An Examination of the Efficacy and Background of the Covid-19 Vaccine: Comparative Analysis
Significance and Aim: The aim of this review is to instigate the existing literature on the efficacy levels of the administered Covid-19 pandemic vaccines. The review examines how the efficacy levels compare or contrast among the leading vaccines globally. The proposed value of the review is to indicate if the inoculation of the population has a significant value and impact on reducing exposure and risk of Covid-19 infection and severity of the disease. Methods: The review was developed as an ILR analysis. The search was made from 5 different databases. The findings were Scopus (103), Medline (78), Google Scholar (320), CINAHL (167), and WHO (201). By applying the review inclusion and exclusion criteria, the review settled on 21 articles included in the analysis. The findings were analysed thematically. Results and findings: The findings indicate that the vaccines analysed, the (i) Pfizer, (ii) Astra Zeneca, (iii) Johnson &, (iv) Moderna, can be categorised into two main levels, namely the mRNA vaccines and the carrier/ virus vector vaccines. The findings indicate that all the vaccines have a high efficacy index above the WHO threshold of 50% efficacy minimum. Pfizer has the highest efficacy based on the RCTs done at the manufacturing stage. Conclusion: In summary, the findings indicate the validity and value of vaccines in reducing the healthcare industry burden. The high efficacy levels on reducing the severity and hospitalisation needs allow for a reduced disease burden globally. Sensitisation is required for the global population base. Equally, more RCTs are required to test the efficacy of the existing vaccines against the emerging variants, such as the highly virulent delta variant.
Introduction
The ongoing global coronavirus disease 2019 (COVID-19) is caused by the severe acute respiratory syndrome coronavirus (SARS-COV-2) [1, 2]. Having been declared a global pandemic by the world health organisation (WHO) in March 2020, the pandemic has of august 2021 claimed over 4.24 Million deaths related to the illness and over 199 million positive cases reported globally. This makes it the deadliest global pandemic in the world’s history [3]. In partnership with global and national infectious diseases control organs, the WHO formulated proactive control and spread mitigation policies such as hand washing, social distancing, use of face masks, and reduced physical interactions. Although the measures have been critical in reducing the spread rates and protecting vulnerable groups such as those with underlying conditions and the elderly, they have not been effective in stopping the disease spread [1]. Some of the most virulent SARS- CoV-2 virus variants include delta, alpha, and beta variants. The long term mitigation of the pandemic has been linked to the development and roll-out of vaccines for the global population. It is estimated that with an over 60% inoculation with the Covid-19 vaccines, the world would achieve a herd immunity level allowing for the lifting of travel restrictions [4, 5]. The first mass vaccination programs kicked off in December 2020. To date, the WHO has approved at least 13 vaccines (across 4 platforms) and they have been administered globally [6].
Although the WHO undergoes a verification and vaccine testing stage, there have been challenges in the adoption of the vaccines globally. The challenges are linked to both the vaccine distribution inequality across the global regions and a negative attitude by the patients on the vaccines’ efficacy. On inequality, there has been rising outcry from the emerging and developing nations, mainly in Asia and Africa, on the shortage and challenges in accessing the vaccines due to a perceived over-ordering of the vaccines by the developed countries [7, 8]. Additionally, on the existing negative attitudes, there have been mass media and social media reports on the potential immediate short term and long term health effects from the Covid-19 vaccines inoculation. The surrounding misinformation has been linked to the low vaccine uptake in Europe and the USA developed countries. Nations such as Australia the U.K. have created mandatory policies for their essential workers to receive the vaccination as a condition of resuming to work [9, 10, 11]. There is a need to understand the vaccines’ efficacy and how the different vaccines compared and rank against each other on their efficacy levels. This is a basis for creating aura and scientifically proven data on the Covid-19 vaccinations, thus help in reducing the circulating misinformation on the vaccines globally [12].
Aim
The review investigates existing literature on the efficacy levels of the administered Covid-19 pandemic vaccines. The review examines how the efficacy levels compare or contrast among the leading vaccines globally.
Materials and Methods
The developed review is an integrated literature review. This allows for the evaluation of the existing literature and analysing and comparing the findings. The ultimate focus and aim of the review was to examine the existing vaccines efficacy levels [13]. This is through identifying the vaccines individual efficacy levels and how they compare or differ from each other. The realisation of the comparative analysis of the vaccines’ efficacy levels required the comparison of existing literature, thus adopting an integrated literature review (ILR) design. The approach applied in the review is to classify the vaccines based on the 4 platforms approved by the WHO and that are currently rolled out globally in a significant proportion. The review, based on the WHO vaccination data established that the leading vaccines with a majority of vaccinations globally were (i) Pfizer, (ii) Astra Zeneca, (iii) Johnson & Johnson, (iv) Moderna [6]. Although there are other vaccines under different stages of approval, such as the Sputnik V vaccine, the review focused on the five leading vaccines with the current highest number of vaccinations globally.
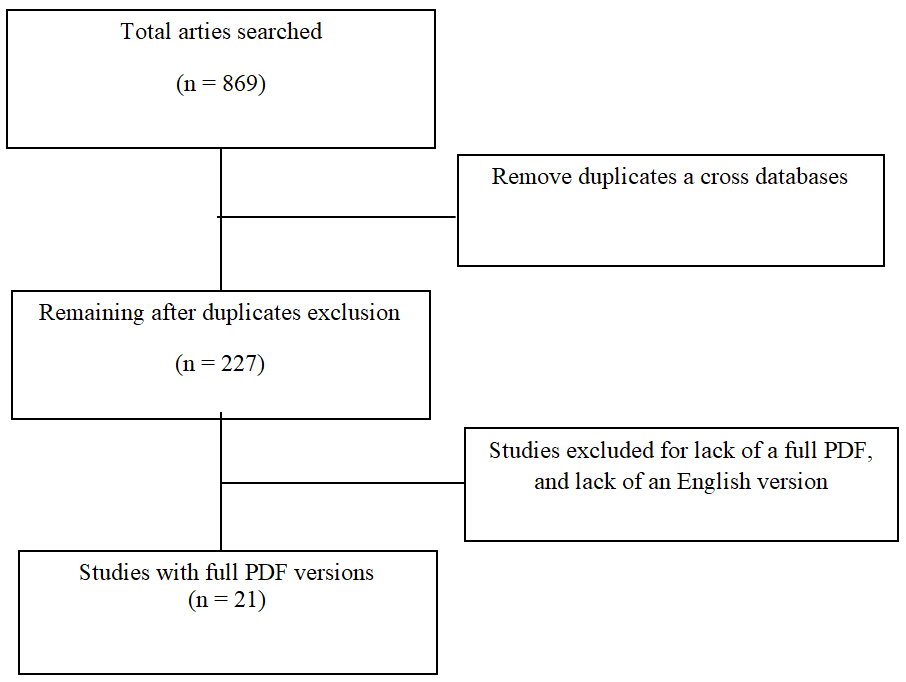
The study literature search was online and was based on five different databases. They included Scopus, Medline, Google Scholar, CINAHL, and WHO, respectively [14]. The databases were included based on their magnitude of health- related articles and the saturation of articles on the Covid-19 pandemic. The information search was developed online through the use of keywords and phrases. The review used the keywords’ Covid-19’ AND ‘vaccine’ AND ‘efficacy’ AND ‘compare’. There exists a high risk of misinformation on the vaccines and their efficacy index. Thus, the analysis focused on relying on and using only verifiable and accurate sources. The sources were predominantly limited to peer-reviewed studies, preferably the randomised control trials (RCTs), the WHO database and resources, vaccine manufactories official reports, and reliable industry and infectious diseases related literature and publications. Data published from late 2020 to the current was included [14]. All data published before the 2020 December mass vaccination roll-out was regarded as the trial and testing data on the efficacy and safety of the vaccine. Data published before the pandemic declaration as a global disaster in March 2020 was ignored as it was not related to the Covid-19 vaccination development and manufacturing process. On exclusion, all data not developed by any of the above sources were excluded from the review analysis. This also applied for all literature whose authorship was neither professional nor accredited to a reputable professional institution regarding health and infectious diseases control.
Additionally, duplicated articles, those lacking a full PDF and those not published in English, were excluded. From the searched findings and with the adoption of the inclusion and exclusion criteria, the study established 21 resources to be used in the analysis. This was from the initial search results of Scopus (103), Medline (78), Google Scholar (320), CINAHL (167), and WHO (201). The findings obtained were then analysed thematically with due reference and citation for all the information sources used in the analysis. The PRISMA figure as indicated below (Figure 1).
Results
The initial stages of examining a vaccine efficacy are based on the development of RCTs focused on examining how effective a vaccine is in proactively protecting the vaccinated population against a virus. The RCTs and the established efficacy levels from the basis for the vaccinations approval by the respective bodies both nationally and globally. The Covid-19 pandemic was viewed as a severe global pandemic with vaccinations required urgently. Consequently, the WHO set the efficacy level at 50% for a vaccine to be listed for emergency use to inoculate against Covid-19. Although this was set as the minimum with a projected aim of at least offering 50% protection to those vaccinated, the developed vaccines, based on the RCTs and the manufacturers, indicate a higher efficacy level [15, 16, 17]. An evaluation of the obtained findings indicated that the four major vaccines globally could be classified into two main categories, namely the mRNA vaccines and the carrier/ virus vector vaccines.
mRNA Vaccines
An analysis of Pfizer, one of the first mRNA vaccines to be approved, indicates that manufacturers reported an efficacy level of up to 95% effectiveness in preventing symptomatic Covid-19 pandemic infections after the second dose, up from 52% after the first dose. Additional RCTs have been developed since the vaccination approval for individuals 16 years and older [18, 19, 20]. The vaccine’s efficacy is based on two doses for full vaccinations that are ideally 21 days apart. A PHE analysis re-analysis indicated that the vaccine had an 89% efficacy rate for days 15 to 21 after the first dose and slightly before the full immunization second dose [21, 22]. Immediately after the first dose and 19<7 days after the second dose, protection from the first doses rose to up to 91% with a range of 74%-97%, respectively [23]. A real-world data based collection and analysis sampling over 44,000 people vaccinated with the Pfizer dose across the USA and globally indicted that the efficacy rate and protection against severe diseases declined to an estimated 84% efficacy level after six months of receiving the second dose. The study indicated a gradual 6% efficacy decline per month. The tests were on the alpha and the beta variants Hallas, et al. [21, 22].
The second analysed vaccine is the Moderna vaccine is an mRNA vaccine. Its initial RCTS indicated a 94.1% efficacy in preventing symptomatic infections in people who depicted no evidence of previous Covid-19 infections. However, the trials indicate a lower efficacy level for the people who were 65 years and older, with an efficacy level of 86% [24, 25]. In a real-world study conducted by the CDC, including over 3950 health care providers and first responders in the health care industry, the study indicated that the vaccine had an efficacy rate of 90% once they were fully immunized, especially 14 days after the second dose. The vaccine is administered in two doses that are ideally 28 days apart. The testing was on the alpha and the beta variants [26, 27].
The Career/Virus Vector Vaccines
The third analysed vaccine was the Johnson and Johnson (J&J) vaccine. Unlike the Moderna and the Pfizer vaccines, the vaccine is a carrier or a virus vector vaccine. Unlike a majority of the other vaccines, it requires a single shot for full inoculation against the Covid-19 disease. The vaccine is approved for those aged 18 years and above. The first phase of the vaccine RCTs conducted in the USA and two months apart indicated an overall efficacy of 72%, 86% against severe diseases [28, 29]. In a similar real-life study developed in South Africa, the FDA reported that the vaccine had an overall efficacy of over 64%, but a slightly higher efficacy against severe disease at 82% on a study developed using those injected with the vaccine in South Africa. The studies were on the alpha and the beta variants [30, 31].
Similar to the J&J vaccine, the Oxford AstraZeneca is a carrier vaccine. It is approved for injection to those 18 years and above. The full dosage includes two shots that are ideally 12 weeks apart. The recent trials on the vaccine’s efficacy were RCTs conducted at phase three of the vaccine manufacturing. The results indicated a 76% efficacy and effectiveness in reducing and lowering the risk of symptomatic disease and 100% efficacy against severe disease infection [20, 32]. This was at its peak 15 days after receiving the second booster dose (12 weeks or more after the first dose). The efficacy index was higher at 86%for those aged 65 years and above. The vaccine efficacy has been reported as higher against the alpha and beta variants than the delta variants [11, 33]. For instance, in a study developed in February 2021, findings indicated a 74.6% efficacy against the Alpha variant. This was slightly higher than a recent study showing 60% efficacy against symptomatic disease for the delta variant. However, the efficacy against hospitalisation remains high at 93%, even against the delta variant [4].
Discussion
A critical analysis of the obtained findings indicates that all the examined vaccines had an efficacy index higher than the set 50% efficacy for approval by the WHO. This is a preliminary indication that the vaccines are of value to society [34]. Although an ideal efficacy would be one that allows for 100% protection, the WHO argued that due to the severity of the Covid-19 pandemic and its impacts on the society and economy globally, the offering of protection for at least 50% of the immunised population is a safe option to allowing for the reduction on the healthcare industry burden [35, 36]. Of the four examined vaccines, it is clear that the four vaccines had high efficacy in reducing hospitalisation and the risk of severe infections. One of the challenges facing global healthcare at the initial pandemic stages was the risk of overburdening the healthcare sectors globally. An analysis and case studies of nations such as Italy and France indicate the pandemic risk of hospitalisations overrunning the healthcare industry [37]. This was equally experienced in other parts globally, including the USA and Europe. One of the core challenges was bed capacities and the lack of oxygen and ventilators globally. The lack of these spaces in hospitals led to exclusive and field hospitals set up to cater to the Covid-19 pandemic [38, 39]. However, with the vaccines rollout, there has been a significant reduction in the risk of severe cases and, as such, a reduction in the need for hospitalisations. This is a significant step in ensuring that those with underlying conditions and with severe infections have enough healthcare providers, healthcare facilities, and ventilators to serve them. This is a strategic move towards realising a reduced Covid-19 mortality rate [36, 40]. The fact that a significant proportion of the inoculated population does not require hospitalisation means a lower burden on the hospitals, allowing them maximum care for those in critical and severe infection stages. Thus, despite the perceived declining efficacy in reducing mild and moderate infections, the relatively high efficacy rates for the severe infections remain a key pillar validating the vaccinations.
Furthermore, the findings indicate the need for an understanding of the full immunization process. As illustrated, the vaccines protection optimality differs based on the number of shots and the days after the shots are received. For instance, for the Pfizer vaccine, it was established that protection and efficacy was highest 12 days after the second shot while AstraZeneca efficacy was highest 15 days and later after the second vaccination [41, 42]. This means that although inoculated with the full dosage for the vaccines, and understanding is imperative on the need for care and protection to ensure that the body gradually adapts and optimises to the vaccine benefits and efficacy against Covid-19 infections. Studies and case study reports indicate that a significant proportion of infections reported among the vaccinated population occurred between the first and second doses or slightly after the second doses due to the time required for the body to optimise on the vaccine protection.
Conclusion
The review findings indicate that the existing vaccines have a significant efficacy index. The results indicate a significant risk reduction for severe infections and the need for hospitalisations. This indicates that the use of vaccines plays a key role in reducing the healthcare industry burden globally. However, a challenge exists in the perceived declining efficacy index of the vaccines with the rise in new Covid-19 virus such as the highly virulent Delta variant first reported in India and the U.K. The findings indicate the need for further studies, RCTs and real clinical reports on the efficacy of the existing vaccines against the emerging virulent variations of the disease. This would inform the future for new vaccines or the progression of the existing vaccines based on the demonstrated efficacy levels.
Conflict of Interest
There is no conflict of Interest
Funding
The review was not funded
References
-
AlTakarli NS (2020) Emergence of COVID-19 infection: what is known and what is to be expected–narrative review article. Dubai Medical Journal 3(1): 13-18.
-
Kirksey E (2020) The emergence of COVID-19: a multispecies story. Anthropology Now 12(1): 11-16.
-
WHO (2021a) WHO Coronavirus (COVID-19) Dashboard.
-
Lopez Bernal J, Andrews N, Gower C, Gallagher E, Simmons R, et al. (2021) Effectiveness of COVID-19 vaccines against the B. 1.617. 2 (Delta) variant. New England Journal of Medicine 385: 585-594.
-
Planas D, Veyer D, Baidaliuk A, Staropoli I, Guivel Benhassine F, et al. (2021) Reduced sensitivity of SARS- CoV-2 variant Delta to antibody neutralisation. Nature pp: 1-7.
-
WHO (2021b) Coronavirus disease (COVID-19): Vaccines.
-
Black M, Lee A, Ford J (2021) Vaccination against COVID-19 and inequalities–avoiding making a bad situation worse. Public Health in Practice 2: 100101.
-
Campos Matos I, Mandal S, Yates J, Ramsay M, Wilson J, et al. (2021) Maximising benefit, reducing inequalities and ensuring deliverability: Prioritisation of COVID-19 vaccination in the U.K. The Lancet Regional Health– Europe pp: 2.
-
Smith DT, Attwell K, Evers U (2021) Support for a COVID-19 vaccine mandate in the face of safety concerns and political affiliations: An Australian study. Politics pp: 02633957211009066.
-
Wise J (2021) Covid-19: Is the U.K. heading towards mandatory vaccination of healthcare workers?. pp: 373.
-
Wise J (2021) Covid-19: New data on Oxford AstraZeneca vaccine backs 12 week dosing interval. pp: 372.
-
Love AS, Love RJ (2021) Considering Needle Phobia among Adult Patients During Mass COVID-19 Vaccinations. Journal of Primary Care & Community Health, 12: 21501327211007393.
-
Burke LA, Hutchins HM (2007) Training transfer: An integrative literature review. Human resource development review 6(3): 263-296.
-
Bekhet AK, Zauszniewski JA (2012) Methodological triangulation: An approach to understanding data. Nurse researcher 20(2): 40-43.
-
Lin DY, Zeng D, Mehrotra DV, Corey L, Gilbert PB (2020) Evaluating the efficacy of COVID-19 vaccines. medRxiv.
-
Paltiel AD, Schwartz JL, Zheng A, Walensky RP (2021) Clinical Outcomes of a COVID-19 Vaccine: Implementation Over Efficacy: Study examines how definitions and thresholds of vaccine efficacy, coupled with different levels of implementation effectiveness and background epidemic severity, translate into outcomes. Health Affairs 40(1): 42-52.
-
Mehrotra DV, Janes HE, Fleming TR, Annunziato PW, Neuzil KM, et al. (2021) Clinical endpoints for evaluating efficacy in COVID-19 vaccine trials. Annals of internal medicine 174(2): 221-228.
-
Mahase E (2020) Covid-19: Pfizer vaccine efficacy was 52% after first dose and 95% after second dose, paper shows. pp: 371.
-
Chagla Z (2021) In adults, the Oxford/AstraZeneca vaccine had 70% efficacy against COVID-19> 14 d after the 2nd dose. Annals of Internal Medicine 174(3): JC29.
-
Chagla Z (2021) The BNT162b2 (BioNTech/Pfizer) vaccine had 95% efficacy against COVID-19≥ 7 days after the 2nd dose. Annals of Internal Medicine 174(2): JC15.
-
Hallas D, Spratling R, Fletcher J (2021) Methodological Analysis: Randomized Controlled Trials for Pfizer and Moderna COVID-19 Vaccines. Journal of Pediatric Health Care 35(4): 443-448.
-
Tenforde MW (2021) Effectiveness of Pfizer-BioNTech and Moderna Vaccines Against COVID-19 Among Hospitalised Adults Aged≥ 65 Years-United States. MMWR, Morbidity and mortality weekly report pp: 70.
-
Badiani AA, Patel JA, Ziolkowski K, Nielsen FBH (2020) Pfizer: The miracle vaccine for COVID-19?. Public Health in Practice 1: 100061.
-
Doshi P (2020) Peter Doshi: Pfizer and Moderna’s” 95% effective” Vaccines—Let’s Be Cautious and First See the Full Data. BMJ Opinion.
-
Richman DD (2021) COVID-19 vaccines: implementation, limitations and opportunities. Global Health & Medicine 3(1): 1-5.
-
Dyer O (2021) Covid-19: Moderna and Pfizer vaccines prevent infections as well as symptoms, CDC study finds. BMJ: British Medical Journal pp: 373.
-
Thompson MG, Jefferey L, Allison LB, Harmony LN, Sarang KT, et al. (2021) Interim estimates of vaccine effectiveness of BNT162b2 and mRNA-1273 COVID-19 vaccines in preventing SARS-CoV-2 infection among health care personnel, first responders, and other essential and frontline workers—eight U.S. locations. Morbidity and Mortality Weekly Report 70(13): 495- 500.
-
Mahase E (2021) Covid-19: Novavax vaccine efficacy is 86% against U.K. variant and 60% against South African variant.
-
Moore JP (2021) Approaches for optimal use of different COVID-19 vaccines: issues of viral variants and vaccine efficacy. Jama 325(13): 1251-1252.
-
Bian L, Gao F, Zhang J, He Q, Mao Q, et al. (2021) Effects of SARS-CoV-2 variants on vaccine efficacy and response strategies. Expert review of vaccines 20(4): 365-373.
-
Livingston EH, Malani PN, Creech CB (2021) The Johnson & Johnson Vaccine for COVID-19. Jama, 325(15): 1575- 1575.
-
Knoll MD, Wonodi C (2021) Oxford–AstraZeneca COVID-19 vaccine efficacy. The Lancet 397(10269): 72-
-
Hung IF, Poland G (2021) Single-dose Oxford– AstraZeneca COVID-19 vaccine followed by a 12-week booster. The Lancet 397(10277): 854-855.
-
Sadoff J, Gray G, Vandebosch A, Cárdenas V, Shukarev G, et al. (2021) Safety and efficacy of single-dose Ad26. COV2. S vaccine against Covid-19. New England Journal of Medicine 384(23): 2187-2201.
-
Moghadas SM, Vilches TN, Zhang K, Wells CR, Shoukat A, et al. (2021) The impact of vaccination on COVID-19 outbreaks in the United States. medRxiv.
-
Roghani A (2021) The Influence of Covid-19 Vaccine on Daily Cases, Hospitalization, and Death Rate in Tennessee: A Case Study in the United States. medRxiv.
-
Sah P, Vilches TN, Moghadas SM, Fitzpatrick MC, Singer, et al. (2021) Accelerated vaccine roll-out is imperative to mitigate highly transmissible COVID-19 variants. EClinicalMedicine 35: 100865.
-
Bartsch SM, O’Shea KJ, Wedlock PT, Strych U, Ferguson MC, et al. (2021) The Benefits of Vaccinating With the First Available COVID-19 Coronavirus Vaccine. American journal of preventive medicine 60(5): 605-613.
-
Vilches TN, Zhang K, Van Exan R, Langley JM, Moghadas SM (2021) Projecting the impact of a two-dose COVID-19 vaccination campaign in Ontario, Canada. Vaccine 39(17): 2360-2365.
-
Dagan N, Barda N, Kepten E, Miron O, Perchik S, et al. (2021) BNT162b2 mRNA Covid-19 vaccine in a nationwide mass vaccination setting. New England Journal of Medicine 384(15): 1412-1423.
-
Chandir S, Siddiqi DA, Mehmood M, Setayesh H, Siddique M, et al. (2020) Impact of COVID-19 pandemic response on uptake of routine immunisations in Sindh, Pakistan: an analysis of provincial electronic immunisation registry data. Vaccine 38(45): 7146-7155.
-
Lambert PH, Ambrosino DM, Andersen SR, Baric RS, Black SB, et al. (2020) Consensus summary report for CEPI/ BC March 12–13, 2020 meeting: assessment of risk of disease enhancement with COVID-19 vaccines. Vaccine 38(31): 4783-4791.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda