distribution of COVID-19 infections and the general population. Younger member of the population is more likely to be infected than a model with constant attack rate would predict. Further work is needed to disentangle the effects of differential attack rate and susceptibility to the infection.
For Indian women, these divisions correspond to the median ages of puberty and menopause. The female to male ratio for COVID-19 infections and fatalities in these three age bins ( 0–13, 14–46, and 47) All the ratios are significantly smaller than unity, but the age dependence of the ratios for fatalities cannot be seen to have any age structure [11, 12].
Around six out of every 10 (62%) infections of the coronavirus disease (Covid-19) in India have been among people below the age of 45 years, but Covid-19 patients above 45 years of age account for nearly nine in 10 (87%) of all deaths, shows government data. People between the ages of 60 and 74 years, who are only 8% of the population, form the largest proportion of fatalities- 39%. Those older than 75 (2% of India’s population) account for 14% of the total Covid deaths. The unreleased case data from the Union ministry of health and family welfare, shows that more than half (54%) of the people infected in India are between the ages of 18 and 44, while half (50%) the people who succumbed to the disease are above 60 years of age. Most deaths- 50% is in the age group of 60 years and above, followed by 37% deaths among people between 45 years and 60 years in age [4].
Globally Covid 19 mortality is to a large extent determined by access to and quality of health care. Over 95% of these deaths occurred in those older than 60 years. More than 50% of all fatalities involved people aged 80 years or older. Reports show that 8 out of 10 deaths are occurring in individuals with at least one comorbidity, like overweight, Obesity, cardiovascular disease, CKDs hypertension, and Diabetes, a range of other chronic underlying conditions like Asthma, COPD etc.
Mortality for COVID-19 appears higher than for influenza, especially seasonal influenza. While clear understanding of the mortality due to COVID-19 will take some more , the data we have so far indicate that the crude case fatality ratio (the number of reported deaths divided by the reported cases) is between 3-4%, the infection mortality rate (the number of reported deaths divided by the number of infections) will be much lower. For seasonal influenza, mortality is usually below 0.1%.
The relative risk of dying from COVID-19 was higher for men than for women in almost all age groups in all countries and India (Table 4). The overall relative risk ranged from 1.11 (95% CI 1.01-1.23) in Portugal to 1.54 (95% CI 1.49–1.58) in France. In most countries, sex differences increased until ages 60–69 years, but decreased thereafter with the smallest sex difference at ages 80+. In all European countries, the CMRs increased with advancing age. The highest CMRs were found in England & Wales with 91.0 (95% CI 89.9–92.1) per 100,000 men and 72.4 (95% CI 71.4–73.3) per 100.000 women. High CMRs were also found in two Southern European countries, Italy (66.2, 95% CI 65.3–67.2 per 100,000 men and 45.4, 95% CI 44.7–46.2 per 100,000 women) and Spain (50.3, 95% CI 49.4–51.2 per 100,000 men and 37.2, 95% CI 36.4–38.0 per 100,000 women). The countries with the lowest mortality from COVID-19 were Norway (5.0, 95% CI 4.2–5.9 per 100,000 men and 4.3, 95% CI 3.6–5.2 per 100.000 women), Denmark (11.8, 95% CI 10.6–13.2 per 100,000 men and 8.9, 95% CI 7.9–10.0 per 100,000 women), and Germany (12.1, 95% CI 11.8–12.5 per 100,000 men and 9.5, 95% CI 9.2–9.8 per 100,000 women) . The patterns for the CMRs between February and June 2020 revealed an overall similar trend for men and women; however, higher CMRs were found for men than for women, particularly in Western and Southern Europe and India [9, 10].
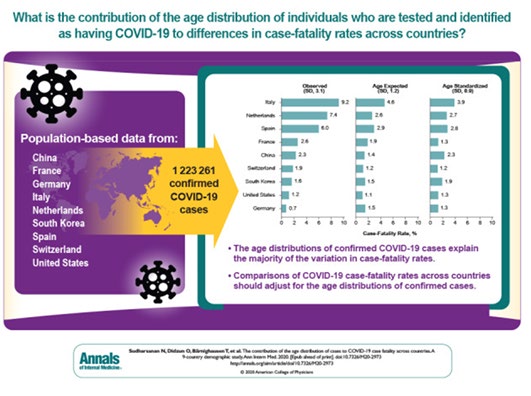
In another study reported by Public Health Emergency COVID-19 Initiative of American College of Physicians Public Health Emergency Collection of the authors argue that there was a wide variation in COVID-19 case-fatality rates (CFRs) across countries, attributable to the ages of individuals who were tested and identified. The authors draw attention to the importance of adjusting for the age distribution of cases of coronavirus disease 2019 before doing cross-country comparisons of case-fatality rates. This leads to uncertainty about the true lethality of the disease [10, 11].
A recent study conducted by the Indian Council of Medical Research (ICMR) that has concluded that Bacillus Calmette-Guerin (BCG) vaccine, also provided protection against Covid-19 among the elderly, particularly those in the 60-80-year age group. BCG increases "total antibody production in elderly" and enhances "adaptive immunity in elderly individuals which may prove beneficial against the Covid virus". Similar studies are now being promoted across India [14].
Summary
While the past few months have delivered a flood of data about the virus, the world has not yet fully understood about the pathology, the organs that these viruses can damage, presenting symptom and signs , possible diagnostics, complications, and primary causes of deaths. Some studies have made it clear that it will take years to fully make sense of SARS-CoV-2.
Selective testing and identifying of older cases considerably warp estimates of the lethality of COVID-19 within populations and comparisons across countries. Removing age distortions and focusing on differences in age-adjusted case fatality will be essential for accurately comparing countries’ performance in caring for patients with COVID-19 and for monitoring the epidemic over time.
Globally Covid 19 mortality is to a large extent determined by access to and quality of health care. Over 95% of these deaths occurred in those older than 60 years. Reports show that 8 out of 10 deaths are occurring in individuals with at least one comorbidity, like those with overweight, Obesity, cardiovascular diseases, hypertension, Diabetes, and a range of chronic underlying conditions like Asthma, COPD Pneumoconiosis, kidney failure (CKDs), etc.
The global health community is still on a learning curve to better understand the science behind COVID-19 herd immunity. A vaccine, on the other hand, offers a pathway to protect human capital and for countries to end the pandemic and resume stalled development priorities. Universal vaccine availability may take another year or two especially in developing countries. Therefore Individuals must practise physical distancing, clean their hands frequently, wear a mask as advised, cough and sneeze safely away from others, avoid crowds, and keep windows and doors open when they can’t meet friends and family outside.
The year 2020 first year of observance of ’Decade of Healthy Ageing’ is marred by Covid 19 Pandemic that will wipe off high risk elderly and some of 40 + year population with comorbidities and Covid 19 may attack will not survive to move in 60-65+ group. Those who survive will be strong enough to live for another decade. Coping mental health challenge may continue to be an issue.
India has enormous expertise in public health, health policy, and basic biology and have consistently been able to turn that expertise into new therapies, developing case management protocols, vaccine manufacturing and preventive measures. Much of that national expertise resides in government institutions NCDC, ICMR, AIIMS, Public Health Schools, and professional organizations Like IPHA, IAP. yet our leaders have largely chosen to ignore and even denigrate experts.
Way Forwards
There is a dire need to understand the epidemiology of the Covid 19 disease fully. The analysis of gender and age specific infection rates need for hospitalization, severity, complications and causes of deaths, the attack rates, hospitalization, and case fatality rates. Other technical analysis should look at association of BMI, pre-existing comorbidities, and access to and quality of health services. Countries should also prepare near-real-time data on highly vulnerable populations and their conditions, with a special focus on infection and death rates, poverty, joblessness, mental health, violence, hunger, forced labour, and other forms of extreme deprivation and abuses of human rights.
While practicing physical distancing elderly people need to find ways socialization over phones, video-consultations, and discussions to keep the mental health & their sprits high. Practice of Yoga may one other way of tiding the crisis.
Countries must revise their strategies and plans for the Decade of Healthy Ageing and Global rededication is desired after the pandemic.
Indian leaders need to choose to capitalize public health expertise and invest in Public Health Services for long time to come while building public private partnership of not for profit nature.
References
-
Leng J, Goldstein DR (2010) Impact of aging on viral infections. Microbes Infect 12(14-15): 1120-1124.
-
(2020) Overweight is a risk too, not just obesity, CDC Atlanta, USA, Times of India.
-
(2020) Age composition of population and Covid-19.
-
Linda Juel Ahrenfeldt, Otavova M, Christensen K, Lindahl Jacobsen R (2020) Sex and age differences in COVID-19 mortality in Europe. Res Sq pp: 61444.
-
(2020) Covid 19 Cases and deaths by age and sex.
-
(2020) 90% of those killed by Covid in India are older than 40, 69% are men, Sanchita Sharma, IST, Hindustan Times, New Delhi.
-
(2020) An mRNA Vaccine against SARS-CoV-2- Preliminary Report. NEJM.
-
(2020) India’s covid-19 count could be missing many women.
-
(2019) Population ages 65 and above (% of total population), World Bank estimates based on age/ sex distributions of UN Population Division’s World Population Prospects.
-
Sudharshanan N (2020) The Contribution of the Age Distribution of Cases to COVID-19 Case Fatality across Countries. Ann Intern Med Mpp: 20-2973.
-
David N Fishman (2020) Age is a critically important Number for COVID-19 Case Fatality. Ann Intern Med. M20-4048.
-
Tata Institute of Fundamental Research.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda