Senile Pruritis (SP) - An Emerging Geriatric Public Health Problem (EGPHP)!
Background: Itching in any part of the body without a primary rash and in the absence of xerosis or other recognizable causes in a person over 65 years old is called Senile Pruritis. Though Pruritus is a relatively common symptom everybody experiences at any point in their life, it impacts quality of life among elderly population. Materials and Methods: This article is based on managing 2 cases and another rare case managed by the Dermatology department of a government medical college that was taken for medico-social case study for MPH scholars in the last 2 years. Relevant literature search on etiology and management practices across the globe complimented the article. Results: While the rare case taught the MPH scholars i) Idiopathic generalized pruritus is a diagnosis of exclusion, that is often difficult for primary health care providers to treat, ii) with Patients with uncontrolled idiopathic pruritus, failing to respond to standard treatment of topical applications, antihistamines and cortisone, Low-dose gabapentin can be tried. iii) An empathetic support from the family contributes to medical management. Two other cases are just a few days old, but responding to standard treatment well, need to be followed up for final long-term outcome. The standard approach consists of i) Oral antihistamines (containing Fexofenadine) ii) Chlorpromazine 25 mg at night for addressing Psychogenic component and iii) Topical application of Crotamiton 10% lotion on affected skin surface twice a day after bath.
Introduction
Senile pruritus can be defined as a chronic pruritus of unknown origin in elderly people. in persons over 65 years old. It is one of the most common conditions in the elderly accompanied by changes in temperature and textural characteristics of the skin. In the elderly, xerosis is the most common cause for an itch due to the degradation of the skin barrier over time [1]. Diabetes, Liver or kidney disease, Eczema, Psoriasis, Cholestasis, Obsessive-compulsive disorder, and Allergies are other causes. The whole-body itch might be a symptom of an underlying illness, like liver disease, kidney disease, anemia, diabetes, thyroid problems, and certain cancers [2].
Multiple studies have reported a prevalence of 11–78% pruritus in elderly patients [2]. The etiology of pruritus in elderly is not fully understood. In most elderly people, occasional pruritis is due to climate or allergens, but when it turns into long standing problem, it can induce debilitating effects, like irritation, sleep impairment, resulting in clinical depression, to the extent that they would prefer a shorter life free of symptoms than a longer life with pruritus. In fact, while an acute pruritus is the commonest cause making people rush for consultation to seek relief and chronic itch makes the sufferer avoid any social group.
Itch is clinically classified into seven types: i) Itch caused by systemic diseases, like Thyroid diseases, Polycythemia vera, Iron deficiency anemia, ii) itch caused by skin diseases, Xerosis, irritant or allergic dermatitis, Atopic dermatitis, Psoriasis, Urticaria, & Seborrheic dermatitis iii) neuropathic pruritus, Brachioradial pruritus - triggered by UV light, Brachioradialis muscle (C6 dermatome) Notalgia paranesthesia iv) Psychogenic pruritus, Somatoform disorders, dissociative disorders, schizophrenia, Hallucinations, delusional parasitosis and Adjustment disorder v) Drug-induced pruritus, with or without rashes, vi) pruritus with multiple factors, and vii) pruritis of unknown causes- without a primary rash in the absence of xerosis or other recognizable causes [3].
Pathophysiology: Various neuronal mediators, signaling mechanisms at neuronal terminals, central and peripheral neurotransmission pathways, and neuronal sensitizations processes cause itching. A variety of therapies are used, and several novel drugs are being developed to relieve itch, including systemic and topical treatments [4].
Basic Management includes symptomatic management with antihistamines and topical applications, sometime adding cortisones. Of late use of Gabapentin has resolved the issue though the mechanism is not yet clear.
This article is based on 3 different cases managed or observed being managed by the author in last 2 years.
Case Reports
Housemaid’s MIL: A house maid came late for work last Sunday 17 March 2024, begging excuses. On enquiry, she reported the reason for the delay was her mother in-law’s sleepless night. Gouramma aged about 76 years, was unable to sleep and was scratching all over the body whole night, that disturbed the entire family. She has been having this pruritis problem for over a month, itch starting in the back.
There were no eruptions or blisters. As she was sleeping most of the day on the bed, the family applied coconut oil, that gave relief for about a week, to revert soon. They tried all home remedies and followed homeopathy treatment for 8-10 days each as they costed little money and a common practice among low socio-economic families: After a detailed history taking and physical examination, she was put on oral antihistamines (Foristal Lontab 2.5 mg) in the morning and Chlorpromazine 50 mg at night, apart from local surface application of Crotorax 10% (Crotamiton 10% lotion) affected area twice a day after bathing. The lady slept well on the first night itself and within a week she is fine now, having withdrawn Chlorpromazine for the last 15 days.
Venkamma, A Longtime Bed Ridden Lady: Ms. Venkamma a widow of 82 yrs., in Sindhanur a town in Karnataka, my cousin with restricted mobility for over a year following a fracture femur (left). She is living with her younger son & daughter in law has been under lot of pressure due to her husband’s death, disturbed family life of an elder son and a psychotic elder son-in-law. She went to her elder son in Gujarat for a change about 3 months early in 2023. When she returned in Septemebr 2023 was more worried about elder son‘s family life. Since early 2024 she has become more restricted in her mobility and is under stress all the time. Started complaining of itching in the back in January 2024. They tried home remedies like applying oil, diet restriction which are traditionally associated with itching like banning {Brinjal (eggplant), sour and salty food, and promoting eating bitter leaves of Nimba (Neem), Haridra (Turmeric)}. With no relief for a fortnight, the son took her to an Ayurvedic practitioner who advised Panchakarma -a) Purgation (Virechana) through herbal medicines, emesis (Vamana) through herbal medicine, Lepa (applying medical plasters on the site of itching), bloodletting (Rakta Mokshana) which the family refused. She was administered Arogya Vardhini Vati and Manjishthadi Kwatha orally. All of them had a combined effect and itching was reduced largely after week but recurred once the treatment was stopped [10]. After the third recurrence. I was consulted on 20th March 2024. After digital inspection (over Zoom video) of the sites of itching and noticing absence of any eruptions, I advised my standard approach of i) Oral antihistamines (Allegra 180 mg contains Fexofenadine) in the morning and ii) Chlorpromazine25 mg at night and iii) Topical application of Crotorax 10% (Crotamiton 10% lotion) affected area twice a day after bathing. It’s just 3 days since following the schedule and this (31 March 24) morning’s news is a relief of all symptoms by 25%. Crotorax lotion was not available in the local market and had to be brought from Bellary, the nearest big pharma market.
A Case Generalized Chronic Idiopathic Pruritus (GCIP): A 68-year-old rural male presented to the outpatient dermatology clinic of a Government Medical College, Gadag Karnataka (GMCK), which our MPH students had taken for a socio medical case study in December 2022. This was a case with new onset, diffuse and intense pruritic symptoms that gradually progressed over a period of 2 months. The symptoms began at the lower extremities and advanced to present on the upper extremities as well. The patient had a decreased quality of life with an inability to work or sleep due to itching and the condition exacerbated by stress due to her both grown up son’s disowning him. History and physical exam revealed excoriations on both lower and upper extremities localized to the flexor surfaces. There were no specific nodules, but post-inflammatory hyperpigmentation was positive. A biopsy was not prompted due to a lack of a specific lesion. The Key outcomes after treatment with antihistamines (Allegra 120 mg BD) and, cortisones failed. They used Gabata 400 mg (Gabapentin), which resulted in Complete resolution of symptomatology within a week’s treatment.
This case taught our MPH scholars that i) Idiopathic generalized pruritus is a diagnosis of exclusion and is often difficult for providers to treat ii) with patients who present with uncontrolled idiopathic pruritus, a trial of low-dose gabapentin must be considered iii) An empathetic support from the family contributes to medical management. The mechanisms of efficacy of this treatment to promote usage need further studies.
Discussions
Identifying the underlying causes of chronic pruritus tends to be more difficult in older patients, regardless of the apparent time between the onset of symptoms and the onset of possible causes. Diagnosing Pruritus:
History Taking: “To diagnose pruritus in the elderly primary care physician must take a complete history of the itch and other medical comorbidities and the medications used to treat them. Followed by a complete skin exam, paying attention to the ‘primary’ skin lesion. If a rash is present, a skin biopsy is usually performed to help confirm the diagnosis.” One of the diagnostic challenges associated with pruritus in older adults is the difficulty of examining geriatric skin. As the skin of older patients is often “busy” due to skin changes from lifelong sun exposure and other benign skin growths. “In addition, the immune alterations of age may modify the appearance of typical skin. For example, scabies may not itch, may involve the face, and may spare the finger webs, all very atypical features for scabies in a younger patient. Laboratory and radiological evaluation may be required to exclude iron deficiency, renal disease, liver disease, diabetic neuropathy, and lymphoma as possible causes. “A careful medicine history, especially for exposure to calcium channel blockers, may identify a medication as the cause of the pruritus. Diagnosing pruritus is time consuming. The care provider must talk to the patient directly, as the representative may not give correct picture as happened to me in case of Venkamma, whose son said that itch is on the back and attributed it to long hours of sleeping supine. When checked with her directly it all over body, more see behind ears and scalp.
Physical Examination: As part of the initial diagnosis, identifying pruritic skin disease usually involves a thorough examination of a patient’s skin and detailed questions about their medical histories. It’s important to look for dry, red, rough, scaly, or bumpy skin. Additionally, it’s necessary to ask patients whether they know what inciting factor caused the pruritus and whether they’ve found anything that alleviates the itch. Lab tests (blood, thyroid, liver, and kidney function tests) may be needed to rule out other causes. “In refractory cases, radiological evaluation, and routine cancer screenings up to date (e.g., colonoscopy, mammography) may be necessary. Bullous pemphigoid is present in older adults with pruritus and nonspecific skin eruptions without blisters, so special ELISA [enzyme-linked immunoassay] testing and immunofluorescent skin biopsy testing may also be required to make this diagnosis. “The examination must also look for possible secondary causes. Organomegaly (liver, spleen), and Lymph nodes palpation, in rare cases of lymphoma with pruritus are assessed.
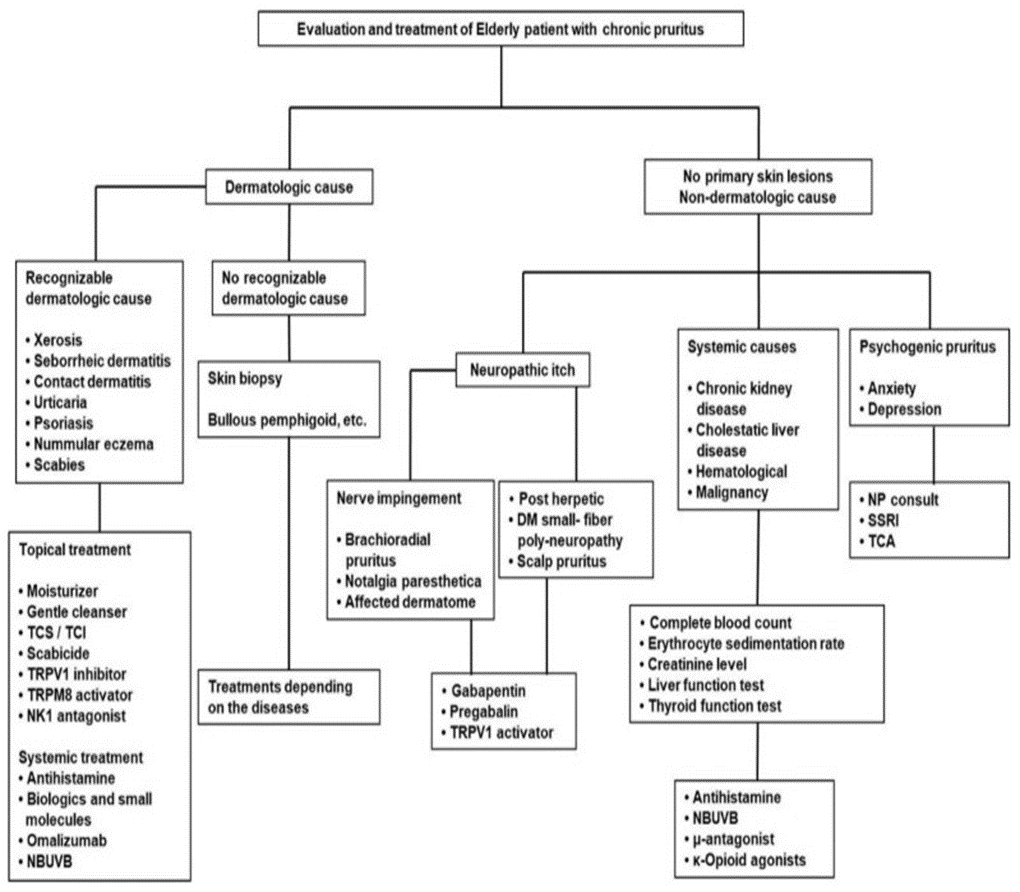
Investigations: Asking for a full blood count, renal, liver, fasting glucose and thyroid function studies is done in the first instance. A full blood count is helpful in assessing hematological disorders such as leukemias, anemia and polycythemia. Renal and liver function studies evaluate renal or hepatic dysfunction. Abnormalities in liver function could also point to infections, or drug-related, alcoholic, or inflammatory hepatitis. Given the association of itch with neoplasms, patients must get an age-appropriate cancer screening [5] (Figure 1).
Dry aging skin, xerosis, is the commonest cause of itch in elderly patients, with a prevalence ranging from 38 to 85%. Multiple skin changes the alterations in the barrier function of the stratum corneum (SC), and proteases, pH variations, and decreased activity of sebaceous and sweat glands in the elderly are related to xerosis and chronic pruritus. The SC is a barrier to prevent trans-epidermal water loss and provides protection from external factors. The SC constantly undergoes cellular turnover, and as it ages, the normal process of desquamation can be altered, leading to the appearance of dry skin [2].
Considering multiple drugs being taken that might contribute to pruritus by inducing side effects or drug associated eczematous skin lesions is the priority. A detailed patient history and laboratory tests may be required for accurate diagnosis. For chronic pruritus of inflamed or excoriated skin lesions, a skin biopsy for histological or immunofluorescence testing may be required.
An observational study, of 300 patients aged 60 years and above for geriatric dermatoses, involving 211 patients attending dermatology OPD (group A) and 89 patients were controls (Group B) from other were selected from specialties. Detailed history, thorough examination and appropriate investigations were done after obtaining informed consent. Results indicated that among 300 study subjects, 192 (64%) were, males were and 108 (36%) were females. The majority were in the 60 -70 years age group (82%). Primary ageing dermatoses were more prevalent than non-ageing dermatoses (95.3%). Pruritus was the most common complaint (164, 54.7%). Common patterns of geriatric dermatoses were wrinkling (286, 95.3%), xerosis (164,54.7%), seborrheic keratosis (94, 31.3%), Leucoplakia (48,16%), actinic keratosis (6,2.3%), infections (66, 22%), eczema (48, 16%), pigmentary disorders (38,12.7%), Papulo-squamous disorders (31, 10.3%), autoimmune blistering disorders (6,2%) and exfoliative dermatitis in 5 (1.7%). Geriatric dermatoses become more prevalent following environmental and occupational hazards as their skin is nutritionally, immunologically, and psychologically compromised. Primary ageing and pathological disorders were higher among pre-existing dermatoses group than other systemic disorders group. Early recognition of patterns and appropriate management improve the quality of life in elderly [3, 5].
A meta-analysis of 46 relevant articles, Indian recommendation for an effective diagnosis of pruritus includes a comprehensive patient history and physical examination for determining whether pruritus is due to a dermatologic disorder or an underlying systemic disease. General care measures like topical therapies with local anesthetics, pramoxine, capsaicin, calcineurin inhibitors, menthol, camphor, zinc, doxepin, corticosteroids, and palmitoyl-ethanolamine. This could be followed by basic investigations and subsequent suitable therapies. The systemic therapies, with oral antihistamines (e.g. hydroxyzine, Foristal Lontab, Allegra 24 hrs. etc.) are the first line of treatment for pruritus. The other systemic therapies include gabapentin and pregabalin, tricyclic antidepressants, doxepin, mirtazapine, naltrexone, cyclosporine and ultraviolet (UV) phototherapy [5].
While xerosis (dry skin) must be ruled out first, one- third of the geriatric population suffers from Seborrheic dermatitis (SD), which is associated with localized itch, and skin manifestation are characterized by overlying adherent, greasy scales. SD predominantly affects oily areas of the body, such as the scalp, periauricular area, nasolabial folds, cheeks, sternal area and interscapular areas and may also affect other body folds. Other dermatological conditions associated to chronic itch in the elderly are atopic dermatitis, Psoriasis, and Urticaria. Nummular eczema (NE) is an extremely pruritic, inflammatory skin disease found in elderly patients and is considered as a late-onset form of atopic dermatitis. Severe scratching or rubbing to eliminate the itch will result in skin damage, such as scratches, abrasions, erythema, lichenification, ulcers, and pigmentation of the skin. Skin diseases that induce itch mainly include eczematous dermatitis, hives, food allergies, insect bites, and scabies.
Cutaneous Immunologic Reactions: The transformation of the immune system results from the process of aging, known as immunosenescence (IS), is related to chronic pruritus. It affects both innate and adaptive immunity and induces increased autoreactivity. Bullous pemphigoid (BP), more common in the elderly, may manifest with pruritus and a nonspecific urticarial rash accompanied by circulating autoantibodies. Elderly patients suffering from chronic idiopathic pruritus produced evidence of immune dysregulation, such as lymphopenia, eosinophilia, and hypo-gammaglobulinemia. With the progression of IS, the protective effects of T helper 1 cells diminish, causing higher influence of T helper 2 cell–driven allergic reactions. This immunological imbalance increases the susceptibility of older people to chronic pruritus. In addition, Langerhans cells found in the skin of elderly tend to decrease dendrites as well as decreased numbers.
If an itching sensation occurs on the skin due to systemic diseases, then kidney disease, liver disease, gastrointestinal disease, or cancer could be the problem. Additional comprehensive laboratory tests are needed to rule out associated systemic disorders such as diabetes, renal dysfunction, and hepatic or hematologic disorders. In chronic renal failure, itch tends to become more pronounced when hemodialysis is done later than when is done earlier. Itch may also accompany various obstructive biliary diseases (primary biliary sclerosis, cirrhosis, etc.) in which bile ducts are blocked. If pruritus is less than 1 year, radiological and laboratory tests are necessary to rule out malignant disease. In patients with Hodgkin’s disease (a malignant hematological tumor), itch may appear months earlier than other systemic symptoms. Itch may also occur in association with intestinal parasites, hyper- or hypothyroidism, diabetes, and acquired immunodeficiency. In addition, medication used in patients with systemic diseases may cause allergic reactions and itch with skin rashes.
As dry skin is a common problem in Indian population and a cause for pruritus’ emollients that coat the skin with lipids can reduce the damage to skin barrier and reduce itch. Adding topical anesthetics such as pramoxine to commercial emollients to further reduce the itch. Western (USA, UK, Russia) experience document that, chronic pruritus an itch lasting more than six weeks experienced by people 65 years old and older. “It’s common, with a prevalence of 25% to 40%” [1, 6].
Scratching the itchy areas can cause the inflamed skin cells and nerve endings to release chemical mediators such as proteases that induce itch. While physical discomfort can be extremely irritating on its own, pruritus leads to the experience of sleep disruption, depression, and anxiety due to the overwhelming frustration of not being able to eradicate the itchy sensation. According to many senior dermatologists in Bengaluru “pruritic skin disease is an ever-increasing concern in the elderly population.” In many cases like our case reports the patients will have no notable skin rash. The skin conditions like dry skin, stasis dermatitis on the lower legs and above the ankles (due to venous insufficiency), age-associated immunosenescence and in diseases such as bullous pemphigoid an autoimmune blistering disease that’s more common in people older than 70 years. Senescence of the nervous system and subclinical neuropathy which occurs in diabetes can cause itch. The itch in diabetes may precede the abnormalities of blood sugar prediabetic neuropathy.
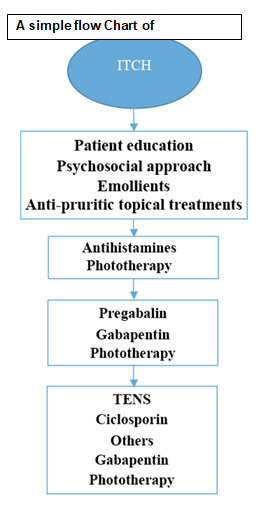
Management: There are two steps in managing pruritic skin disease, academically i) First identify and treat the underlying cause ii then treat the itching. But in Practice First treat the itching, and then make all out efforts and treat the underlying cause. Often the cause may not be identified. Therefore, in the case of xerosis, patients must be advised moisturizers are recommended for pruritic patients by applying emollients liberally. Most Indian patients have done this before coming to a health care provider. These are most effective after showering a practice most Indians reverse. Patients must be encouraged to avoid the use of drying soaps and instead use mild cleansers or Bengal gram powder. Modulating water temperature and avoiding extreme high temperatures while bathing is another simple intervention. A cold compress, ice cubes, or cooling agents containing menthol & camphor help relieve pruritus (Figure 2).
Systemic Antihistaminic or Chlorpromazine (25-50 mg based on body weight) tablets orally before going to bed, and local antipruritic lotions containing Crotamiton (Crotorax) twice a day would give relief as was our both cases response.
Sometimes first-generation antihistamines may increase the risk for falling and mental decline and, therefore, need to be monitored in this population and dose adjusted. Our experience is that these are not a big problem in Indian population especially women as they are mostly sleeping or sitting in one place hardly mobile except for going to ease themselves. Caution is needed in choosing an appropriate antipruritic cocktail for an elderly patient as most pruritus is mediated by nonhistaminergic sensory neurons. These ‘itch-specific’ nerves do not have histamine receptors, so antihistamines are generally ineffective for pruritus in the elderly.” Alternatives include gabapentin and pregabalin in doses like managing pain and neuropathies. Low-dose Sinequan (up to 6 mg), and tetrahydrocannabinol (THC, Marinol) are helpful. Ultraviolet phototherapy can be an effective treatment for pruritus in the elderly and avoids possible systemic complications. Given the limited number of treatment options, it is critical to continue to try and treat any underlying skin or systemic condition that may be contributing to the pruritus.” Of course, the treatment must be directed at the underlying cause when present.
Treating any underlying cause such as iron deficiency or renal or liver disease may be all that’s required. For the most severely pruritic patients, dry skin is usually not the cause of their pruritus. Most inflammatory dermatosis require targeted treatment, through immunosuppressives like methotrexate or mycophenolate.” “Systemic therapies include antihistamines or doxepin. Narrow-band UVB [type B ultraviolet] phototherapy may also be helpful. If an underlying systemic cause is detected, treatment is often specific to the systemic disease. Since xerosis is particularly common in elderly patients, strategies directed at treating xerosis are often fruitful as first-line attempts.” A cream with hydrocortisone, typically applied locally two times a day for two weeks. If hydrocortisone doesn’t help, trying an anti-itch cream with Pramoxine hydrochloride is also advocated [6].
Side effects of treatment of pruritus in older adults need to be constantly monitored, as they are more susceptible to the sedative effects of antihistamines, GABAergic drugs, and antidepressants certain medications, target the neural system, and may lead to confusion, therefore, be used cautiously and slowly withdrawn as soon as possible [7].
Homeopathy Management of Senile Pruritis
a) Sulphur is the first remedy they were given as the skin texture was dry, scaly, and unhealthy, burning when scratched and was sensitive to air, wind & washing. Sulphur is a potent antiseptic, helpful for scabies, and has an independent anti- psoric action. b) Arsenicum album was tried, which modifies skin symptoms like dry, scaly, shriveling that worsens in cold with internal ailments or asthma. Skin peels off in large scales. c)Rhus Toxicodendron (RT): They had also tried RT, which is useful if the skin is dry, hot, and burning, scratching is followed by burning. Rhus Toxicodendron is indicated in shingles, herpes zoster, pemphigus, and eczema [7, 8].
Ayurvedic Treatment for Senile Pruritis in India
Bakuchi or bakuchiol is valued in Ayurveda for its antipruritic (anti-itch) properties, which help relieve itching and irritation associated with eczema. Its cooling and soothing effects provide instant relief from itching, allowing for better management of eczema symptoms [4].
Alarnil with its unique triple action formula, and non- drowsy formula targets the root causes of skin irritation, inflammation, and histamine release, without fatigue as side effects. It also provides long-lasting comfort and continues to help maintain long-term skin health [10].
Prevention
• There are no proven strategies for preventing pruritus in geriatric patients. However, Patients must avoid overbathing, limit the use of harsh soaps, and use very small amounts of liquid soaps to the armpits, groin, and feet only.
• Older patients can also try to take short, lukewarm baths or showers.
• Oatmeal baths may also be soothing for dry skin.
• After showering or bathing, skin should be dried by patting instead of rubbing.
• As elderly patients have a propensity to develop allergies to cosmetic products, they should avoid or use a fragrance & preservative free moisturizer on the lower legs & sides.
• Prediabetic neuropathy can precede the development of type 2 diabetes, therefore, a good management of metabolic syndrome reduces the severity of pruritus.
• Adding Pramoxine, a topical anesthetic to emollients will further reduce the itch.
• The risk for dry and itchy skin increases with high temperatures, low humidity, and frequent hot bathing. Wearing loose, nonirritating clothing and keeping their environments cool and humidified will also benefit.
Conclusion
Itching in any part of the body without a primary rash and in the absence of xerosis or other recognizable causes in a person over 65 years old is called Senile Pruritis. Though Pruritus is a relatively common symptom everybody experiences at any point in their life, it impacts quality of life among elderly population.
Dry skin is a common problem in Indian population and a cause for pruritus, xerosis must be ruled out first. Next comes Seborrheic dermatitis (SD), which is associated with localized itch, and skin manifestation are characterized by overlying adherent, greasy scales. SD predominantly affects oily areas of the body, such as the scalp, periauricular area, nasolabial folds, cheeks, sternal area and interscapular areas and may also affect other body folds. Then comes the Psychogenic pruritus, somatoform disorders, dissociative disorders, schizophrenia, Hallucinations, delusional Parasitosis and Adjustment disorder followed by Nummular eczema (NE) is an extremely pruritic, inflammatory skin disease found in elderly patients and is considered as a late- onset form of atopic dermatitis.
Idiopathic generalized pruritus is a diagnosis of exclusion and is often difficult for primary health care providers to treat. However, they can try: i) Standard treatment with antihistamines, local application of antihistamines of Crotamiton 10% lotion on affected area twice a day after bathing. If sleep is disturbed a short-term Chlorpromazine (25 mg) be given. ii) A cream with hydrocortisone, applied locally two times a day for two weeks. If hydrocortisone also doesn’t help, an anti-itch cream with Pramoxine hydrochloride is tried. iii) with patients who present with uncontrolled idiopathic pruritus, a trial of low-dose gabapentin must be considered. iv) Empathetic support from the family contributes to medical management.
References
-
Abhirami C, Kaviarasan PK, Poorana B, Kannambal K, Prasad PVS, et al. (2023) Clinical spectrum of ageing versus non-ageing geriatric dermatoses -A case- controlled study in tertiary care center, Tamil Nadu, South India. IP Indian Journal of Clinical and Experimental Dermatology.
-
Gunalan P, Indradevi R, Oudeacoumar P, Govardhan J, Damayandhi K, et al. (2017) Pattern of skin diseases in geriatric patients attending tertiary care center. Med. Dent. Sci 6: 1566-1570.
-
Maura Keller, Treating Pruritus in Older Adults.
-
Chung BY, Um JY, Kim JC, Kang SY, Park CW, et al. (2021) Pathophysiology and Treatment of Pruritus in Elderly. Int J Mol Sci 22(1): 174.
-
Clerc C-J, Misery L (2017) A Literature Review of Senile Pruritus: From Diagnosis to Treatment. Acta Derm Venereol 97(4): 433-440.
-
Kiran Godse, Sangolli PM, Abhishek D, Sharma N, Girdhar M, et al. (2021) Management of Pruritus in Indian Settings: An Expert Opinion. American Journal of Dermatology and Venereology 10(3): 31-43.
-
Wadyka S (2022) How to Soothe Itchy Skin as You Age. Consumer Reports.
-
Homeopathy treatment for pruritus.
-
Vikas Sharma (2024) Get Rid of Itching with Natural Homeopathic Medicines.
-
Chinniah N, Monisha G (2014) Pruritus in the elderly – a guide to assessment and management. Australian Family Physician (AFP) 43(10).
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda