Intestinal Resection as the Last "Salvage" Option in the Management of Difficult Enter Atmospheric Fistulas
Introduction: The case of a patient with difficult-to-manage entero-atmospheric fistulas is presented, who received prolonged medical treatment with multiple complications and reinterventions, to whom intestinal resection surgery was proposed as the last step of management as a definitive solution to his disease. Clinical Case: This is a 62-year-old male patient from a rural area who, after blunt trauma to the abdomen and acute perforating abdomen, underwent several surgeries which as a complication presented the establishment of several enter atmospheric fistulas, difficult to manage due to multiple intercurrences during his hospitalization and to whom intestinal resection was considered as a solution. Evolution: The patient underwent surgery and it was possible to resect the intestinal segment with the fistulas in a hospital abdomen, in addition to reestablishing intestinal transit by reconnecting the iliostomy that the patient presented. His evolution was good, recovering intestinal transit and restarting his nutritional recovery, receiving discharge. at 100 days of hospitalization. Conclusions: Surgery is a useful tool for patients with prolonged management of entero-atmospheric intestinal fistula, as a rescue maneuver for these patients.
Introduction
Three categories are used to define a fistula: anatomical, physiologic, and etiologic [1]. Small intestine fistulas constitute one of the greatest challenges in general surgery, it is an epithelialized connection between the small intestine and the skin [2], within these fistulas the most serious is called enter atmospheric fistulas and constitute a true challenge of the multidisciplinary management for any hospital, due to complications and prolonged stay [3, 4]. Studies show that 80% of them are the product of interventions in patients and only 20% occur spontaneously [5, 6, 7]. Fistulas not associated with surgery are caused by systemic diseases such as Crohn’s
disease, radiation enteritis, neoplasms, trauma, or ischemia [1, 2, 5]. Physiologically, low-output fistulas drain less than 200 ml/day, high-output fistulas drain more than 500 ml/day, and medium-output fistulas between 200 and 500 ml/day. It is a condition that requires a prolonged hospital stay due to complications such as electrolyte imbalance, malnutrition, metabolic disorders, psychological affectation of the patient and his family, sepsis, and even death, for which it represents a serious pathology that the surgeon must face during the exercise of his profession and the medical team, during the hospital stay [1, 3].
The management of patients with enterocutaneous fistula (ECF) requires an interdisciplinary approach and represents a significant challenge for surgeons, gastroenterologists, intensive care providers, wound/ostomy care specialists and nutritional support physicians, nurses, psychologists; results for a long time difficult to treat in clinical settings. Current approaches may not achieve satisfactory results, including surgery, antibiotics, and nutritional support [4].
Adherence disease is the most frequent disorder of small bowel obstruction, the definitive confirmation of this etiology is made during the surgical treatment. Zuhlke, et al. classifies adhesions as presented in the following Table 1 [8].
| Degree | Definition |
|---|---|
| Yo | Loose, transparent, and easily sectioned |
| II | Lax, White, and more difficult to section, initiating vascularization |
| II | Firm, possible lysis by dissection, clear vascularity |
| IV. | Integrated, with a difficult plane of dissection between the viscera and the mesh. imminent organ injury |
Table1: Zuhlke classification.
Postoperative adhesions are the cause of considerable morbidity and their prevention can be considered a public health problem [9]. These complications have repercussions on the patient and their relatives due to the physical, work, social, economic and psychological inconveniences leading to poor social integration.
The following article presents a case, important for our institution, where all clinical and conservative management resources were exhausted, for which reason surgery was used as a salvage for the patient.
The objective of this research is to report the evolution and clinical and/or surgical treatment of a patient with a prolonged hospital stay, through intestinal resection as the last “salvage” option in the management of difficult enter atmospheric fistulas.
Clinical Case
The case of a 62-year-old male patient with no level of education, coming from and residing in Cañar-Ecuador, farmer occupation is described.
Surgical history: he presented multiple interventions in the abdominal cavity, admitted to a second-level hospital, with a picture of intense, diffuse, colicky abdominal pain, plus lack of elimination of gases and feces, with a diagnosis of acute perforating abdomen, intestinal resection was performed at 50 ccs of the ileocecal valve plus ileostomy preparation. After five days of hospitalization and with no apparent improvement, the patient’s relatives requested discharge and he was brought to a tertiary hospital, where, followed by an assessment by the surgeon on duty, he underwent surgery due to acute abdominal pain. perforation, an exploratory laparotomy was performed, with the discovery of multiple adhesions, flanges, and intestinal loop perforation. During his evolution in our hospital, the patient presented intestinal fluid leaking from the wound, a high-output intestinal fistula, and poor general condition, managed with multiple cavity washes, an open abdomen, and drains, in addition to guided broad-spectrum antibiotic therapy. with crops and nutritional support.
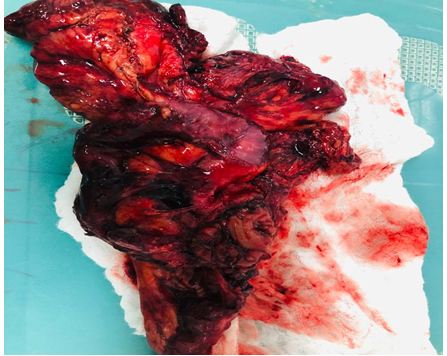
The patient required a total of 9 interventions and finally consolidated enter atmospheric fistulas that were difficult to manage with outputs above 1500 ml per day, as well as skin, hydroelectrolyte, and metabolic complications, as well as liver function disorders induced by parenteral nutrition that required to cover their basal needs and losses, for this reason, and after a 3-month hospitalization, a new laparotomy was proposed to the patient and his family as a last resort, with adherenciolysis and resection of the intestinal segments compromised by the Antero-atmospheric fistula where evidenced (Figures 1-3) a hostile abdomen with seven fistulas, the largest diameter being 2 ccs, weak fascia, and a severe adhesion syndrome with firm Zulhke type IV adhesions [9].
Exploration with intestinal resection and side-to-side anastomosis was successfully performed giving continuity to intestinal transit and, in addition, closure of the abdominal wall with dissection of the aponeurosis, achieving total closure of the wall and placement of Jackson Pratt drains (one in the cavity abdominal next to the anastomosis and another at the level of subcutaneous cell tissue).
After the intervention, the patient presented a good evolution with enteral nutritional support and physiotherapy that allowed him to recover, and was finally discharged 103 days after arriving at our center. Controls were carried out after discharge, due to dehiscence of the wound due to seroma and closure by secondary intention after two months of outpatient treatment, at the outpatient appointment 6 months (Figure 4) after hospital discharge with nutritional recovery and Satisfactory return to daily activities.

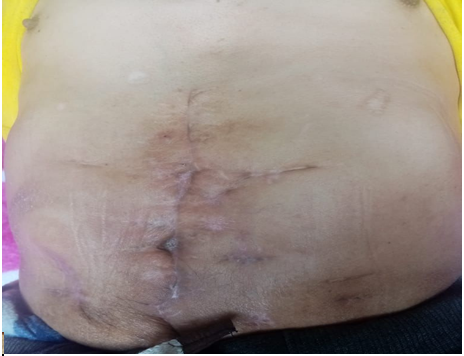

Source: Photographs taken by the authors. Figure 4: Post-surgical wound.
Discussion
The case of a patient with a diagnosis of the acute perforating abdomen was presented, after several interventions ended up with a catastrophic abdomen and multiple intestinal fistulas consolidating an enter atmospheric fistula, he received conservative clinical management with parenteral nutrition, metabolic, and infection control, in addition of multiple reinterventions with strategies such as the open abdomen and drains during a period of 3 months; Given the persistence of intestinal leakage through multiple orifices and with a high cost, an intestinal resection of the compromised segments was chosen as a rescue maneuver for the patient with good evolution and improvement. Regarding this case, it is mentioned that the flanges and adhesions are pathologically constituted by the union of the opposite surfaces of a wound and are responsible for 75% of the causes of intestinal obstruction; According to estimates in the United States, more than 300,000 patients are operated every year for this reason [10], these fistulas increase as there are more admissions to the abdominal cavity, increasing the risk of presenting a fistula, which depending on the area of the digestive tract has different implications; Inside the abdomen, the picture of an intestinal fistula can be very dramatic despite the control of the mainstays of the treatment, such as: the patient’s nutritional status, infection control, and metabolic control. enterocutaneous fistulas and enter atmospheric fistulas to which other factors are associated, such as tachycardia, fever, peritoneal irritation, leukocytosis, neutrophilia, and hypokalemia [11, 12].
Enterocutaneous fistulas (ECF) and enter atmospheric fistulas (EAF) are difficult complications that arise mainly after abdominal surgical procedures. Effective management of patients with these disease states includes surgical, pharmacotherapeutic, and nutritional interventions, ie a multidisciplinary approach [11, 13, 14].
Therefore, the intervention of nursing, nutrition, and rehabilitation, for the recovery of the patient is representative.
The treatment of fistulas is then a challenge for the multidisciplinary team that manages these patients in hospitals, so according to Quinn et.al, where sand identified a total of 286 enterocutaneous fistulas in 278 patients, with a mean age of 64 years (20-96 years), a total of 154 patients resolved with aggressive non-surgical management and 46 died before resolution, in addition, the hospital mortality was 19.1% (53/278) and 30-day postoperative mortality from definitive surgery was 9.8% (5/51) [15]. The study of a 77-year-old patient who developed a high output enterocutaneous fistula after several urgent surgeries, due to complications in the postoperative period of a complex eventronplasty and urgent right hemicolectomy due to a diagnosis of intestinal subocclusion and parastomal hernia. Initial management was performed with negative pressure therapy [16].
Kaska M, et al. [17] shows a set of eighteen patients who were successfully treated surgically and cured, enjoyed relatively good convalescence after surgery and returned to a satisfactory standard of living from the point of view of organ function. and the psychosomatic state. For it; “Care for people with enterocutaneous fistulas has an interdisciplinary approach based on five pillars: sepsis prevention and control, hydroelectrolyte imbalance, malnutrition prevention, effluent control, and peri wound skin care” [18].
The aforementioned is related to the recovery of the clinical case under study, where up to six months later, in the follow-up in the controls by outpatient clinic and the cures, the patient recovered his nutritional and emotional state, including his family and social life.
The majority of patients with high-strength enterocutaneous fistulas can be submitted to salvage surgery, avoiding prolonged complications, hospital expenses, and psychological damage to the patient and family.
In our case, all instances of conservative treatment were exhausted, however, given the intestinal failure conditioned by the high output of the fistula and the general commitment that the patient is presenting, intestinal resection was taken as a last resort, the objective of which is to resect the entire diseased intestinal segment [13, 14, 15] to restore its continuity, this surgery has a high rate of fistula recurrence and the appearance of significant intestinal failure, the last resort is small intestine transplantation; however, it is not available in our setting.
The study of this case provides a valuable resource in definitive surgery, once the patient has been stabilized or for patients who can no longer be managed due to the high debt and evolution that conditions a prolonged hospitalization, total parenteral nutrition, in long periods, and multiple problems. of handling caused in the patient and the care of the area exposed by the fistulas.
Conclusions and Recommendations
- Enteroatmospheric fistulas constitute a pathology with high morbidity and mortality, therefore, it is essential to make a timely diagnosis in order to adopt adequate interdisciplinary, clinical, and/or surgical management.
- The prolonged hospital stay causes emotional exhaustion in the patient and family, however, the cooperation and absolute predisposition of the patient under study were essential to achieve a positive result in the face of a rather bleak prognosis.
- Surgery with resection of the compromised segments is the last option in the management of fistulas in the face of chronicity and lack of closure with conservative management and initial control.
- The advantage of this surgical treatment is to reduce complications, hospital stay, and public health costs, so it is recommended, at the discretion of the surgeon, to make the best decision.
- We are proud as an Institution to be able to treat this diagnosis and return the patient to health and his return to the family and society.
- Financing Self-financed
- Authors’ Contribution
GM, FB, LC, PC, CR, RM: design, analysis and interpretation of the data, drafting of the manuscript, and approval of the final version.
- Conflict of Interests The authors declare no conflict of interest.
- Ethics Approval and Participation Consent The authors have the patient’s informed consent for the publication of the clinical case and its images.
References
-
Galindo F (2020) Digestive Surgery Encyclopedia: Enterocutaneous fistulas. Chapter 3, pp: 255.
-
McNaughton V (2010) Summary of best practice recommendations for management of enterocutaneous fistulae from the Canadian Association for Enterostomal Therapy ECF Best Practice Recommendations Panel. Rev J Wound Ostomy Continence Nurs 37(2): 173-184.
-
Graf JDP, Kumpf VJ, Aguilar Nascimento J, Hall AM, McKeever L, et al. (2020) ASPEN-FELANPE clinical guidelines: nutritional support of adult patients with enterocutaneous fistula. Rev Hospital Nutrition 37(4): 875-885.
-
Zhou H, Jin Y, Gu C, Chen Y, Xia J (2019) Bletilla striata promotes healing of enterocutaneous fistula: a case report. Rev. Baltimore Medicine 98(27): 1-5.
-
Kevin B, Sebastiano C (2021) Enterocutaneous Fistula.
-
Adaba F, Vaizey C, Warusavitarne J (2017) Management of Intestinal Failure: The High-Output Enterostomy and Enterocutaneous Fistula.Rev. Clinics in Colon and Rectal Surgery 30(3): 215-222.
-
Tang QQ, Hong ZW, Ren HJ, Wu L, Wang Gf, et al. (2020) Nutritional Management of Patients With Enterocutaneous Fistulas: Practice and Progression. Rev Frontiers in nutrition 7: 1-12.
-
Badrasawi M, Shahar S, Sagap I (2015) Nutritional Management in Enterocutaneous Fistula. What is the evidence?. Journal of Medical Sciences 22(4): 6-16.
-
Zühlke HV, Lorenz EM, Straub EM (1990) Pathophysiology and Classification of Adhesions. Peritoneal Adhesions 2: 29-34.
-
Correa M, Cleva VLG, Roberto MS, Raúl CE (2015) Intestinal obstruction secondary to postoperative adhesion formation in abdominal surgery. Rev Surgery and surgeons 83(4): 345-351.
-
Parli SE, Pfeifer C, Oyler DR, Magnuson B, Procter LD (2018) Redefining the “bowel regimen”: pharmacological strategies and nutritional considerations in the treatment of small intestinal fistulas. Rev AJS 216(2): 351-358.
-
Quinn M, Falconer S, McKee RF (2017) Management of Enterocutaneous Fistula: Outcomes in 276 Patients. Rev. World Journal of Surgery 41(10): 2502-2511.
-
Sanchez RMG (2017) Patient with chronic enterocutaneous fistula as an ileostomy presents low self- esteem and impaired skin integrity. Rev Dermatological Nursing 11(31): 43-50.
-
Schecter WP (2011) Management of Enterocutaneous Fistulas. Surgical Clinics of North America 91(3): 481- 491.
-
Gribovskaja-Rupp I, Melton GB (2016) Enterocutaneous Fistula: Proven Strategies and Updates. Clinics in colon and rectal surgery 29(2): 130-137.
-
Zabala López I, Navarro Antón C, Layunta Acero R (2019) Patient with enterocutaneous fistula and significant deterioration of skin integrity. Rev Nursing role 42(4): 10-15.
-
Kaska M, Chobola M, Skalska H (2018) Quality of life after reconstructive surgery for intestinal fistulas. Rev Medical Act 61(3): 103-107.
-
Caballero Vanegas C, Guerrero Ramirez M, Nieto L (2021) Nursing care, a fundamental factor for the evolution of people with enterocutaneous fistulas. Rev. Culture of Care 18(2): 41-51.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda