Techniques for the Analysis of Covid-19 Virus: State-of-the-Art and Future Prospects
SARS-CoV-2 was first reported in 2019 in China, which then inadvertently spread rapidly across the globe and by 2020 WHO has confirmed Covid-19 as a pandemic. Infections have been transmitted through airborne mechanisms leading to an exponential spread which called out for a strategic medical action plan to curtail the spread. Though WHO has established definite guidelines for containing the spread, such as isolation, social distancing, mandatory masks, sanitization, quarantines, international travel bans, and lockdowns. Early diagnosis and a large number of screenings were given a crucial role in the medical action plan, as they helped in delivering the medical aid and protecting the uninfected population. Various diagnostic methods have sprung up to detect Covid-19 with varying modes of sample collection, time of sampling, duration of test results, and accuracy. These diagnostics tests have been majorly based on a molecular and serological assays which are readily available, mass-produced, easy to handle, offer high accuracy, and shorter duration for results. This review article consolidates the functionality and efficacy of different diagnostic methods describing details of their functioning mechanisms, limitations, and accuracy of the test results. The role of artificial intelligence and deep learning algorithms have also been mentioned for future integrations to make the diagnostic tools efficient, reproducible, and robust. Auxiliary methods like Point care devices, biosensors, and lateral flow devices have also been used for quick diagnosis, which is however only qualitative in nature. Each technique is unique and has its limitations, but in testing times like a pandemic every technological development can be a game-changer when put to the right use.
Graphical Abstract
Abbreviations: CT: Computed Tomography; CXR: Chest X-Ray; SARS CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2; CoV: Coronavirus; ORF: Open Reading Frames; ACE2: Angiotensin-Converting Enzyme; ER: Endoplasmic Reticulum.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS CoV-2) virus comes under the virus classification Coronavirus (CoV), which are encapsulated, positive-sense, and SS- RNAviruses with nucleocapsid. Under the microscope, they appear to have a crown-like structure with a diameter of 60- 140nm and have distinguished protein spikes. Its genome is about 30,000 nucleotides long Zhou P, et al. [1, 2], with dimensions varying from 29.8 kb to 29.9 kb [3]. The complete structure of virion is shown in Figure 1, which includes Open reading frames (ORF) 1ab encoding ORF1ab polypeptides, making up about two-thirds of the genome.
One-third of crown consists of proteins structures: surface protein (s), envelop protein (E), Membrane (M), and Nucleoclaspid (N) proteins. It also comprises six additional attachment proteins, ORF3a, ORF7a ORF6, ORF7b ORF8 genes shown in Figure 2 [4, 5].
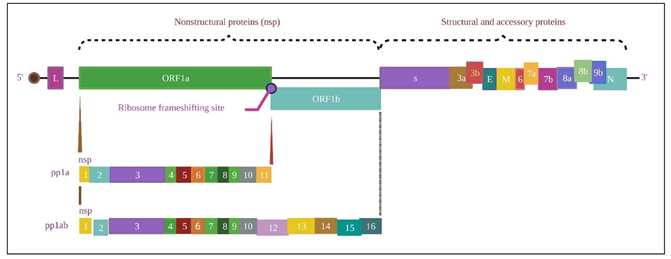
The spike surface glycoprotein is essential for binding to host cells where the spike protein of the virus attaches to the angiotensin-converting enzyme (ACE2) receptor and sometimes to CD209L as an alternative [6]. The infectious cycle begins as soon as the virus enters the respiratory tract and interacts with the epithelial membrane, as shown in Figure 3. S1 subunit recognizes ACE2 as a key entry into the host cell. It leads to conformational changes in S protein followed by proteolysis, where the protein is split into S1 and S2 subunits, after which membrane is combined in the S2 region. S2 has HR1 and HR2 domains, which form a 6-Hb mixture core that leads to cellular and viral interactions [7, 8].
ORF1a/1b, on the other hand, is translated into non-structural proteins [9]. Replication of the virus occurs together with the aid of RdRp (RNA-dependent RNA polymerase) encrypted by NSP12. The genomic replication occurs at cytoplasmic membranes. The transcript proteins are introduced into endoplasmic reticulum (ER), Golgi, after which translated RNA is crammed inside the capsid, as explained in Figure 3 N, E, M, S parts of genome form capsid, envelope, membrane, and spike[10, 11]. Understanding genomics and proteomics of viruses is crucial for developing molecular diagnostic techniques which are elaborated in this paper.
![Figure 3: S1 subunit recognizes ACE2 as a key entry into the host cell. It leads to conformational changes in S protein followed by proteolysis, where the protein is split into S1 and S2 subunits, after which membrane is combined in the S2 region. S2 has HR1 and HR2 domains, which form a 6-Hb mixture core that leads to cellular and viral interactions [7,8].](/fulltextimages/12456/fig_3.png)
Stage of Infection, testing scenario, and testing types are essential to determine the excellence of the specimen [12]. The upper respiratory tract samples, such as anterior nasal swabs, oro-pharyngeal swabs, nasopharyngeal swabs, nasopharyngeal aspirates, and mid turbinate swabs, are taken for testing Zou L, et al. [13], when the patient is symptomatic Wolfel R, et al. [14], where the virus replicates actively in upper respiratory tracts [15]. Reliable results are seen when combinations of both nasopharyngeal and oro- pharyngeal swabs are considered [16, 17]. Samples from the lower respiratory tract are considered when a higher viral load is required for the test; this is suggested for a later course based on patient condition. The Blood specimens rarely contain SARS-CoV-2 viral load, and they cannot be used for molecular tests [18]. However, blood samples can be taken for immunological assays to study the rise in antibodies. According to World Health organisation (WHO), they cannot be applied as a standalone diagnostic for SARS-CoV-2 disease. Faecal samples can also be taken from severely ill patients or patients from the second week of infection. Some anal samples showed positive results, while respiratory samples tested negative [14, 19, 20].
During the course of the pandemic in the past two years many variants of concern have emerged that have mutated from the initially sequenced strain. India was affected by two predominant variants Delta (B.1.617.2) which was first detected in January 2021. Later on, in November 2021, an omicron (B.1.1.529) was observed which is very close to the gamma variant, with 46 mutations with 15 mutations in spike protein Brooks ZC, et al. [21], and it showed stronger binding to the ACE receptor [22]. As the spread is across all the countries worldwide with new variants emerging with multiple mutations new and faster diagnostic technologies are required [23]. Laboratory diagnostics play a vital role in a pandemic. Diagnostic tests for SARS-CoV-2 are broadly categorized into two types: Serological tests and Molecular tests. Scientists have made great efforts to develop accurate, easy-to-use diagnostic tests. Latest technologies have improved diagnostic performance, increased specificity, sensitivity, and reduced time with particular attention to repeatability, cost of equipment, scope, reagent usage, convenient use, and effectiveness. This review summarises the various techniques and latest advancements in diagnostic procedures to screen, diagnose, and follow up on COVID-19. Promising technologies in detection with their advantages and disadvantages are discussed. All the figures in the manuscript were drawn using bio render software premium version.
Various Testing Techniques of Covid-19
Diagnostic tests are broadly classified into two types: Molecular tests and Serological tests [24]. Furthermore, imaging techniques like Computed tomography (CT) scans, chest X-ray (CXR), and ultrasound are available to confirm COVID-19, differentiate it from pneumonia, and understand the severity of the disease. Recently AI has been used for faster diagnosis. (Point of care) POC devices are being developed with cutting-edge technology to aid robust diagnosis. All of these are discussed in detail in the following sections. An overview of the diagnostic tests is given in Table 1.
| Diagnostic technique | Advantage | Disadvantage |
|---|---|---|
| Next-generation sequencing (NGS) | Unknown virus detection | Long turnaround time |
| viral mutation and evolution can be detected. | Expensive and complicated | |
| RT-PCR | High sensitivity and specificity | An experienced person is required; false positives can occur. Need a high viral sample to test (181) |
| Reverse transcription loop-mediated isothermal amplification (RT-LAMP) | On-site detection, low cost, minimum steps | Low throughput |
| Enzyme-linked immunoassay (ELISA) | High throughput, low cost | Easily contaminated time-consuming, an active infection cannot be detected in most cases |
| Ineffective in the early stages of infection, not approved by many authorities | ||
| Clinical Laboratory Improvement Amendments (CLIA) | Higher sensitivity than ELISA, reproducible, automated | Bulky equipment required |
| Lateral flow immunoassay (LFIA) | Low cost, simple operation | Low sensitivity |
Table1: Overview of various diagnostic tests with advantages, and disadvantages along with their applications.
Molecular Tests
RT-PCR: RT-PCR is the gold standard for SARS-CoV-2 detection, recommended by WHO and Centers for Disease Control and Prevention (CDC). It is a type of PCR method technologically advanced for genomic RNA detection. The samples for the test are attained from the upper and lower respiratory tract or stool [10]. The mechanism of testing involves the following steps which is clearly shown in Figure 4. First, complementary DNA (cDNA) is generated from the sample RNA through RNA-dependent DNA polymerase, and then cDNA is amplified several times by PCR. DNA template, specific primer, deoxy-ribonucleotides, DNA polymerase, buffer solution, and quencher are added to the sample [25]. This endorses the attachment of probes amongst forward and reverse primers. Gene-specific primers lead the next reaction. Only the designated genome area is amplified, and the probes yield fluorescent signals in each amplification cycle to give an assessable reaction time. This intensity of fluorescent is computed and equated with positive and negative samples. RT-PCR has a sensitivity of 0.77 (95% CI- 0.71) and specificity of 0.988 (CI- 0.933-1.000) [26, 27].
![Figure 4: First, complementary DNA (cDNA) is generated from the sample RNA through RNA-dependent DNA polymerase, and then cDNA is amplified several times by PCR. DNA template, specific primer, deoxy-ribonucleotides, DNA polymerase, buffer solution, and quencher are added to the sample [25]. This endorses the attachment of probes amongst forward and reverse primers. Gene-specific primers lead the next reaction. Only the designated genome area is amplified, and the probes yield fluorescent signals in each amplification cycle to give an assessable reaction time. This intensity of fluorescent is computed and equated with positive and negative samples. RT-PCR has a sensitivity of 0.77 (95% CI- 0.71) and specificity of 0.988 (CI- 0.933-1.000) [26,27].](/fulltextimages/12456/fig_4.png)
Over two years, different viral gene targets have been adopted by various countries. Mainly five genes are targeted, RdRp gene, N gene (nucleocapsid gene), E gene (envelope gene), S gene (spike gene), and ORF1b/ORF8 region. China relies on ORF1ab and N genes. Japan targets the N gene and spike protein. India and Germany aim for RdRP, E, and N genes. US-CDC recommends 3 RT-PCR reactions aiming at the N gene. The other set detects all beta- CoVs, whereas two are specific towards SARS CoV-2 infection validation altogether, three must be positive [19].
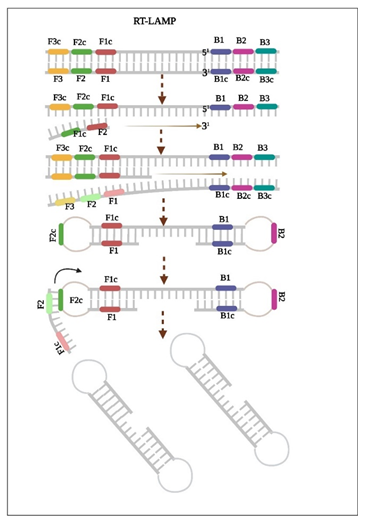
RT-LAMP: Loop-mediated Isothermal Amplification is the newest technique of gene amplification assay [28]. This method employs six different primers to recognize desired regions of the gene. Amplification takes place at a constant temperature (63ºC), both amplification and detection take place in a single step. Samples of oropharyngeal and nasopharyngeal swabs are taken, and the following are added: primers, Bst DNA polymerase, reverse transcriptase, and pH indicator dye, along with separated sample RNA. Then the mixture is heated to 65 ºC for 60 min. pH decreases as the DNA amplification proceeds, causing a visible colour change [29]. The turbidity of magnesium pyrophosphate can also be visualized.
Additionally, any fluorescent dye (ethidium bromide, SYBR Greene, Calcein) can be added, showing fluorescence under UV. Sequence-specific visual detection can be done by adding polyethyleneimine, forming the insoluble product with high molecular weight LOOP amplified DNA [30]. The detection mechanism occurs in two steps, which are represented in Figure 5 first, reverse transcription of DNA is achieved, followed by DNA amplification [31]. For faster and more accurate detection, a nanoparticles-based biosensor method coupled with RT-LAMP was developed and can be in under 30 minutes [32, 33].
Huang C, et al. [24], designed LAMP for ORF1ab, N gene, and S gene for COVID-19 disease. LAMP is 100 times more specific than RT-PCR, directly attributed to several primers used in LAMP [34]. Zhen Luo, et al. 2022 enhanced LAMP by scheming serial primers that can spot extremely conservative areas, maximizing the presence of virus [35, 36]. Zhu X, et al. [32] developed multiplex reverse transcription loop-mediated isothermal amplification- based lateral flow biosensors (MRT-LAMP-LFB), which achieved the whole procedure in an hour. In this, ORF1ab and N genes were concurrently multiplied in a single tube reaction, where LFB was used to interpret the results [37]. To overcome the RNA elution step, Yugan He, et al. developed a one-tube colorimetric RT-LAMP assay containing Si- OH magnetic beads based on quick extraction and direct isothermal amplification in a single tube. The assay showed 100% agreement with the RT-PCR test [38]. Anto JUK, et al. [37] came up with capillary-based LAMP that uses half the quantity of reagents and a cost-effective procedure [39].
CLAP Assay: Advanced techniques combine LAMP with clustered regularly interspaced short palindromic repeats (CRISPR), such as the CLAP assay, which combines gold nanoparticles with Cas12a and RT-LAMP, is a one-of-a-kind colorimetric assay. It has a fundamental principle, initially the N gene is reverse transcribed using RT-LAMP, Cas12/ gRNA recognizes this sequence-specific gene and later the Cas12 enzyme cleaves linker ssDNA. This does not interact with gold nanoparticles (AuNP), and the colour remains red, whereas in the absence of RNA, the AuNP will cross-link AuNP-DNA1/2, and the colour will change to purple [40]. Vijay Lakshmi et al. 2021 developed the LAMP technique to detect the Delta variant of COVID-19. They downloaded SARS-CoV-2 and beta corona virus sequences from NCBI GenBank are used for computational tools like CLC Genomic workbench and Primer Explorer V5 for alignments and designing variant-specific primers, respectively [27].
RT-LAMP has 91.45% sensitivity and 90% specificity Ge A, et al. [41] with more or less the same accuracy as RT-PCR [42]. Clinical data reveals that RT-LAMP is highly reliable and equivalent to RT-PCR [19]. It has a fast processing time, minimal risk of specimen transfer, and can be performed within 30-60 min. Since it involves no denaturation step, it can be performed at a constant temperature with a heating block as the only external requirement, unlike PCR which requires PCR equipment [43]. Designing appropriate primers and accurate temperature is a challenge for precise detection.
Palm Germ Radar (PaGeR), another modification of the RT-LAMP device that provides rapid and simple detection of SARS-CoV-2, was developed. PaGeR platform has three parts:
- A heating part with two modules for virus inactivation and LAMP assay each.
- A programmed control part with a monitor and switch controls power, temperature, heat, and light
- The detection part has direct readouts from fluorescence detection from the readout window [44].
One-Pot RT-LAMP is a one-step novel approach that does not require RNA extraction that utilizes formamide and colorimetric RT-LAMP. A nasopharyngeal swab is used as a template, and primers specific to primers of the N gene (computational tools are used to design specific primers), Bst DNA polymerase mix, U reverse transcriptase are added along with 6% formamide. Formamide is used as a lysis buffer hence eliminating the RNA extraction step. After 45 minutes of incubation at 65°C, results are analyzed by a colour change or agarose gel electrophoresis. The entire process takes 45 minutes [45]. Different types of molecular tests are shown in Table 2.
| Assay | Targeted gene | Signal readout | Temperature and reaction time | Reference |
|---|---|---|---|---|
| RT-qPCR | ORF1b and N gene | fluorescent probes, colorimetric assay | 30min | Pardee K, et al. [45] |
| PaGeR RT-LAMP | N gene | Palm germ Radar | - | John AJUK, et al. [37] |
| RT-LAMP | RdRp | fluorescent probes, colorimetric assay | 15min | Sun Y, et al. [46] |
| Transcription-mediated amplification (TMA) | - | Gel electrophoresis, fluorescent probes, colorimetric assay | 40 min | Sun Y, et al. [46] |
| RT-RAP | N, S gene | fluorescent probes, colorimetric assay | 45 min | Brooks ZC, et al. [21] |
| RT-LAMP | N and E gene | fluorescent probes, colorimetric assay | - | Brooks ZC, et al. [21] |
| coupled solid-state nanopores | ||||
| One-Pot RT-LAMP | N gene | Colorimetric and gel electrophoresis | 65 ºC, 45min | Haq F, et al. [39] |
| LAMP coupled with solid-state nanopores | N and E genes | Nanopore digital counting Gel electrophoresis | 95 ºC, 45 min | Guo L, et al. [47] |
| o-LAMP | - | Fluorescence and electrochemical signal | 40 min | - |
| Nijmegen-Bethesda assay (NBA) | N and E gene | Multiplex detection | 40 ºC, 30 min | Sanchita B, et al. [48] |
| Magnetic modulation biosensing (MMB) | - | Fluorescence resonance energy- based hydrolysis probe | 30 min | Tang Z, et al. [49] |
Table 2: Different types of Molecular tests specifying the targeted gene.
Amplification Techniques
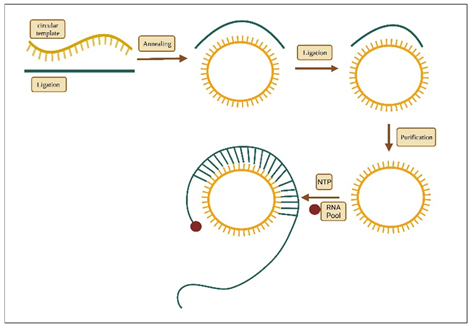
Rolling Circle Amplification (RCA): RCA is an alternative enzymatic isothermal method to identify the presence of viruses. The procedure of the test involves hundreds of DNA base pairs which are repeated and are compatible with circular template. As RCA exactly augments probe signal, the isothermal conditions are maintained properly rather than PCR and the test is performed with less number of reagents [50]. The step wise procedure of the test is shown in Figure 6.
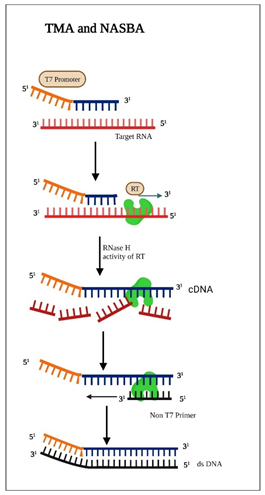
Transcription Mediated Amplification (TMA) and Nucleic Acid Sequence Based Amplification (NASBA): Both the TMA and NASBA methods are most commonly used tests which are performed in isothermal conditions. TMA uses two enzymes where as NASBA uses three enzymes. Both have higher amplification efficiency than PCR and reduce overall error frequency [51]. In the Figure 7 both TMA and NASBA are depicted.
CRISPR Diagnostics
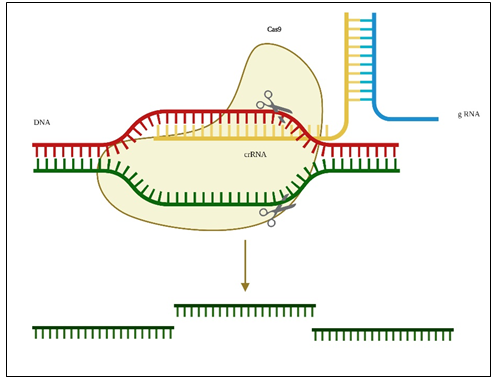
CRISPR was identified 30 years back in the bacterial genome. Distinctive areas of DNA named spacers are parted by short palindromic duplications accompanied by a cluster of Cas genes; later, these genes were known to function as natural adaptive immunity [52]. Later CRISPR-Cas systems were intended to cleave any region of target nucleic acid. Earlier, CRISPER-Cas systems were designed to diagnose Zika virus [53] and Staphylococcus aureus [54], it is vastly used as a gene-editing programmable tool. RT-PCR and other isothermal amplification methods have flaws, including low specificity, complicated reactions, high price, and require experienced personnel, CRISPER-Cas-based systems shown in Figure 8 overcomes these shortcomings of both techniques, it does not require isolation of nucleic acids or isothermal conditioning step, it requires minimal equipment, and is simple to use. It can tolerate nucleotide mismatches between/crRNA, leading to false positives. Still, it can recognize naturally variable genetic sequences providing the latest testing procedures crucial for mass testing and controlling the pandemic. There have been developments in diagnosis and readout steps [55, 56].
Samples for the CRISPER assay can be Nasopharyngeal, Oro-pharyngeal, Saliva, Sputum, Urine, and Stool. Viral RNA is isolated in three steps, i.e. Lysis, separation of unrequired fragments and proteins, RNA elution. To simplify this step, Chen FE, et al. [55] developed POC-CRISPR, a Cas-assisted assay, fully designed from sample preparation to readout [57]. It employs magnetic-based capture of nucleic acid that transports and purifies viral RNA towards downstream amplification and lateral flow detection within thermoplastic cartilage. And in another device, a redox probe conjugated with ssRNA immobilized on electrode surface with nanocomposite and gold nano-flower to enhance sensitivity and eliminate amplification [58]. Spin column isolation is another method to isolate RNA in which membranes are made up of glass fibre, derived silica, or ion exchange membranes are used to confine viral RNAs. Then a centrifugal force is used for the washing and assembling steps. The only disadvantage of this procedure is the membrane can be clogged with particulate matter.
In another method called Organic extraction, samples are homogenized in a phenol-containing solution and then centrifuged, during which the viral RNA is collected in an aqueous phase. This phase is recovered, precipitated, and rehydrated [59]. CRISPR/Cas technology is often combined with RT-LAMP for viral RNA extraction, followed by gene editing and probe attachment with Cas12 complexed with SARS-CoV-2 gRNA. For detection, techniques like DETECTOR (SARS-CoV-2 DNA Endonuclease-Targeted CRISPR Trans Reporter) employ lateral flow readouts for Cas12 fluorescence detection. This technique is widely used to target the N gene and E gene. iSCAN is RT-LAMP coupled with CRISPR-Cas12. RT-LAMP has an advantage over RT-PCR, it takes 45 minutes for the sample to give a result, whereas RT-PCR takes 4 hours, including manual extraction, no bulky instruments are required, and its limit of detection is ten times more when compared with RT-PCR. The use of metal nanoparticles can improve the stability of single-stranded RNA. Novel nano-bio sensors are developed to eliminate the target amplification step [60].
After amplification, to target SARS-CoV-2 Gene Region, desired primers and crRNAs are usually added, and the N gene, E gene, and ORF1ab genes are targeted [61]. Two types of Cas proteins are paired with CRISPER, i.e. Cas13 and Cas12 for SARS-CoV-2 diagnosis assays: Cas12 protein is programmed with CRISPER-RNA (crRNA), it specifically binds to DNA targets and cleaves the surrounding non- target reporters. The reports are usually quenched with a fluorophore label. Prior processing of reverse transcription is essential because Cas12 only bind to DNA molecule. It has a Limit of Detection (LoD) of 10 copies/uL, the procedure takes 40 min with advanced visual detection [62, 63]. CRISPER-Cas12 assays give sensitivity, specificity, and accuracy of 93.2%, 100%, and 97.2%, respectively, when compared with qRT-PCR [64, 65]. Cas13 protein targets RNAs and its cleavage activity are similar to Cas12, however, Cas13 cleaves all surrounding ssRNA instead of DNA [65, 66]. After this step, signal readouts can be performed by fluorescence or colorimetric-based systems [67, 68].
Recent advancements in detection techniques include an electrochemical aptasensor that can detect ultrasensitive COVID-19 nucleocapsid protein and the RdRp gene [69, 70]. In another study, CRISPR-Cas12a was paired with an electro chemi luminescent sensor [65, 67, 71, 72]. Some of the recent developments include methods employing a pH-induced regenerative DNA tetrahedron ECL biosensor [73]. Smartphone readouts are new convenient methods of detection, we need to take a picture of the readout and use a colour picker app, it is converted to a greyscale image and analyzed, from the colour picker app, saturation and Lightness values are extracted for analysis. This method gives a high margin of error though it is easy to use [74]. Another microfluidic chip was developed that could integrate isothermal amplification, CRISPR cleavage, and lateral flow in a closed platform [75]. Aptamers can also be used as general biosensing platforms for various analytics, CRISPR/Cas12a mediated systems for detecting diverse analytics have been developed [76]. They translate the signal of aptamer response into CRISPR mediated nucleic acid detection-based output signal [77]. However, a lack of stable amplification of the input signal is observed, and it doesn’t meet the requirements for low abundance sample detection, it also can’t be used for early diagnosis [78]. A few recent advancements in CRISPER tests are listed in Table 3.
| Name | Sample | Target gene | Cas protein | LoD (Limit of Detection) | RNA Isolation and Amplification Method | Detector/ Biosensor | Reference |
|---|---|---|---|---|---|---|---|
| OR-DETECTR | Human serum | RdRp and N gene | Cas12a | 1-2.5 copies/uL | RT-RPA | Fluorescence/ Lateral flow assay | Li S, et al. [77] |
| OR- SHERLOCK | Nasopharyngeal swab | RdRp and N gene | Cas13 | 1-5 copies/ uL | RT-RPA | Fluorescence/ Lateral flow assay | Safari F, et al. [79] |
| CASdetec | Nasopharyngeal swab | RdRp gene | Cas12b | 1x10^4 copies | RT-RAA | Fluorescence | Khan WA, et al. [78] |
| AIOD-CRISPR | - | - | Lba, Cas12a | 11 copies | RPA | Fluorescence, visual | |
| CRISPR- Cas12A-NER | - | N, Orf1a, Orf1b, E gene | LbCas12a | 10 copies | RT-RAA | Fluorescence, Naked eye | Wang R, et al. [29] |
| SHINE | - | - | Cas13a | 10cp/uL | RPA | Smartphone | Wang R, et al. [29] |
| (in-tube fluorescence readout or lateral flow strip) | |||||||
| CRISPR-FDS | Nasal swabs | ORF1a, ORF1b | Cas12a | 5 copies | RT-RPA | Fluorescent | Wang R, et al. [29] |
| CONAN | Nasopharyngeal swab | N Gene | Cas13 | 1.0x10^10 copies | RT-LAMP | Lateral flow assay | Safari F, et al. [79] |
| PGMs- CRISPER | Nasal swabs | N, M, E genes | Cas12a | 1 copy | RT-RAA | Glucose meter readout | Khan WA, et al. [78] |
| OpvCRISPER | Nasopharyngeal swabs | S gene | Cas12a | 5x10^10 copies /uL | RT-LAMP | Naked eye, Colorimetry, Fluorescence | Khan WA, et al. [78] |
| CODA | Nasopharyngeal swabs | - | Cas12a | 3 copy/uL | RT-RPA | Radiometric measurement of Fluorescence anisotropy | Khan WA, et al. [78] |
| CALIBURN | Nasopharyngeal swabs | ROF1ab | Cas12a | 5 copies per reaction | RT-RPA | Fluorescence | Khan WA, et al. [78] |
| - | - | - | - | - | LAMP, CLAP | Gold nanoparticle- based high throughput platform, TEM. | Li S, et al. [77] |
| CRISPR- Cas12a trans activity | - | SARS-COV-2 RdRp gene | - | - | - | Fozouni P, et al. [80] | |
| Ultralocalized Cas13a Assay | Nasal sample | - | LbuCas13a | 6 copies/uL | - | Fluorescent microscopy/ digital droplet readout | Heo W, et al. [56] |
| CRISPER- Cas13 with mobile phone microscopy | Nasopharyngeal swabs | N gene | Cas13a | 100,000 copies/mL | - | Fluorescence and mobile phone device | Heo W, et al. [56] |
| One-pot CRISPR | - | ORF, NP | - | - | LAMP | Lateral flow biosensors | Nguyen LT, et al. [81] |
| CRISPR-cas13 enzymology | - | O gene, N gene, RP gene | - | - | RT-LAMP | Fluorescence | Nguyen LT, et al. [81] |
| STOPCovid.v2 | Nasopharyngeal swab | - | Cas12b | 1000 copies/mL | Magnetic bead purification method, LAMP | Fluorescence, Lateral flow | Safari F, et al. [79] |
| CRISP- Enhance | - | - | LbCas12a | 10^-15 M | Not required | Lateral flow assay or fluorescence affinity chromatography | Liu M, et al. [43] |
| CRISPER-top | Nasopharyngeal swab | ORF and Np gene | Cas12a | 10 copies per reaction | One-pot assay | Lateral flow CRISPER top assay | Brihn A, et al. [82] |
| NBA | - | E and N gene | - | - | - | - | Böger B, et al. [30] |
Table 3: Different types of CRISPR-Cas technology used in detection of SARS-COV-2.
Serological Assays
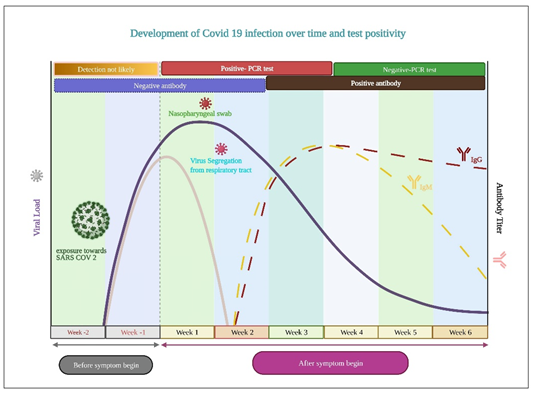
Detection of SARS-CoV-2 by molecular methods becomes undetectable with RT-PCR after 14 days of infection, they start showing false negatives due to the low count of viral RNA [83]. Adaptive immunity starts to rise approximately after one week of illness. On the 12th day, inflammatory cells build up due to pro inflammatory cytokinins and others, leading to tissue damage in the lungs [84]. Antibodies are detected with the help of serological assays to confirm previous SARS-CoV-2 infections in individuals. Antibody-based immunoassays detect antibodies (IgG and IgM) developed in response to viral infection [85]. Recombinant antigens are produced in the lab, which mimic the specific structure that binds with the antibody in the sample. Misinterpretation and false positives are possible, and sometimes cross-reactivity to other similar viruses is also observed [86]. Laboratory- based immunoassays are read by sensitive laboratory instrumentation and give quantitative results that have higher sensitivity and specificity [87]. All immunological assays show accurate and equivalent performance, and they have excellent sensitivity (around 80%) they give about 100% sensitivity after 14 days of infections [75]. Specificity varies with the type of antibody [88]. Both nucleic acid tests and serological tests are used together for effective results.
To improve the accuracy of tests, nucleic acid tests and serological tests are used in combination. The highest overall sensitivity can be obtained from the IgM-IgG combined assay compared to nuclear acid testing (NAT) and IgG and IgM independently [89]. Serological assays are not interchangeable, and individual immune monitoring may be required [90]. The complete infectious period along with positivity rate is clearly shown in Figure 9.
ELISA: Quantitative ELISA uses a two-stage procedure to test for immunoglobulin’s presence in serum which may correspond to past COVID infection. Quantitative assays against RBD protein and spike protein are done using pooled high titre serum as a reference standard. Results are compared with positive and negative controls. WHO has approved this test for detecting and quantifying SARS-CoV-2 seroprevalence and antibody profiling [91].
CLIA: Chemiluminescence immunoassay is used as a rapid POC test to detective many viral infections. The principle of CLIA is simple chemiluminescence of antigen-antibody reaction products. CLIA kits detect IgG and IgM against SARS Co-V-2 are labelled in Table 4.
Lateral Flow immunoassays are well-suited and easy-to- use point-of-care devices tests that can be performed outside the laboratory, they are also used in agricultural, veterinary, and biomedical industries and are also mentioned in Table 4. Lateral flow immunoassay developed by Mertens and colleagues at Coris Bio Concep, Belgium, targets the highly conserved nucleoprotein region of SARS-Co-V-2. It can detect the antigen in 15 minutes with an overall sensitivity of 57.6 and specificity of 99.5% [92].
Medical Imaging Techniques
Medical imaging techniques are used to confirm Covid infection and study the pulmonary damage caused by infection. The features like interstitial changes, pulmonary nodules, GGO (ground-glass opacities) are observed [93, 94]. Chest CXR detects clinical features of SARS-CoV 2 like GGO pulmonary nodules, interstitial changes, and lesions. They are easy to perform and are available in many hospitals, but they are not enough to identify low-density GGO [95].
Chest CTs are used to identify clinical features like reticular patterns, lung fibrosis, airway changes, paving patterns, GGO, etc. They have good reproducibility, high sensibility, and early imaging can help treatment. However, repeated exposure can cause irreversible effects [94, 96]. Chest ultrasound identifies B lines artefacts and pleural line irregularities. It is readily available at a low cost, but it does not examine the deep field of the lung [97].
| Company kit | Targeted molecule | Comment |
|---|---|---|
| Abbott Laboratories Inc. | IgG only | ELISA |
| DiaSorin Inc. | IgG | ELISA |
| Autobio Diagnostics Co. Ltd | IgM and IgG | ELISA |
| Ortho-clinical Diagnostics Inc. | IgG | ELISA |
| Total antibody | ||
| Mount Sinai Laboratory | IgG | ELISA |
| Chembio Diagnostic System Inc. | IgM and IgG | ELISA |
| CellaxInc | IgG and IgM | ELISA |
| Aytu Bioscience Inc | IgM and IgG | ELISA |
| Scannell Health/ Innovita | IgG and IgM | ELISA |
| SD Biosensor, Inc | IgM and IgG | ELISA |
| ZydusCadila Healthcare Ltd, India / Euroimmum US Inc. | IgG | ELISA |
| CalbiotechInc, USA | IgG | ELISA |
| Creative Diagnostics | IgG | ELISA |
| Abbott Core Laboratory | IgG | CELIA |
| Bioscience Diagnostic technology Co., Ltd | IgG antibody | Magnetic particle-based CLIA |
| SD Biosensor | - | |
| Diazyme Laboratories | IgG, IgM | Lateral Flow Immunoassay |
| Advanced Biotech | IgG IgM | |
| Aytu bioscience/ orient gene Biotech | IgG, IgM | Lateral Flow Immunoassay |
| Cellex Inc | IgG, IgM | Lateral Flow Immunoassay |
| Bio Medomics | IgG, IgM | Lateral Flow Immunoassay |
| Celer Biotechnologia | One step Covid-19 test | Lateral Flow Immunoassay |
| Mesoscale Diagnostics | IgG | V-PLEX |
Table 4: Serological kits by different companies approved by US-FDA.
Recent Advancements For Fast Detection
Electrochemical Immunosensors: Electrochemical immunosensors combined with immunoassays for robust detection, Gowan, et al. came up with a biosensing device that has filed effect transistor coated with a layer of FET graphene sheets that are specific towards antibodies [98]. Laura Fabiani et al. 2021 developed an antibody-based bioassay with magnetic beads to sustain the immunological chain. This allows the loading of a high quantity of antibodies due to an increased surface-to-volume ratio and eliminates the washing step. It takes saliva as samples. The device employed SARS-CoV-2 N and S protein as a target in the form of the sandwich test with immobilized antibodies for S or N protein on MBs, using alkaline phosphate as a secondary antibody label, it had carbon black-based SPE as sensor combined with PALM SENS moveable reader [99]. Abdulhadee Yakoh et al. 2021, developed an attractive paper-based electrochemical platform for SARS-CoV-2 diagnosis, the device has three sections that overlap each other in a zig-zag fashion with the help of double adhesive on corners. Three layers a working, a counter, and closing ePAD, have working electrode, reference electrode, and counter printed on the back of them, respectively. SARS-CoV-2 binding domain and spike protein are immobilized on the working ePAD test zone [56]. A circle is punched in the center for the test sample i.e. human serum. After placing the sample, a redox indicator ([Fe(CN)6]) is applied to enclose ePAD. Electrochemical readings are tracked using the square wave voltammetry technique were the voltammograms are displayed on a connected smartphone. This device is disposable, ready to use, and compact [100].
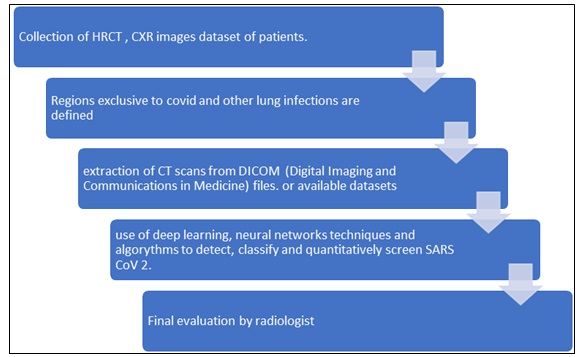
Intervention of AI: During the pandemic, many people would come to hospitals with serious health complications and severe symptoms of COVID-19, they needed immediate hospitalization. It is required to take CT images of all these patients and screen them. With a moderate number of radiologists, it was challenging to screen so many CT and CXR images. Artificial intelligence was developed to combat this situation, which could screen out SARS-CoV-2 infected lung abnormalities. Machine learning algorithms based on deep learning were developed to classify and quantify pulmonary diseases [101]. Deep learning models improve early detection, enabling isolation and treatment they relieve pressure from frontline radiologists and increase their efficiency [102]. The basic principle is to collect patients’ CT images and compare them against already available datasets (Figure 6).
Deep Learning Neural Networks Algorithms: Many computational algorithms based on deep learning were designed to detect COVID-19. We have mentioned some notable ones. Explanation of working of these models is beyond the scope of this paper. COVNet can identify COVID-19 infected lungs and differentiate them from pneumonia from their CT scans and CXR images [103]. DarkCovidNet was designed to differentiate Covid-19 vs. non-Covid-19. Few studies employ a 2D Convolutional Neural Network (CNN) to categorize figures into four categories: SARS, Influenza, non-pneumonia, and CAP [104]. Unet++ can detect viral pneumonia and differentiate it from SARS-CoV-2 [105]. DNN predicts the probability of covid-19 infection [106]. COVID-19 lesions from CT images can be drawn by DRE-Net.
All the techniques have above 90% sensitivity and specificity. They are very reliable for screening medical radiological images during the pandemic. However, larger datasets are further required to develop more robust algorithms.
Point of Care Tests
Next-generation diagnosis point of care devices and lab-on-chip devices are highly advanced, selective, easy to handle, and sensitive biosensing devices that can be used for mapping and mass testing of infections, they find a unique use for monitoring the pandemic. They are cheap, rapid, and don’t need an expert to perform tests or lab equipment. EEVD is a graphene-based hybrid electrical-electrochemical point-of-care biosensor, and it quantifies the bio-conjugation of IgG on the SARS-CoV-2-Receptor binding domain, which is immobilized onto a surface [107]. CHA-LFIA is an isothermal, non-enzymatic signal amplification system that uses catalytic hairpin assembly reaction coupled with lateral flow immunoassay. Two single-stranded are added that are complementary to each other, RNA from the sample opens the probes, yielding a stable hybrid, as the reaction proceeds, as the number of hybrids increases enabling signal amplification. The 5’ ends of H1 and H2 probes are labelled with digoxigenin and biotin, which are detected by Lateral flow immunoassay. Nasopharyngeal swabs are used for the sample, and it takes 90 minutes to complete the process [108].
Laser-scribed graphene (LSG): Laser-scribed graphene- based biosensing platforms equipped with the latest technology provide a fast and easy diagnosis of many SARS-CoV-2 variants. Researchers have come up with many modifications for these POC devices to make them for efficient detection and a user-friendly environment. LSG has gained lots of attention as an efficient POC device. Beduk T, et al. [97] developed an LSG detection system by pairing electrodes with 3D Gold nanostructures that showed faster results when compared with RT-PCR and ELISA [109].
The device is a gold-modified LSG surface with cystamine, and 1-ethyl-3-(3-diethylanimopropyl) carbodiimide along with cross-linking agents such as N-hydroxysuccinimide (EDC: NHS) is used to produce electro active groups on the surface and this was then combined with POC system along with smart phone connection. It takes blood samples and allows easy use the portable and handy devices. Beduk D, et al. [98] went one step further and coupled LSG sensors with gold nanoparticles (AuNPs) for creating a more stable, compact biosensor. They chose the ACE2 receptor as the enzymatic receptor to bind to spike protein. The entire unit was connected to a smart phone easy-to-use application. In clinical trials, the device detected Sars Cov2 variants of Alpha, Beta, and Delta variants taken from nasopharyngeal swabs under 1 minute [110]. Procleix assay: Procleix SARS- CoV-2 Assay is a fully automated transcription-mediated amplification nucleic acid test with 100% sensitivity [111]. Multiplex immunoassays can detect multiple antibodies, V-PLEX by Meso Scale Diagnostics, Canada can detect SARS- CoV-2 serostatus, and its latest algorithm can distinguish between recent infections vs. vaccine-induced humeral response. The assay requires serum samples from patients 14 days post-infection. The kit consists of 96 well plates containing spike proteins about different covid targets (Spike of alpha variant, a spike of beta variant, spike for SARS-CoV-1, nucleocapsid, and S1 receptor binding domain of virus).
The samples are diluted, and attached antibodies are marked with SULFO-TAG anti-human IgG antibodies. If the plates give output from 0-1 targets, it is considered negative, 2-3 positive targets indicate positive for infection, and report gives negative for nucleocapsid target. Then the presence of immunoglobulin is due to a vaccine or remote disease. The assay uses a (MASS 2) molecular affinity screening system, laser light of high intensity, and high-speed optical scanning with high speed to scrutinize the real-time antibodies binding to the targets. COVIDOT-TEST is a multiplex immunoblot test that can sort disputes among discordant results between computerized COVID-19 serological assays [112]. The assay allows simultaneous detection of antibodies against different antigens. It consists of enzyme immunoassay with a single barcoded strip of 14 dots (6 dots corresponding to SARS-CoV-1, OC43 MERS, NL63, HKU1, 229E, nucleocapsid, protein. Five dots are for SARS-CoV-2 nucleocapsid and two spike proteins and Receptor binding domain, one dot is blank 2 are positive and negative controls). Output is given by chemiluminescence proportional to antibody concentration. Smart gene is another fully automated POC device with equal analytical performance as RT-PCR [113].
Interpretation: Interpretation of result in RT-PCR is measured by cycle threshold (CT) value, which is defined as several repetitions essential to produce a fluorescent signal that moves across the threshold limit when it becomes detectable [114]. If the Ct value is below 40, it is positive, and above 40 is considered a negative test. If the Ct-value is less than 40 for one of the two genes, i.e., N1 and N2, it is not determined effectively and requires resetting. Low Ct- values with high viral load indicate higher transmissibility of infection [115, 116].
ELISA or CLIA does serological IgM, and IgG antibody tests are susceptible and have straight forward interpretation, they give a colour change or change in fluorescence intensity, indicating the presence or absence of antibodies corresponding to a positive result and negative result, respectively. Sometimes, combinations of two or three antibodies are performed for confirmation [117]. Rapid POC tests are being widely developed to detect antibodies. Manufacturers of these do not reveal the nature of antibodies, they directly indicate the presence and absence of antibodies by a colour change and fluorescence. However, antibodies can decline over time, so the duration of protection and persistence of these neutralizing antibodies in infected patients is yet to be studied.
Imperfect Test: Laboratory diagnosis of viral diseases is a ubiquitous part of medicine; few studies have indicated that physicians find it challenging to interpret the result correctly. A perfect test is when we have a specific biomarker for disease corresponding to either a positive or negative result. Above mentioned medical diagnostic tests are not ideal, as they have both false negatives and positives. We cannot rely on lab tests alone, clinical symptoms, prior exposure to infection, chances of getting infected, previous health complications, disease prevalence, and two or three tests in combinations or as follow-ups, all have to be considered before concluding. In all the tests, as mentioned earlier, ‘positive predictable values’ are estimated, which means that there is a high probability that the person has an infection. And ‘negative values’ are deliberated to make clear the chance that a person doesn’t have the virus. Sensitivity and specificity are the two metrics needed to interpret any diagnostic test [118]. The sensitivity of a test is defined as the facility to identify a low concentration of a given compound (viral RNA, in the case of SARS-CoV-2) in blood or saliva samples. It is inversely proportional to detectable concentration. In clinical practice, serological tests were reported with a sensitivity of 95%, and for RT-PCR, it is 80%. An assay can entirely identify the primary substance in a sample that comes under the analytical specificity. The specificity of RT- PCR and serological tests are considered to be 99% and 85%, respectively. Sensitivity may also depend on the selection of genes, and some studies suggest that E-gene primer probes give the best sensitivity [103, 104].
False Negatives
The sensitivity of the assay is dependent on viral load and the timing of sample collection from the infected individual. Several studies have questioned the sensitivity of PCR tests giving negative results in patients with all infection symptoms [119, 120]. According to a study, the possibility of false negatives is 100% on day one of infectivity, and it decreases to 68% on day 4, which is usually when symptoms start showing up. It reduces to 20% on day eight and increases to 21% on day 9 to 66% on day 21 [121]. This means testing immediately after exposure gives no result on the likelihood of infection even if the patient has visible symptoms. After one week of exposure, the rate of false-negative reduces to 21%. Sample collection technique and the virus dispersion can be some of the possible reasons for false-negative tests, these results pose a higher risk as they fail to identify the Covid-19 positive individuals who are asymptomatic. In people with symptoms, it may cause false belief that they have no infection, which might increase transmission [122]. Therefore, it should be interpreted that a negative result means “virus not detected” and does not mean “not infected with the virus.” The relation between stage of infection and false negative is vague, and transmission of the virus is also possible in those infected individuals whose test shows negative wherein samples are taken from nasopharyngeal swab [49]. Another study even suggests HRCT scan be performed for accurate diagnosis [48]. Because of lab errors, there is a chance of false negatives and infection stage during sample drawing.
Pre-test probability of the presence of disease: As discussed in the above section, the results of the test should be elucidated probabilistically to provide a likelihood that an individual does or doesn’t have an infection [46]. Only suspected ones should take the test. Pre-test probability can be estimated based on previous participation in crowd gathering, travelling history, work environment, and the overall prevalence in the city [47, 123].
Viral load is highest in the respiratory tract, followed by stool and serum samples. The severity of the disease was proportional to the viral load in respiratory samples, which is high during 14-21 days. Glucocorticoids, age, and sex affected the viral load. This can account for the high transmissibility of pandemics [124, 125, 126].
Challenges and Future Perspectives
To diagnose COVID-19, RT-PCR is considered the golden standard, but false negatives abound with this technique. In case of high clinical suspicion, alternate testing methods should be opted for confirmation. It is also crucial to reduce the number of false positives by creating clear differentiation between other infections. Another challenge is the requirement of RNA extraction platforms; though many innovative techniques have come up, they are expensive.
Serological tests have limited sensitivity early, which is also affected by a target antigen. A study showed that the S protein showed lower sensitivity levels than the N protein [127, 128]. Another challenge is to overcome cross-reactivity between the antibodies against different viruses. There are many antigenically closely related human corona viruses, increased levels of antibodies do not confirm SARS-CoV-2 infection, and it also has uncertainty in the case of delayed antibody response. Target protein responsible for immune response is not fully understood. Some argue it is S protein, some state it is N protein; this brings up ambiguity in antigen preparation. Furthermore, there are knowledge gaps about immune memory, and studies state it can be from 4 months to years [38].
CRISPR/Cas systems need professional experience for performing molecular biology techniques required, the kits are difficult to procure, and they have decreased sensitivity and specificity. Many innovative POC tests come out daily with simpler kits and lateral flow strips, making the testing process faster, more affordable, and more ready to use. But the drawback is specificity, sensitivity, and high false- negative ratio, and they still have to be basically tested and clinically approved for rapid detection. In this pandemic, accurate diagnosis is required, and lab tests need to give epidemiological information to measure the extent of the event and the rate of virus spread [80].
More knowledge should be drawn in the diagnostic field of zoonotic diseases, investigating more salient features of viruses that can help develop accurate and robust diagnostic tools. Furthermore, with the introduction of AI, the assessment of molecular and serological tests could be centralized in one place. It can be quickly implemented in other laboratories after the performance analysis. Investigations on local micro biota (in GIT and respiratory tract) should be done to assess its function against the dispersion of the virus, which may contribute to various clinical presentations and affect viral concentrations within the immune system. A consolidated list of diagnostic methods with their limitations is given in Table 5.
| S No. | Name of the test | Assay type | Accuracy | Duration of test result | Sampling Method | Limitations | References |
|---|---|---|---|---|---|---|---|
| 1 | Molecular tests | RT-PCR | 96% | 24 hrs | Nasopharyngeal Swabs. | Complex, expensive and slow to deliver | Afzal A [129] |
| 2 | Molecular tests | RT-PCR | 95% | - | Nasopharyngeal Swabs. | false-positive, expensive | Habibzadeh P, et al. [130] |
| instruments, lack of skilled personnel | |||||||
| 3 | Molecular tests | Digital PCR | 95% | 1 hr | Nasopharyngeal Swabs. | complicated work flow, expensive instruments and consumables, | Habibzadeh P, et al. [130] |
| 4 | Molecular tests | Quantitative PCR | 47% | 2-4 hrs | Nasal or Nasopharyngeal Swabs. | No Quantification, less precession | Habibzadeh P, et al. [130] |
| 5 | Nucleic Acid test | LAMP | 92.3-100% | 1-2 hrs | Blood ,urine or saliva. | Designing primer sets, and temperature. | Kilic T, et al. [131] |
| 6 | Nucleic Acid test | RT-LAMP | 92% | 2 hrs | Nasopharyngeal Swabs. | Difficulty in multiplexing | Kilic T, et al. [131] |
| 7 | Serological | ELISA | 67-98% | 3-5 hrs | Blood, plasma, or serum samples. | - | Kilic T, et al. [131] |
| 8 | Serological | Lateral Flow Assay | 95% | - | Blood or nasal samples. | Inability to the early disease | Grant BD, et al. [132] |
| 9 | Nucleic Acid test | RT-LAMP | - | < 1 hr | oropharyngeal & nasopharyngeal | limited technical infrastructure | Augustine R, et al. [28] |
| swabs and urine samples | |||||||
| 10 | Deep Learning Methods | Convolutional Net | 89.92% | - | Chest Radiographic Images | Availability of data | Nguyen TT, et al. [133] |
| 11 | Deep Learning Methods | Automated Deep Convolutional Neural Network | 98% | - | X- ray. | Less number of data sets | Salehi AW, et al. [134] |
| 12 | Nucleic Acid test | TMA | 94.70% | 5 -6 hrs | Nasopharyngeal or oral swabs. | Less detection | Kabir MDA, et al. [135] |
Table 5: Consolidated list of major diagnostic methods including their assay methods and limitations.
Conclusions
Early diagnosis plays a key role in shaping the medical action plan in a pandemic scenario, WHO opined that a diagnostic tool for viral infections need to be rapid, cheap, and accurate. RT-PCR is the predominantly used diagnosis tool in many countries; however, it needs to be repeatedly optimized to detect mutated strains. To overcome the effects of frequent mutations and low viral loads, isothermal amplification techniques have been adapted, which could quickly amplify a small amount of viral RNA to the required amount. Gene-editing tools like CRISPR/Cas systems became a new reality in diagnosis; upcoming new devices seem to be promising for more accurate diagnosis.
Various Point of care devices with amplification techniques and CRISPER/Cas systems came up based on lateral flow strips that could be operated and performed at home. Most of these innovative techniques still have to be clinically tested and approved for public use. Also, most of the tools have to overcome limitations like a separate step to prepare samples and minimize user exposure to viruses. Serological tests based on antibody detection came in handy to diagnose the previous infection in individuals and monitor immune response and diseased conditions after vaccine trial. Data integration and AI can provide excellent predictive analysis and prognosis to enable disease management and control pandemics, but AI technologies are far from immediate use.
Diagnosis domain is a promising and ever evolving scientific area that has improved drastically during the past two years. Majority of these novice interventions have been through incorporations in the various testing tools, such as molecular, radiological, and serological assays. Apart from the above tools, new age advanced methods such as bio detectors, electrochemical assays, and AI are being developed to aid these detection techniques. Need for unique advancements and testing strategies for SarSCOV-2 virus with deep learning algorithms to predict its future mutations would help in fostering a defence medical action plan that prevents future pandemics and aids in complete eradication of the infections.
Acknowledgments
This manuscript is of communication No IICT/ Pubs./2022/182.
References
-
Zhou P, Yang XL, Wang XG, Hu B, Zhang L, et al. (2020) A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 579: 270-273.
-
Wu F, Zhao S, Yu B, Chen YM, Wang W, et al. (2020) A new coronavirus associated with human respiratory disease in China. Nature 579: 265-269.
-
Khailany RA, Safdar M, Ozaslan M (2020) Genomic characterization of a novel SARS-CoV-2. Gene Reports 19: 100682.
-
Rahimi A, Mirzazadeh A, Tavakolpour S (2021) Genetics and genomics of SARS-CoV-2: A review of the literature with the special focus on genetic diversity and SARS- CoV-2 genome detection. Genomics 113(1): 1221-1232.
-
Wu A, Peng Y, Huang B, Ding X, Wang X, et al. (2020) Genome Composition and Divergence of the Novel Coronavirus (2019-nCoV) Originating in China. Cell Host Microbe 27(3): 325-328.
-
Dërmaku-Sopjani M, Sopjani M (2021) Molecular Characterization of SARS-CoV-2. Curr Mol Med 21(7): 589-595.
-
Mohamadian M, Chiti H, Shoghli A, Biglari S, Parsamanesh N, et al. (2021) COVID‐19: Virology, biology and novel laboratory diagnosis. J Gene Med 23(2): e3303.
-
Gao Y, Yan L, Huang Y, Liu F, Zhao Y, Cao L, et al. (2020) Structure of the RNA-dependent RNA polymerase from COVID-19 virus. Science 368: 779-782.
-
Shereen MA, Khan S, Kazmi A, Bashir N, Siddique R (2020) COVID-19 infection: Emergence, transmission, and characteristics of human coronaviruses. J Adv Res 24: 91-98.
-
Nyaruaba R, Mwaliko C, Hong W, Amoth P, Wei H (2021) SARS-CoV-2/COVID-19 laboratory biosafety practices and current molecular diagnostic tools. J Biosaf Biosecurity 3: 131-140.
-
Banada P, Elson D, Daivaa N, Park C, Desind S, et al. (2021) Sample collection and transport strategies to enhance yield, accessibility, and biosafety of COVID-19 RT-PCR testing. J Med Microbiol 70(9): 1380.
-
Touma M (2020) COVID-19: molecular diagnostics overview. J Mol Med 98: 947-954.
-
Zou L, Ruan F, Huang M, Liang L, Huang H, et al. (2020) SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med 382(12): 1177-1179.
-
Wölfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, et al. (2020) Virological assessment of hospitalized patients with COVID-2019. Nature 581: 465-469.
-
Spencer S, Thompson MG, Flannery B, Fry A (2019) Comparison of respiratory specimen collection methods for detection of influenza virus infection by reverse transcription-PCR: a literature review. J Clin Microbiol 57(9): e00027-e00019.
-
Wyllie AL, Fournier J, Casanovas-Massana A, Campbell M, Tokuyama M, et al. (2020) Saliva or nasopharyngeal swab specimens for detection of SARS-CoV-2. N Engl J Med 383(13): 1283-1286.
-
Caulley L, Corsten M, Eapen L, Whelan J, Angel JB, et al. (2021) Salivary detection of COVID-19. Ann Intern Med 174(1): 131-133.
-
Lui G, Ling L, Lai CKC, Tso EYK, Fung KSC, et al. (2020) Viral dynamics of SARS-CoV-2 across a spectrum of disease severity in COVID-19. J Infect 81(2): 318-356.
-
Lin W, Xie Z, Li Y, Li L, Wen C, et al. (2021) Association between detectable SARS‐COV‐2 RNA in anal swabs and disease severity in patients with coronavirus disease 2019. J Med Virol 93(2): 794-802.
-
Benzigar MR, Bhattacharjee R, Baharfar M, Liu G (2021) Current methods for diagnosis of human coronaviruses: pros and cons. Anal Bioanal Chem 413(9): 2311-2330.
-
Brooks ZC, Das S (2020) COVID-19 Testing: Impact of Prevalence, Sensitivity, and Specificity on Patient Risk and Cost. Am J Clin Pathol 154(5): 575-584.
-
Lupala CS, Ye Y, Chen H, Su X-D, Liu H (2022) Mutations on RBD of SARS-CoV-2 Omicron variant result in stronger binding to human ACE2 receptor. Biochem Biophys Res Commun 590: 34-41.
-
Kannan SR, Spratt AN, Sharma K, Chand HS, Byrareddy SN, et al. (2022) Omicron SARS-CoV-2 variant: Unique features and their impact on pre-existing antibodies. J Autoimmun 126: 102779.
-
Huang C, Wang Y, Li X, Ren L, Zhao J, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223): 497-506.
-
Udugama B, Kadhiresan P, Kozlowski HN, Malekjahani A, Osborne M, et al. (2020) Diagnosing COVID-19: the disease and tools for detection. ACS Nano 14(4): 3822- 3835.
-
Kitajima H, Tamura Y, Yoshida H, Kinoshita H, Katsuta H, et al. (2021) Clinical COVID-19 diagnostic methods: Comparison of reverse transcription loop-mediated isothermal amplification (RT-LAMP) and quantitative RT-PCR (qRT-PCR). J Clin Virol 139: 104813.
-
Ochola L, Ogongo P, Mungai S, Gitaka J, Suliman S (2022) Performance Evaluation of Lateral Flow Assays for Coronavirus Disease-19 Serology. Clin Lab Med 42: 31- 56.
-
Augustine R, Hasan A, Das S, Ahmed R, Mori Y, et al. (2020) Loop-Mediated Isothermal Amplification (LAMP): A Rapid, Sensitive, Specific, and Cost-Effective Point-of-Care Test for Coronaviruses in the Context of COVID-19 Pandemic. Biology 9(8): 182.
-
Wang R, Qian C, Pang Y, Li M, Yang Y, et al. (2021) opvCRISPR: One-pot visual RT-LAMP-CRISPR platform for SARS-cov-2 detection. Biosens Bioelectron 172: 112766.
-
Böger B, Fachi MM, Vilhena RO, Cobre AF, Tonin FS, et al. (2021) Systematic review with meta-analysis of the accuracy of diagnostic tests for COVID-19. Am J Infect Control 49(1): 21-29.
-
Yu L, Wu S, Hao X, Dong X, Mao L, et al. (2020) Rapid Detection of COVID-19 Coronavirus Using a Reverse Transcriptional Loop-Mediated Isothermal Amplification (RT-LAMP) Diagnostic Platform. Clin Chem 66(7): 975- 977.
-
Zhu X, Wang X, Han L, Chen T, Wang L, et al. (2020) Multiplex reverse transcription loop-mediated isothermal amplification combined with nanoparticle- based lateral flow biosensor for the diagnosis of COVID-19. Biosens Bioelectron 166: 112437.
-
Lamb LE, Bartolone SN, Ward E, Chancellor MB (2020) Rapid detection of novel coronavirus/Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) by reverse transcription-loop-mediated isothermal amplification. PLoS One 15(6): e0234682.
-
Luo Z, Ye C, Xiao H, Yin J, Liang Y, et al. (2022) Optimization of loop-mediated isothermal amplification (LAMP) assay for robust visualization in SARS-CoV-2 and emerging variants diagnosis. Chem Eng Sci 251: 117430.
-
Jamwal VL, Kumar N, Bhat R, Jamwal PS, Singh K, et al. (2021) Optimization and validation of RT-LAMP assay for diagnosis of SARS-CoV2 including the globally dominant Delta variant. Virol J 18(1): 178.
-
He Y, Xie T, Tong Y (2021) Rapid and highly sensitive one- tube colorimetric RT-LAMP assay for visual detection of SARS-CoV-2 RNA. Biosens Bioelectron 187: 113330.
-
John AJUK, He PJW, Katis IN, Galanis PP, Iles AH, et al. (2021) Capillary-based reverse transcriptase loop- mediated isothermal amplification for cost-effective and rapid point-of-care COVID-19 testing. Anal Chim Acta 1185: 339002.
-
Zhang Y, Chen M, Liu C, Chen J, Luo X, et al. (2021) Sensitive and rapid on-site detection of SARS-CoV-2 using a gold nanoparticle-based high-throughput platform coupled with CRISPR/Cas12-assisted RT-LAMP. Sensors Actuators B Chem 345: 130411.
-
Haq F, Sharif S, Khurshid A, Ikram A, Shabbir I, et al. (2021) Reverse transcriptase loop-mediated isothermal amplification (RT-LAMP)-based diagnosis: A potential alternative to quantitative real-time PCR based detection of the novel SARS-COV-2 virus. Saudi J Biol Sci 28(1): 942-947.
-
Inaba M, Higashimoto Y, Toyama Y, Horiguchi T, Hibino M, et al. (2021) Diagnostic accuracy of LAMP versus PCR over the course of SARS-CoV-2 infection. Int J Infect Dis 107: 195-200.
-
Ge A, Liu F, Teng X, Cui C, Wu F, et al. (2022) A Palm Germ- Radar (PaGeR) for rapid and simple COVID-19 detection by reverse transcription loop-mediated isothermal amplification (RT-LAMP). Biosensors and Bioelectronics 200: 113925.
-
Li J, Hu X, Wang X, Yang J, Zhang L, et al. (2021) A novel One-pot rapid diagnostic technology for COVID-19. Analytica Chimica Acta 1154: 338310.
-
Liu M, Li Q, Zhou J, Ai W, Zheng X, et al. (2020) Value of swab types and collection time on SARS-COV-2 detection using RT-PCR assay. J Virol Methods 286: 113974.
-
Kostyusheva A, Brezgin S, Babin Y, Vasilyeva I, Glebe D, et al. (2021) CRISPR-Cas systems for diagnosing infectious diseases. Methods 203: 431-446.
-
Pardee K, Green AA, Takahashi MK, Braff D, Lambert G, et al. (2016) Rapid, Low-Cost Detection of Zika Virus Using Programmable Biomolecular Components. Cell 165(5): 1255-1266.
-
Sun Y, Yu L, Liu C, Ye S, Chen W, et al. (2021) One-tube SARS-CoV-2 detection platform based on RT-RPA and CRISPR/Cas12a. Journal of Translational Medicine 19: 74.
-
Guo L, Sun X, Wang X, Liang C, Jiang H, et al. (2020) SARS- CoV-2 detection with CRISPR diagnostics. Cell Discovery 6: 34.
-
Sanchita B, Riedel TE, Lakhotia S, Tran ND, Ellington AD (2022) High-Surety Isothermal Amplification and Detection of SARS-CoV-2. MSphere 6: e00911-20.
-
Tang Z, Nouri R, Dong M, Yang J, Greene W, et al. (2022) Rapid detection of novel coronavirus SARS-CoV-2 by RT-LAMP coupled solid-state nanopores. Biosens Bioelectron 197: 113759.
-
Song Y, Chao Y, Guo Y, Zhang F, Mao C, et al. (2022) Paper-based netlike rolling circle amplification (NRCA) for ultrasensitive and visual detection of SARS-CoV-2. Sensors and Actuators B Chemical 358: 131460.
-
Islam MM, Koirala D (2022) Toward a next-generation diagnostic tool: A review on emerging isothermal nucleic acid amplification techniques for the detection of SARS- CoV-2 and other infectious viruses. Analytica Chimica Acta 1209: 339338.
-
Guk K, Keem JO, Hwang SG, Kim H, Kang T, et al. (2017) A facile, rapid and sensitive detection of MRSA using a CRISPR-mediated DNA FISH method, antibody-like dCas9/sgRNA complex. Biosens Bioelectron 95: 67-71.
-
Rauch JN, Valois E, Solley SC, Braig F, Lach RS, et al. (2021) A scalable, easy-to-deploy protocol for Cas13- based detection of SARS-CoV-2 genetic material. J Clin Microbiol 59(4): e02402-20.
-
Gootenberg JS, Abudayyeh OO, Lee JW, Essletzbichler P, Dy JA, et al. (2017) Nucleic acid detection with CRISPR- Cas13a/C2c2. Science 356(6336): 438-442.
-
Chen FE, Lee PW, Trick AY, Park JS, Chen L, et al. (2021) Point-of-care CRISPR-Cas-assisted SARS-CoV-2 detection in an automated and portable droplet magnetofluidic device. Biosens Bioelectron 190: 113390.
-
Heo W, Lee K, Park S, Hyun KA, Jung HI (2022) Electrochemical biosensor for nucleic acid amplification- free and sensitive detection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) RNA via CRISPR/ Cas13a trans-cleavage reaction. Biosens Bioelectron 201: 113960.
-
Ravi N, Cortade DL, Ng E, Wang SX (2020) Diagnostics for SARS-CoV-2 detection: A comprehensive review of the FDA-EUA COVID-19 testing landscape. Biosens Bioelectron 165: 112454.
-
Ali Z, Aman R, Mahas A, Rao GS, Tehseen M, et al. (2020) iSCAN: An RT-LAMP-coupled CRISPR-Cas12 module for rapid, sensitive detection of SARS-CoV-2. Virus Res 288: 198129.
-
Phan QA, Truong LB, Medina-Cruz D, Dincer C, Mostafavi E (2022) CRISPR/Cas-powered nanobiosensors for diagnostics. Biosens Bioelectron 197: 113732.
-
Nouri R, Tang Z, Dong M, Liu T, Kshirsagar A, et al. (2021) CRISPR-based detection of SARS-CoV-2: A review from sample to result. Biosensors and Bioelectronics 178: 113012.
-
Zhang K, Fan Z, Ding Y, Xie M (2022) A pH-engineering regenerative DNA tetrahedron ECL biosensor for the assay of SARS-CoV-2 RdRp gene based on CRISPR/ Cas12a trans-activity. Chem Eng J 429: 132472.
-
Chen Y, Shi Y, Chen Y, Yang Z, Wu H, et al. (2020) Contamination-free visual detection of SARS-CoV-2 with CRISPR/Cas12a: A promising method in the point-of- care detection. Biosens Bioelectron 169: 112642.
-
Nimsamer P, Mayuramart O, Rattanaburi S, Chantaravisoot N, Saengchoowong S, et al. (2021) Comparative performance of CRISPR-Cas12a assays for SARS-CoV-2 detection tested with RNA extracted from clinical specimens. J Virol Methods 290: 114092.
-
Aquino-Jarquin G (2021) Recent progress on rapid SARS-CoV-2/COVID-19 detection by CRISPR-Cas13- based platforms. Drug Discov Today 26(8): 2025-2035.
-
Han C, Li W, Li Q, Xing W, Luo H, et al. (2022) CRISPR/ Cas12a-Derived electrochemical aptasensor for ultrasensitive detection of COVID-19 nucleocapsid protein. Biosens Bioelectron 200: 113922.
-
Lin X, Liu Y, Chemparathy A, Pande T, La Russa M,et al. (2021) A comprehensive analysis and resource to use CRISPR-Cas13 for broad-spectrum targeting of RNA viruses. Cell Reports Med 2(4): 100245.
-
Zhang K, Fan Z, Huang Y, Ding Y, Xie M (2022) A strategy combining 3D-DNA Walker and CRISPR- Cas12a trans-cleavage activity applied to MXene based electrochemiluminescent sensor for SARS-CoV-2 RdRp gene detection. Talanta 236: 122868.
-
Infantino M, Pieri M, Nuccetelli M, Grossi V, Lari B, et al. (2021) The WHO International Standard for COVID-19 serological tests: towards harmonization of anti-spike assays. Int Immunopharmacol 100: 108095.
-
Sun H, Zu Y (2015) A Highlight of Recent Advances in Aptamer Technology and Its Application. Molecules 20(7): 11959-119580.
-
Krähling V, Halwe S, Rohde C, Becker D, Berghöfer S, et al. (2021) Development and characterization of an indirect ELISA to detect SARS-CoV-2 spike protein-specific antibodies. J Immunol Methods 490: 112958.
-
Mertens P, De Vos N, Martiny D, Jassoy C, Mirazimi A, et al. (2022) Development and Potential Usefulness of the COVID-19 Ag Respi-Strip Diagnostic Assay in a Pandemic Context . Frontiers in Medicine 7: 225.
-
Li Z, Ding X, Yin K, Avery L, Ballesteros E, et al.(2022) Instrument-free, CRISPR-based diagnostics of SARS- CoV-2 using self-contained microfluidic system. Biosens Bioelectron 199: 113865.
-
Xu X, Yu C, Qu J, Zhang L, Jiang S, et al. (2020) Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2. Eur J Nucl Med Mol Imaging 47(5): 1275- 1280.
-
Jacobi A, Chung M, Bernheim A, Eber C (2020) Portable chest X-ray in coronavirus disease-19 (COVID-19): A pictorial review. Clin Imaging 64: 35-42.
-
Wong HYF, Lam HYS, Fong AH-T, Leung ST, Chin TW- Y, et al. (2020) Frequency and distribution of chest radiographic findings in patients positive for COVID-19. Radiology 296(2): E72-E78.
-
Ye Z, Zhang Y, Wang Y, Huang Z, Song B (2020) Chest CT manifestations of new coronavirus disease 2019 (COVID-19): a pictorial review. Eur Radiol 30(8): 4381- 4389.
-
Li S, Huang J, Ren L, Jiang W, Wang M, et al. (2021) A one- step, one-pot CRISPR nucleic acid detection platform (CRISPR-top): Application for the diagnosis of COVID-19. Talanta 233: 122591.
-
Khan WA, Barney RE, Tsongalis GJ (2021) CRISPR-cas13 enzymology rapidly detects SARS-CoV-2 fragments in a clinical setting. J Clin Virol 145: 105019.
-
Safari F, Afarid M, Rastegari B, Borhani-Haghighi A, Barekati-Mowahed M, et al. (2021) CRISPR systems: Novel approaches for detection and combating COVID-19. Virus Res 294: 198282.
-
Fozouni P, Son S, Díaz de León Derby M, Knott GJ, Gray CN, et al. (2021) Amplification-free detection of SARS-CoV-2 with CRISPR-Cas13a and mobile phone microscopy. Cell. 184(2): 323-333.
-
Nguyen LT, Gurijala J, Rananaware SR, Pizzano BLM, Stone BT, et al. (2022) CRISPR-ENHANCE: An enhanced nucleic acid detection platform using Cas12a. Methods 203: 116-124.
-
Brihn A, Chang J, OYong K, Balter S, Terashita D, et al. (2021) Diagnostic Performance of an Antigen Test with RT-PCR for the Detection of SARS-CoV-2 in a Hospital Setting - Los Angeles County, California, June-August 2020. MMWR Morb Mortal Wkly Rep 70(19): 702-706.
-
Li Y, Xia L (2020) Coronavirus disease 2019 (COVID-19): role of chest CT in diagnosis and management. Ajr Am J Roentgenol 214: 1280-1286.
-
Saegerman C, Gilbert A, Donneau AF, Gangolf M, Diep AN, et al. (2021) Clinical decision support tool for diagnosis of COVID-19 in hospitals. PLoS One 16(3): e0247773.
-
Rashid ZZ, Othman SN, Samat MNA, Ali UK, Wong KK (2020) Diagnostic performance of COVID-19 serology assays. Malays J Pathol 42(1): 13-21.
-
Joung J, Ladha A, Saito M, Kim N-G, Woolley AE, et al. (2020) Detection of SARS-CoV-2 with SHERLOCK One- Pot Testing. N Engl J Med 383(15): 1492-1494.
-
Cheng Z, Lu Y, Cao Q, Qin L, Pan Z, et al. (2020) Clinical features and chest CT manifestations of coronavirus disease 2019 (COVID-19) in a single-center study in Shanghai, China. Am J Roentgenol 215(1): 121-126.
-
Peng Q-Y, Wang X-T, Zhang L-N, (2020) Findings of lung ultrasonography of novel corona virus pneumonia during the 2019–2020 epidemic. Intensive Care Med 46(5): 849-850.
-
Seo G, Lee G, Kim MJ, Baek S-H, Choi M, et al. (2020) Rapid Detection of COVID-19 Causative Virus (SARS-CoV-2) in Human Nasopharyngeal Swab Specimens Using Field- Effect Transistor-Based Biosensor. ACS Nano 14: 5135- 5142.
-
Fabiani L, Saroglia M, Galatà G, De Santis R, Fillo S, et al. (2021) Magnetic beads combined with carbon black- based screen-printed electrodes for COVID-19: A reliable and miniaturized electrochemical immunosensor for SARS-CoV-2 detection in saliva. Biosens Bioelectron 171: 112686.
-
Yakoh A, Pimpitak U, Rengpipat S, Hirankarn N, Chailapakul O (2021) Paper-based electrochemical biosensor for diagnosing COVID-19: Detection of SARS- CoV-2 antibodies and antigen. Biosens Bioelectron 176: 112912.
-
Chen J, Wu L, Zhang J, Zhang L, Gong D, et al. (2020) Deep learning-based model for detecting 2019 novel coronavirus pneumonia on high-resolution computed tomography. Sci Rep 10: 19196.
-
Chen N, Zhou M, Dong X, Qu J, Gong F, et al. (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395(10223): 507-513.
-
Jin C, Chen W, Cao Y, Xu Z, Tan Z, et al. (2020) Development and evaluation of an artificial intelligence system for COVID-19 diagnosis. Nat Commun 11: 5088.
-
Bai X, Wang H, Ma L, Xu Y, Gan J, et al. (2021) Advancing COVID-19 diagnosis with privacy-preserving collaboration in artificial intelligence. Nat Mach Intell 3: 1081-1089.
-
Apostolopoulos ID, Mpesiana TA (2020) Covid-19: automatic detection from X-ray images utilizing transfer learning with convolutional neural networks. Phys Eng Sci Med 43: 635-640.
-
Beduk T, Beduk D, de Oliveira Filho JI, Zihnioglu F, Cicek C, et al. (2021) Rapid Point-of-Care COVID-19 Diagnosis with a Gold-Nanoarchitecture-Assisted Laser-Scribed Graphene Biosensor. Anal Chem 93: 8585-8594.
-
Beduk D, Ilton de Oliveira Filho J, Beduk T, Harmanci D, Zihnioglu F, et al. (2022) “All in One” SARS-CoV-2 variant recognition platform: Machine learning-enabled point of care diagnostics. Biosens Bioelectron: X 10: 100105.
-
Sauleda S, Palacios L, Brès V, Piñana M, Alonso-Hernandez L, et al. (2022) Clinical evaluation of the Procleix SARS- CoV-2 assay, a sensitive, high-throughput test that runs on an automated system. Diagn Microbiol Infect Dis 102(1): 115560.
-
Li FF, Liu A, Gibbs E, Tanunliong G, Marquez AC, et al. (2022) A novel multiplex electrochemiluminescent immunoassay for detection and quantification of anti- SARS-CoV-2 IgG and anti-seasonal endemic human coronavirus IgG. J Clin Virol 146: 105050.
-
Soleimani R, Khourssaji M, Aupaix A, Rodriguez- Villalobos H, Scohy A, et al. (2021) Usefulness of a multiplex immunodot in case of discordant results between automated COVID-19 serological assays. J Virol Methods 292: 114129.
-
Kiyasu Y, Owaku M, Akashi Y, Takeuchi Y, Narahara K, et al. (2022) Clinical evaluation of the rapid nucleic acid amplification point-of-care test (Smart Gene SARS- CoV-2) in the analysis of nasopharyngeal and anterior nasal samples. J Infect Chemother 28(4): 543-547.
-
Pan Y, Zhang D, Yang P, Poon LLM, Wang Q (2020) Viral load of SARS-CoV-2 in clinical samples. Lancet Infect Dis 20(4): 411-412.
-
To KK-W, Tsang OT-Y, Leung W-S, Tam AR, Wu T-C, et al. (2020) Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. Lancet Infect Dis 20(5): 565- 574.
-
Al Bayat S, Mundodan J, Hasnain S, Sallam M, Khogali H, et al. (2021) Can the cycle threshold (Ct) value of RT- PCR test for SARS CoV2 predict infectivity among close contacts. J Infect Public Health 14(9): 1201-1205.
-
Aranha C, Patel V, Bhor V, Gogoi D (2021) Cycle threshold values in RT‐PCR to determine dynamics of SARS‐CoV‐2 viral load: An approach to reduce the isolation period for COVID‐19 patients. J Med Virol 93(12): 6794-6797.
-
Sethuraman N, Jeremiah SS, Ryo A (2020) Interpreting Diagnostic Tests for SARS-CoV-2. JAMA 323: 2249-2251.
-
Xiang F, Wang X, He X, Peng Z, Yang B, et al. (2020) Antibody Detection and Dynamic Characteristics in Patients With Coronavirus Disease 2019. Clin Infect Dis 71(8): 1930-1934.
-
Lou B, Li T-D, Zheng S-F, Su Y-Y, Li Z-Y, et al. (2020) Serology characteristics of SARS-CoV-2 infection after exposure and post-symptom onset. Eur Respir J 56(2): 2000763.
-
Caruana G, Croxatto A, Coste AT, Opota O, Lamoth F, et al. (2020) Diagnostic strategies for SARS-CoV-2 infection and interpretation of microbiological results. Clin Microbiol Infect 26: 1178-1182.
-
Torres R, Rinder HM (2020) Double-Edged Spike— Are SARS-CoV-2 Serologic Tests Safe Right Now. Lab Med 51: 236-238.
-
Yu F, Yan L, Wang N, Yang S, Wang L, et al. (2020) Quantitative Detection and Viral Load Analysis of SARS- CoV-2 in Infected Patients. Clin Infect Dis 71(15): 793- 798.
-
Poramed W, Romanee C, Chalerm L, Parichat S, Aree G, et al. (2022) Negative Nasopharyngeal and Oropharyngeal Swabs Do Not Rule Out COVID-19. J Clin Microbiol 58(5): e00297-20.
-
Wiseman J, D’Amico TA, Zawadzka S, Anyimadu H (2020) False negative SARS-CoV-2 PCR - A case report and literature review. Respir Med Case Reports 31: 101140.
-
Bos JM, Hebl VB, Oberg AL, Sun Z, Herman DS, et al. (2020) Marked Up-Regulation of ACE2 in Hearts of Patients with Obstructive Hypertrophic Cardiomyopathy: Implications for SARS-CoV-2–Mediated COVID-19. Mayo Clin Proc 95(7): 1354-1368.
-
Kucirka LM, Lauer SA, Laeyendecker O, Boon D, Lessler J (2020) Variation in false-negative rate of reverse transcriptase polymerase chain reaction–based SARS-CoV-2 tests by time since exposure. Ann Intern Med 173(4): 262-267.
-
Khan Z, Khaleel M, Mustafa M, Pavani M (2021) Interpretation of False Negative Tests for SARS-CoV-2 Infection - Challenges and solutions. Indian journal of medical microbiology, pp: S71-S71.
-
Zheng S, Fan J, Yu F, Feng B, Lou B, et al. (2020) Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January- March 2020: retrospective cohort study. BMJ 369: m1443.
-
Meyer B, Drosten C, Müller MA (2014) Serological assays for emerging coronaviruses: Challenges and pitfalls. Virus Res 194: 175-183.
-
Yi-Wei T, Schmitz JE, Persing DH, Stratton CW (2020) Laboratory Diagnosis of COVID-19: Current Issues and Challenges. J Clin Microbiol. 58(6): e00512-e00520.
-
Ju Y, Kim J, Park Y, Lee CY, Kim K, et al. (2022) Rapid and accurate clinical testing for COVID-19 by nicking and extension chain reaction system-based amplification (NESBA). Biosens Bioelectron 196: 113689.
-
Qian J, Boswell SA, Chidley C, Lu Z, Pettit ME, et al. (2020) An enhanced isothermal amplification assay for viral detection. Nat Commun 11(1): 5920.
-
Huang Z, Tian D, Liu Y, Lin Z, Lyon CJ, et al. (2020) Ultra-sensitive and high-throughput CRISPR-p owered COVID-19 diagnosis. Biosens Bioelectron 164: 112316.
-
Wang X, Zhong M, Liu Y, Ma P, Dang L, et al. (2020) Rapid and sensitive detection of COVID-19 using CRISPR/Cas12a-based detection with naked eye readout, CRISPR/Cas12a-NER. Sci Bull 65: 1436-1439.
-
Huang D, Shi Z, Qian J, Bi K, Fang M, et al. (2021) CRISPR‐Cas12a‐derived biosensor enabling portable personal glucose meter readout for quantitative detection of SARS‐CoV‐2. Biotechnol Bioeng 118(4): 1587-1596.
-
Broughton JP, Deng X, Yu G, Fasching CL, Singh J, et al. (2020) Rapid Detection of 2019 Novel Coronavirus SARS-CoV-2 Using a CRISPR-based DETECTR Lateral Flow Assay. medRxiv Prepr Serv Heal Sci.
-
Lee CY, Degani I, Cheong J, Lee J-H, Choi H-J, et al. (2021) Fluorescence polarization system for rapid COVID-19 diagnosis. Biosens Bioelectron 178: 113049.
-
Wang Y, Liu D, Lin H, Chen D, Sun J, et al. (2021) Development of a Broadly Applicable Cas12a-Linked Beam Unlocking Reaction for Sensitive and Specific Detection of Respiratory Pathogens Including SARS- CoV-2. ACS Chem Biol 16(3): 491-500.
-
Afzal A (2020) Molecular diagnostic technologies for COVID-19: Limitations and challenges. J Adv Res 26: 149-159.
-
Habibzadeh P, Mofatteh M, Silawi M, Ghavami S, Faghihi MA (2021) Molecular diagnostic assays for COVID-19: an overview. Crit Rev Clin Lab Sci 58(6): 385- 398.
-
Kilic T, Weissleder R, Lee H (2020) Molecular and Immunological Diagnostic Tests of COVID-19: Current Status and Challenges. iScience 23(8): 101406.
-
Grant BD, Anderson CE, Williford JR, Alonzo LF, Glukhova VA, et al. (2020) SARS-CoV-2 coronavirus nucleocapsid antigen-detecting half-strip lateral flow assay toward the development of point of care tests using commercially available reagents. Anal Chem 92(16): 11305-11309.
-
Nguyen TT, Nguyen QVH, Nguyen DT, Hsu EB, Yang S, et al. (2020) Artificial intelligence in the battle against coronavirus (COVID-19): a survey and future research directions. arXiv Prepr arXiv200807343.
-
Salehi AW, Baglat P, Gupta G (2020) Review on machine and deep learning models for the detection and prediction of Coronavirus. Mater Today Proc 33: 3896- 3901.
-
Kabir MDA, Ahmed R, Iqbal SMA, Chowdhury R, Paulmurugan R, et al. (2021) Diagnosis for COVID-19: current status and future prospects. Expert Rev Mol Diagn 21(3): 269-288.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda