Examining the Effect of Drums Alive® Intervention on Verbal Communication and Task Engagement in Children with Autism Spectrum Disorder
Background: Children diagnosed with autism spectrum disorder (ASD) often encounter difficulties in verbal communication (VC) and task engagement (TE). This study aimed to investigate the impact of the Drums Alive® (DA) program, implemented as an antecedent-based intervention, on VC and TE among children with ASD. Methods: This study involved five male participants with ASD, aged four to six years. Employing an eight-week single-subject withdrawal research design (A1-B1-A2-B2), the research comprised structured activities (e.g., Legos, Jenga, hopscotch, and matching cards, etc.) in the A1 and A2 phases, each lasting 15 minutes. Subsequently, the B1 and B2 phases featured similar activities but integrated the DA intervention before the structure activities, lasting 30 minutes in total. Visual inspection was utilized to code and analyze the data. Results: During the B1 and B2 sessions, all five participants exhibited higher TE percentages compared to the A1 and A2 phases. However, no significant increase in VC percentages was observed. Conclusion: While the evidence is limited, the study suggests potential support for the effectiveness of the DA intervention in enhancing TE among children with ASD. Nevertheless, further research involving a larger sample size is imperative to validate the impact of the DA program comprehensively.
Introduction
Autism spectrum disorder (ASD) is a widely discussed neurological and developmental condition that emerges early in childhood and persists throughout life [1, 2]. Diagnosis criteria, according to the Diagnostic Statistical
Manual of Mental Disorders (DSM-5), involve deficits in social interaction and communication alongside repetitive behaviors, often leading to disruptive behavior and reduced academic concentration in learning environments [3]. These impairments can impact motor development, academic achievement, and daily life skills for children with ASD, hindering their participation in social activities. Intensive behavioral interventions are crucial for enhancing communication skills and concentration in individuals with ASD [4].
Antecedent-based intervention (ABI) is an evidence- based practice effective in addressing interfering behaviors and promoting on-task behaviors [5, 6]. ABI modifies environmental conditions to engage learners positively, enhancing social and communication skills, academic achievement, motor skills, and adaptive skills [7]. While exercise, music, drumming, and rhythmic movement have been used individually as ABIs to improve behavior in ASD, a more comprehensive approach is needed to enhance verbal communication (VC) and task engagement (TE) effectively [8].
Drums Alive® (DA) uniquely combines exercise, music, and rhythmic movement and has shown promise in enhancing attention and well-being in various populations, including individuals with attention deficits/hyperactivity disorder (ADHD) and intellectual disabilities (ID) [9, 10, 11, 12]. Previous studies, such as Yang Q, et al. [12], explored the impact of DA on attention and behavior in adolescents with ID and ASD, indicating improved attention following an eight-week DA intervention. However, research investigating the role of DA in improving VC and TE in children with ASD is scarce.
This study aimed to investigate the effect of the DA program as an ABI on VC and TE in children with ASD, exploring the potential of this unique intervention to enhance communication skills and engagement for this population.
Methods
Participants
Five participants were recruited from a North Texas autism behavioral treatment center using convenience sampling. Inclusion criteria included ages four to six, ASD diagnosis (requiring Level 1 or Level 2 support), no latex allergies, and tolerance to percussion sounds. University Institutional Review Board (IRB-FY2020-186) approval was obtained. Parents provided consent, and participants verbally/pointedly assented to Drums Alive® activities. Participants, pseudonymously named Oliver, Ethan, Dylan, Jesus, and Elijah, were categorized based on the participants’ registered behavior technicians (RBT) information and initial observations. Younger participants, Oliver and Ethan, were non-verbal, needing Level 2 support, while the older three had some verbal communication, requiring Level 1 support, working independently with occasional prompting.
Oliver, a four-and-a-half-year-old male, communicated non-verbally, understanding two to three-step instructions. Despite having an augmentative communication device, he did not utilize it throughout the two-month study. His behaviors included screaming, aggression, flopping, staring at the window, and evading tasks. During the data collection period, he liked engaging in activities such as matching cards and stacking Jenga blocks. During the DA intervention, he preferred rolling and bouncing on a ball.
Ethan, also a four-and-a-half-year-old male, initially non- verbal, started asking for “help” and would say “go” during the study. He could comprehend and follow two-step instructions but demonstrated hand tapping and frequently put his hands in his mouth, affecting his participation. His favored activities during the DA intervention were rolling and bouncing on the ball.
Dylan, a six-year-old male, had limited expressive language, answering questions with one or two-word phrases. He required reminders to stay on task and often stared at the ceiling, disrupting his activities. His preferred task involved putting letters in alphabetical order.
Jesus, another six-year-old male, had near age-appropriate expressive language but did not initiate conversations. He independently requested items and answered questions briefly. He exhibited compliant behaviors and preferred activities like throwing balls, jumping on a hopscotch course, and matching cards.
Elijah, also a six-year-old male, showed significant independence and needed minimal support. Although he had slurred speech, he could request items independently. He enjoyed activities such as dancing to Go Noddle videos, stacking wood Jenga blocks, and throwing balls and beanbags into a bucket.
Research Design
This study aimed to assess the impact of the DA program, implemented as an ABI, on VC and TE in children with ASD. A four-phase ABAB single-subject withdrawal research design was employed. The study included a non-intervention baseline phase (A1) and an intervention phase (B1), each repeated (A2 and B2). No intervention was applied during the baseline and withdrawal phases; only data on dependent variables (VC and TE) were collected. The DA intervention was introduced first in the intervention phases, followed by the same activities as in the baseline and withdrawal phases. Verification of VC and TE was done in response to the phase change. Introducing the intervention twice, comparing target behaviors with the two baseline phases, aimed to enhance and validate the functional relationship between the target behaviors and the intervention [13].
Independent Variable
In phases B1 and B2, the independent variable, the DA program intervention, preceded all data collection sessions. This intervention integrated locomotor skills (walking, jumping, jogging, and running), age-appropriate music (“What a Wonderful World”) or participant-generated percussion sounds, and rhythmic movements involving drumming, bouncing, or rolling on a 55-cm yoga ball. The principal investigator (PI) and Carrie Ekins, DA’s founder, devised the intervention protocol. Drumming activities included diverse patterns such as overhead sticks clicking, striking the ball with drumsticks (on top, side, bucket base, or ground) simultaneously with both hands, and striking the ball one-handed in an alternating pattern.
Dependent Variables
The study focused on two dependent variables: verbal communication (VC) and task engagement (TE) behaviors. Each variable had three specific conditions used for data coding. For VC, these conditions included verbally responding to questions posed by the PI or RBTs, asking for help verbally, and initiating a conversation with the PI or RBTs. TE was measured based on staying focused on assigned activities, actively working on these tasks, and utilizing assigned activity materials. All participant activities, such as Jenga, Lego, or throwing, were recorded once they commenced. VC and TE behaviors were measured using these recordings’ 10-second partial-interval direct observation. The frequency of these behaviors was then converted into percentages to illustrate changes in VC and TE.
Settings and Materials
Data collection and intervention activities occurred in a designated movement room within the autism center, adhering to COVID-19 guidelines outlined by the Centers for Disease Control and Prevention (CDC). The PI provided necessary materials for data collection (e.g., Jenga blocks, Lego, bean bags, hopscotch, writing books) and intervention (i.e., DA equipment kit). The DA equipment kit comprised three 55-cm yoga balls, three plastic baskets, three pairs of drumsticks, instructional support cards illustrating drumming patterns and locomotor skills, a Bluetooth speaker, a cell phone, and an iPad. The instructional support cards included visuals demonstrating various drumming patterns, locomotor skills like jogging and walking around the ball, and animal imitations such as mimicking an elephant with long ivories.
All intervention and data collection activities were recorded using a cellphone camera. Subsequently, the recorded videos were transferred and securely stored online in a password-protected shared file storage system after each data collection session.
Procedure
The study comprised four phases: baseline (A1), first intervention (B1), withdrawal (A2), and second intervention (B2). Each phase spanned two to three weeks, with three weekly 15-minute sessions for each participant.
During the baseline and withdrawal phases (A1 and A2), participants only participated in data collection activities. The PI instructed them to choose three activities: Legos, Jenga, throwing, matching cards, recognizing letters, hopscotch, dancing to videos, and writing or drawing. The 15-minute session was divided into three 5-minute segments, each dedicated to one chosen activity. Participants’ participation in all three activities was recorded.
The intervention phases comprised the DA intervention and subsequent data collection. Each participant underwent a 15-minute individual DA intervention, followed immediately by a 15-minute data collection session. The PI ensured adherence to CDC guidelines, arranging the environment and equipment accordingly and disinfecting between participants. The DA intervention session commenced with a warm-up involving bouncing and rolling on a ball. Following this, participants played drumming patterns, mimicking the PI’s movements. After three drumming patterns, participants were encouraged to create their drumming style. The session concluded with a cooldown, incorporating activities like stretching or walking around the ball to slow music. After the 15-minute DA intervention, participants seamlessly transitioned to the data collection activities, mirroring the baseline and withdrawal phases’ procedures.
Data collection procedures remained consistent across all phases, with activities video recorded. VC and TE were coded using a 10-second partial-interval direct observation method. The 15-minute session was divided into 90 intervals. Each interval was coded “yes” if a target behavior occurred and “no” if not. Summing the “yes” intervals (e.g., 42 out of 90 for TE) determined the behavior occurrence percentage. For example, a 15-minute video with 42 “yes” intervals out of 90 resulted in a TE percentage of 47%.
( ) " " 100% % 90 Totalintervalsbeenmarked as yes TotalTime Totalintervals intervals = × Phase transitions (e.g., from baseline to intervention) hinged on observed data patterns. In the baseline, measurements continued until a stable pattern emerged, with at least three data points consistently falling within the 0-20% range. Despite the standard of three measures for pattern stability, this study collected a minimum of five measures in each phase, ensuring a thorough assessment of stable, trending, or cyclical patterns.
Field Notes
The PI meticulously recorded observations through field notes taken during or after each session. These notes served two purposes: capturing descriptive information and reflecting on the observations. Descriptive information encompassed factual details like settings, actions, behaviors, and conversations observed and comments and feedback from RBTs. In contrast, reflective notes contained the PI’s thoughts, ideas, questions, and concerns arising during the observation.
Both field notes were crucial for accurate data documentation and analysis, aiding in a comprehensive understanding and interpretation of the observed behaviors and activities.
Inter-Observer Agreement
Inter-observer agreement (IOA) in partial interval recording involves a meticulous interval-by-interval appraisal. Each interval’s recording by data analysts, indicating the occurrence or nonoccurrence of the dependent variable, was compared. A comprehensive data recording manual was developed to detail all procedures and forms for accurate recording.
The PI trained a second data analyst. The PI and another analyst independently coded data points following the manual’s guidelines. IOA was verified when the agreement exceeded 80%. If data points fell below this threshold, the PI and the second analyst would work until an 80% agreement rate was reached. The IOA rate was calculated using the following formula:
( ) 100% % 90 Intervalsof agreement IOA Totalintervals intervals = ×
Procedural Fidelity
Following Ledford and Gast’s work on Measuring Procedural Fidelity in Behavior Research, the PI developed two procedural fidelity checklists [14]. An expert in behavioral research subsequently approved these checklists. The PI used the approved checklists to assess procedural fidelity and explained their purpose and completion process to the RBTs.
The participants’ RBTs were asked whether the PI completed each necessary step based on the fidelity checklist. The data collection procedure fidelity checklist included five items (e.g., the PI presented one activity at a time and asked the participants to change activity every five minutes). The intervention procedure fidelity checklist included five items (e.g., the PI always started the intervention with warm- up activities and ended the intervention with cool-down activities). If the agreement rate of the two checklists among five RBTs was above 80%, it could verify the intervention fidelity.
Social Validity
Besides the procedural fidelity checklists, each participant’s RBTs also completed a social validity questionnaire. This questionnaire contained five statements tailored to the DA intervention’s specifics, assessing aspects like appropriateness and effectiveness for their clients, absence of adverse effects post-participation, and participants’ enjoyment during the DA intervention. RBTs utilized a five-point Likert scale, where 1 indicated strongly disagree, and 5 represented strongly agree, to indicate their agreement with each statement.
Results
The intervention varied significantly among participants, leading to individualized explanations for each participant’s data changes. The average percentage for both VC and TE across all phases for each participant is detailed in Tables 1 and 2. Additionally, figures illustrating the precise data changes in VC and TE across phases for each participant are included.
| Participants | Baseline | Intervention 1 (DA1) | Withdrawal | Intervention 2 (DA2) |
|---|---|---|---|---|
| Oliver | 0% | 0% | 0% | 0% |
| Ethan | 0% | 13% | 2% | 4% |
| Dylan | 16% | 10% | 14% | 10% |
| Jesus | 54% | 53% | 67% | 43% |
| Elijah | 33% | 29% | 40% | 53% |
Table 1: Verbal Communication Average Percentage for Participants across Phases.
| Participants | Baseline | Intervention 1 (DA1) | Withdrawal | Intervention 2 (DA2) |
|---|---|---|---|---|
| Oliver | 59% | 78% | 71% | 81% |
| Ethan | 84% | 91% | 97% | 100% |
| Dylan | 69% | 89% | 88% | 85% |
| Jesus | 76% | 93% | 88% | 100% |
| Elijah | 96% | 94% | 92% | 96% |
Table 2: Task Engagement Average Percentage for Participants across Phases.
Oliver
Despite Oliver’s inclusion in the study, he exhibited extremely limited expressive language. Throughout the baseline phase and the entire study duration, Oliver showed no VC, as illustrated in Figure 1a.
Regarding TE behavior, in the baseline phase, Oliver’s average TE percentage was 59% (range = 38-74%). Following the first DA intervention, his TE increased significantly from
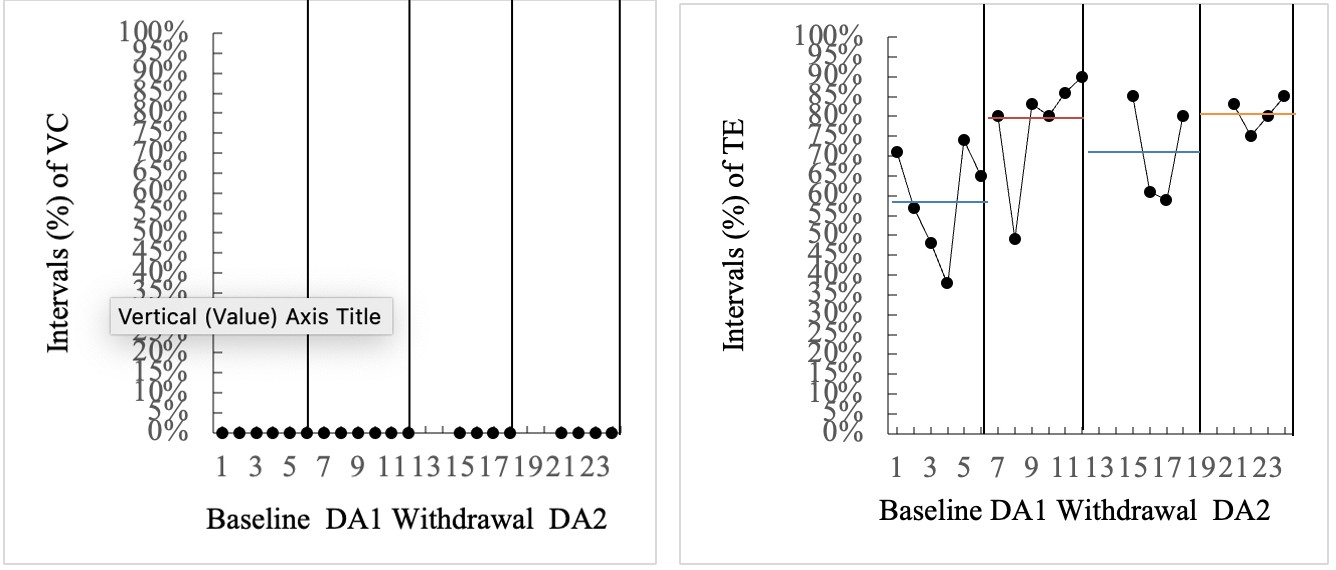
59% to 78% (range = 49-90%). Upon withdrawal of the DA intervention in the subsequent phase, Oliver’s TE decreased to 71% (range = 59-85%). However, during the second DA intervention phase, his TE level surged from 78% in the first intervention phase to 81%, displaying a narrower range of 75-85%. Notably, this phase showcased the highest TE level with the least variability compared to other phases. Interestingly, in both intervention phases, after an initial decline in the first data point, Oliver’s TE percentage steadily rose, as depicted in Figure 1b.
Figure 1a: Oliver’s VC Data. Figure 1b: Oliver’s TE Data.
Ethan
Like Oliver, Ethan did not exhibit VC during the baseline phase. However, following the introduction of the first intervention, Ethan started using single words (e.g., help, go, yes) in response to questions. His VC increased to 13% (range = 3-28%) during the first intervention phase but declined to 2% after the intervention was withdrawn (range = 0-8%).
Although his VC improved to 4% (range = 0-12%) in the second intervention phase, the frequency of his VC remained relatively low. In summary, the introduction of the DA intervention led to an increase in Ethan’s use of single-word responses for communication. However, this improvement in VC diminished to near baseline levels after the intervention was withdrawn (refer to Figure 2a).
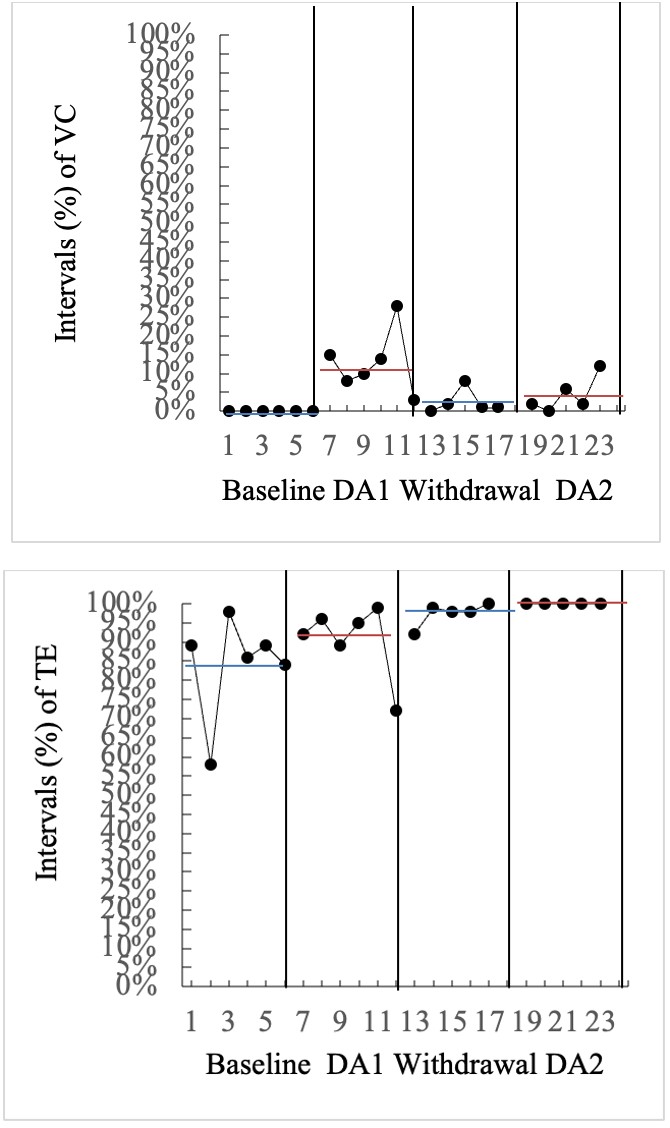
Figure 2a: Ethan’s VC Data.
Concerning TE behavior, Ethan exhibited a TE percentage of 84% during the baseline phase, with a range of 58-98%. Following the first DA intervention, his TE rose from 84% to 91% (range = 72-99%), a level sustained throughout the withdrawal and second intervention phases. The second DA intervention phase showcased the highest TE level with minimal variability compared to other phases. Ethan’s TE remained stable, except for minor fluctuations seen in the 1st and 12th data points. Despite maintaining a high TE and complying with the RBT’s requests to perform tasks, Ethan’s overall task completion accuracy remained low. In summary, Ethan’s TE increased and remained consistent after the DA intervention (refer to Figure 2b).
Figure 2b: Ethan’s TE Data.
Dylan
Dylan’s VC remained stable throughout all four phases, primarily manifesting as self-talk. When interacting with RBTs or the PI, he responded to questions using brief one or two-word phrases, such as identifying the color of a Jenga block as “yellow.” Notably, he did not initiate conversations with either RBTs or the PI. Specific to the study phases, Dylan exhibited a higher percentage of VC in the baseline (M = 16%, range = 2-34%) and withdrawal phases (M = 14%, range = 0-30%) compared to both intervention phases (M = 10%, rangeDA1 = 2-13%, rangeDA2 = 4-21%). Consequently, the DA intervention did not lead to an increase in VC for Dylan (refer to Figure 3a).
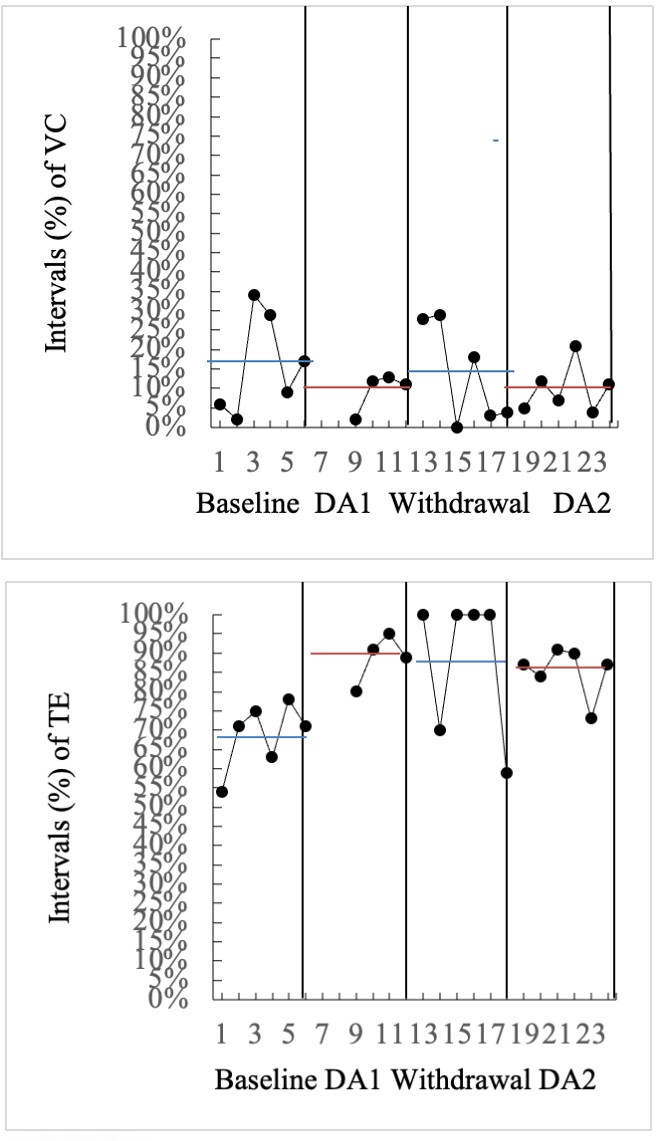
Figure 3a: Dylan’s VC Data.
In terms of TE behavior, Dylan initially exhibited a TE percentage of 69% during the baseline phase, with a range of 54-78%. Following the first DA intervention, his TE increased significantly by 20%, reaching 89% (range = 80-95%). This heightened level of TE was sustained at 88% (range = 59- 100%) throughout the withdrawal phase and only slightly decreased to 85% (range = 73-91%) after the second DA intervention. Upon visually inspecting Dylan’s data, it became apparent that there was considerable variability across all four phases. Despite some TE data points reaching 100% in the withdrawal phase, the overall TE mean was 88% (range = 59-100%), primarily due to two noticeably lower data points (i.e., the 13th and 18th data points). In summary, a thorough analysis of the data trends revealed no significant changes in TE across all phases, but there were noticeable increases following the first intervention compared to the baseline, as depicted in Figure 3b.
Figure 3b: Dylan’s TE Data.
Jesus
Jesus consistently demonstrated higher vocal communication (VC) than other participants in all phases. He provided multiple-word responses to questions from RBTs, initiated conversations, and displayed active participation. Visually analyzing his data, it was evident that his VC remained relatively stable between the baseline phase (M = 54%, range = 40-72%) and the first intervention phase (M = 53%, range = 40-61%). Surprisingly, his VC increased to 67% (range = 38-77%) during the withdrawal phase but dropped significantly to 43% (range = 31-53%) in the second intervention phase. This indicates that the DA intervention did not effectively enhance Jesus’s VC. Notably, a substantial portion of his VC consisted of repetitive echolalia speech, including self-talk, rather than meaningful interpersonal communication with RBTs or PI (see Figure 4a).
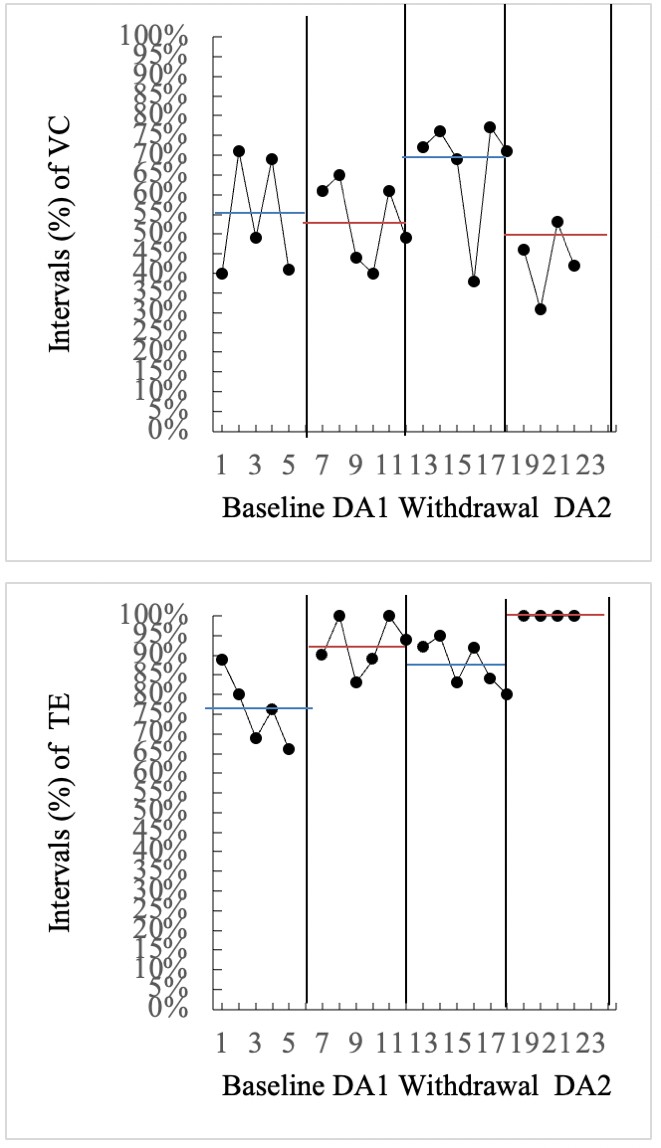
Figure 4a: Jesus’ VC data.
Examining his TE behavior, during the baseline phase, Jesus’s TE was 76% (range = 66-89%), which surged to 93% (range = 83-100%) in the first intervention phase. Following the withdrawal of the intervention, his TE dropped to 88% (range = 80-95%). Interestingly, during the second intervention phase, despite Jesus’s high physical activity levels, he consistently demonstrated 100% TE. It is worth noting that his absence for two days during this phase resulted in four data points instead of six. Figure 4b illustrates that TE percentages were approximately 15% higher in both intervention phases compared to the baseline and withdrawal phases, indicating a significant impact of the DA intervention on Jesus’s TE (see Figure 4b).
Figure 4b: Jesus’s TE Data.
Additionally, observations from intervention videos and field notes revealed Jesus’s high engagement and enjoyment of drumming activities. He frequently requested additional DA activities after sessions and, even after the withdrawal of the DA intervention, inquired about the drumming. This enthusiastic response underscores his positive engagement with the intervention despite the challenges observed in his VC patterns. Elijah Elijah consistently demonstrated a relatively high percentage of VC. Initially recorded at 33% (range = 19-51%) during the baseline phase, his VC dipped slightly to 29% (range = 21-36%) in the first intervention phase. During the withdrawal phase, there was an increase to 40% (range = 29- 52%), followed by a further rise to 53% (range = 26-72%) in the second intervention phase. The significant variability observed in Elijah’s VC data was linked to fluctuations in his social behaviors. Some days, he displayed high activity levels, asking numerous questions, while on other days, he was reserved and unresponsive to RBTs’ inquiries. Despite the notable increase in VC during the second intervention phase, it cannot be concluded that the DA intervention effectively enhanced his VC (see Figure 5a).
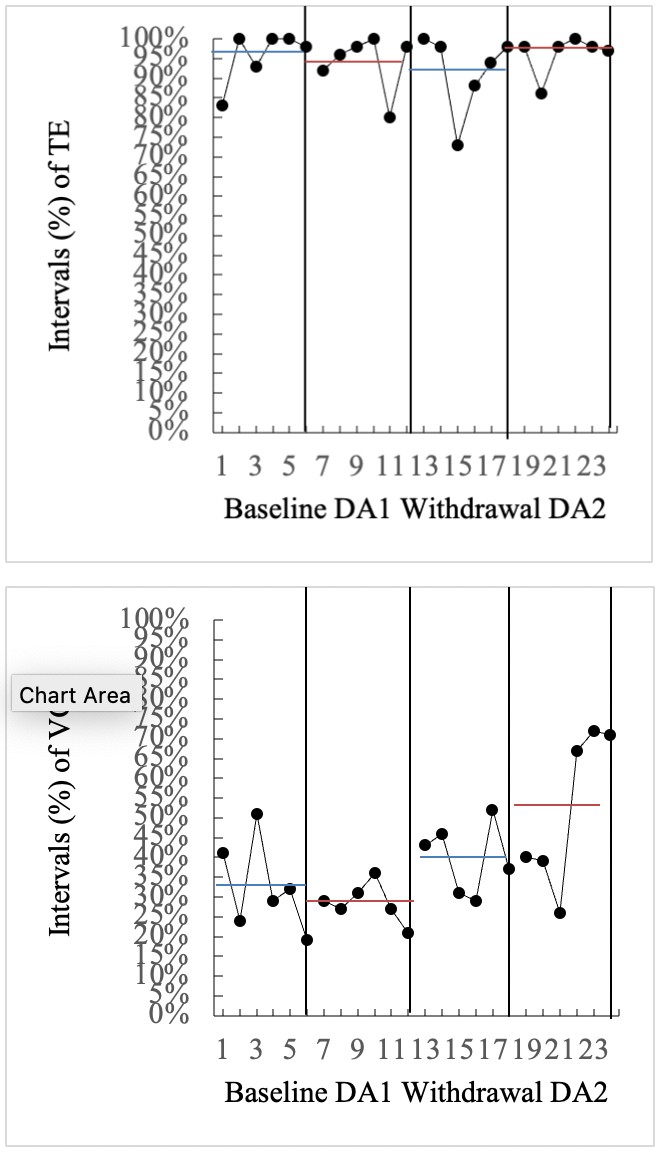
Figure 5a: Elijah’s VC Data.
Regarding TE behavior, Elijah exhibited a remarkably high percentage of TE during the baseline phase (M = 96%, range = 83-100%), maintaining this high and stable level across all four phases, averaging at 94% (range = 73-100%). Interestingly, as presented in Figure 5b, there was one data point in each phase that was very low compared with all other data points. Those data reflected the considerable changes in Elijah’s disruptive behavior that occurred once during each of the phases, which also resulted in lowering the average percentage of TE. The lack of improvement in TE for Elijah may be attributed to a ceiling effect, as his engagement was near 100% across all four phases (see Figure 5b).
Figure 5b: Elijah’s TE Data.
Amazingly, Elijah managed to complete all tasks independently and demonstrated a high level of accuracy. For instance, during the Jenga activity, he correctly stacked all the blocks and took turns with the RBT, pulling out one Jenga block at a time. However, it is also worth noting that Elijah occasionally completed tasks differently from the initial instructions provided by the RBT. For example, when asked to dance following a specific movement sequence, he danced but did not adhere to the requested sequence. Despite these deviations, his overall performance showcased his ability to participate actively and engage meaningfully.
Summary
The visual analysis of individual performance percentages revealed distinct patterns among participants. Oliver showed no variation in VC throughout the study, maintaining a consistent absence of VC or any changes in it. In contrast, his TE displayed significant improvement, starting from a low baseline. Ethan initially lacked VC but progressed to single-word responses with the introduction of the DA intervention. However, his VC decreased substantially in the withdrawal and second intervention phases, settling close to zero. Despite this, there was an overall increase in VC from the baseline. Ethan’s TE exhibited a significant boost during the first intervention phase and remained consistently high across subsequent phases. Dylan exhibited higher VC frequency compared to Oliver and Ethan, albeit at a relatively low and steady level (M = 12%; range = 10%-
16%). His TE displayed a 20% increase from baseline to the first intervention phase, sustained throughout the study. Jesus and Elijah had notably higher VC percentages (M Jesus = 54%, range Jesus = 43-67%; M Elijah = 39%, range Elijah = 29-53%) and TE percentages (M Jesus = 89%, range Jesus = 76-100%; M Elijah = 95%, range Elijah = 92-96%) than the other participants. However, they still exhibited social communication deficits, including repetitive echolalia speech and self-talk. The hypothesis predicting higher VC percentages during the intervention phases compared to the baseline and withdrawal phases was not supported by the data. There was no consistent trend observed in the VC data across all participants and phases. Nevertheless, social communication deficits were consistent across all participants, aligning with the characteristics of ASD (see Figures 1a, 2a, 3a, 4a, 5a). In terms of TE, the average percentage for all five participants increased from 77% in the baseline to 89% in the first intervention phase, maintaining 87% in the withdrawal phase and rising to 92% in the second intervention phase. Except for Elijah, who had already reached a ceiling effect, the hypothesis of increased TE during the intervention phases was confirmed. Oliver displayed a substantial increase in TE after the DA intervention, with a 20% rise during the first intervention and a subsequent 10% increase in the second intervention. Ethan’s TE improved primarily during the first intervention phase, while Elijah maintained a consistently high TE of around 95%, indicating limited room for further enhancement.
When considering group-level VC, it became evident that the DA intervention did not effectively enhance participants’ VC. The variability in VC was significant among the five participants, consistent with the anticipated limited social communication in individuals diagnosed with ASD. Conversely, group-level TE demonstrated a positive response to the DA intervention, with all participants, except Elijah, showing increased TE during the intervention phases compared to the baseline and withdrawal phases.
Inter-Observer Agreement
The inter-observer agreement (IOA) for both TE and VC) was assessed in at least 50% of sessions for each participant. These sessions were randomly distributed across the baseline, withdrawal, and two intervention phases. To calculate IOA, the number of agreed intervals was divided by the total of 90 intervals and then multiplied by 100%. The IOA between the PI and the second data analyst for VC was 86% (range = 80-89%), and for TE, it was 83% (range = 80-85%), exceeding the predetermined criteria of 80%.
Procedural Fidelity
Procedural fidelity data were collected across at least 30% of baseline, interventions, and washout sessions (i.e., 35% for baseline, 40% for intervention phases, 30% for washout) to ensure that all the necessary data collection and intervention procedures were implemented as planned. The percentage of fidelity was calculated by the number of accurately implemented steps divided by the total number of steps and multiplied by 100%. The data collection procedure average percentage fidelity was 95% (range = 90-100%) for the baseline, 94% (range = 92–100%) for both intervention phases, and 92% (range = 90–100%) for the washout phase. The intervention procedure average percentage fidelity was 94% (range = 92-98%) for the first intervention phase and 96% (range = 93-98%) for the second intervention phase. In summary, both the data collection procedure and the intervention procedure obtained a high percentage of fidelity, which means all steps were implemented as planned.
Social Validity
The collective mean score from the five RBTs was 4.8 out of 5, where a score of 1 represented “strongly disagree” and 5 represented “strongly agree.” Two RBTs consistently rated all questions with a score of 5 (M = 5, range = 5-5). Other RBTs responded positively, averaging a score of 4.5 (range = 3-5). All RBTs affirmed the appropriateness and effectiveness of the DA intervention for their clients, noting no adverse effects. They found the intervention activities easy to follow and suitable for the clients’ ages. Upon completing the data collection, they agreed that the DA intervention was cost- effective and expressed willingness to apply it with other children diagnosed with ASD post-study. The social validity of the DA intervention was unanimously endorsed by all RBTs. Moreover, three out of five participants consistently expressed enjoyment during the DA activities. Although Oliver and Ethan did not verbalize their enjoyment, their RBTs observed their excitement when informed it was time for the DA activities.
Discussion
After the DA intervention, participants showed improvements in TE but no overall improvement in VC. Individually, none demonstrated enhanced VC in both phases, except Ethan, who exhibited progress in single-word communications during the initial phase. Communication deficit is a fundamental criterion for ASD diagnosis [1]. Consequently, enhancing communication and language skills constitutes a significant long-term objective for most training programs designed for children with ASD [15, 16]. There are many reasons why we did not see differences in this variable one speculation is that the duration of our protocol was not long enough to result in changes. This speculation is particularly plausible given that it has been suggested that for therapeutic outcomes interventions should be at least twenty hours per week.
The hypothesis underlying this study posited that the DA program, functioning as a form of exercise integrating music, rhythmic movement, and drumming, with a substantial emphasis on auditory-motor integration, would enhance VC among the participating children with ASD. Auditory-motor integration plays a pivotal role in acquiring intricate social interaction and communication skills, including speech and language [17, 18]. However, despite the significant auditory- motor integration within the DA program, no improvement in VC was observed among the participants. This outcome aligns with the findings of Howells, who explored the impact of exercise on social outcomes in children with ASD and reported a non-significant effect on communication [19]. Regarding music as an intervention, previous studies have demonstrated its efficacy in improving language development [20, 21, 22]. However, music has not been proven effective in increasing the initiation or engagement in communication for individuals with ASD. Preis found that the mere presence of music in the background did not suffice to enhance spontaneous verbal expression or verbal engagement in five young participants with ASD [23]. Additionally, LaGasse reported that music therapy as a group intervention did not influence communication initiation and response to communication [24]. Finally, the observed variability in treatment responses for VC can be attributed to the inherent nature of ASD and the substantial variability within the population [25]. Consequently, it was not surprising to witness a lack of improvement in VC following a short-term intervention such as the DA intervention implemented in the current study.
In contrast to VC, the children with ASD displayed notable improvements in TE following their participation in the DA intervention. The overall mean percentages of TE for all five participants were consistently higher after the two intervention phases (MDA1 = 89%, MDA2 = 92.4%) compared to the baseline (M = 76.8%) and withdrawal (M = 87.2%) phases. Moreover, every participant, except for Elijah, exhibited individual post-intervention enhancements in TE during both DA intervention phases. The observed increase in TE in this study can be attributed to the holistic approach of the DA intervention, combining elements of PA, music, rhythmic movement, and drumming. Each of these elements is believed to stimulate the frontal lobe of the brain [26, 27, 28].
The frontal lobe, which comprises two-thirds of the human brain, plays a pivotal role in memory, motor functions, language, and attention [29, 30]. For instance, frontal lobe lesions, especially in the right hemisphere, have been linked to deficits in sustained attention, which is crucial for maintaining focus over an extended period [31]. Given the significance of the frontal lobe in attention, conditions associated with heightened frontal lobe functionality could contribute to improved TE. The prefrontal cortex, a part of the frontal lobe responsible for working memory and decision-making, is strongly associated with attention [32]. Interestingly, the key elements of DA, including PA, music, rhythmic movement, and percussion, all contribute to enhanced prefrontal cortex activity.
Children with ASD confront various challenges, with two of the most pivotal ones being VC Paris J, et al. [1] TE Ashburner J, et al. [33], Richler J, et al. [34]. These challenges are critical as they significantly impact the child’s school participation and future societal functioning as adults [35]. Since these challenges can have enduring effects throughout an individual’s life, early intervention is imperative. Research has underscored the positive and substantial effects of early interventions for children with ASD [36, 37]. While medication is a common intervention for children with ASD, most effective medications do not directly address VC and TE challenges and often entail undesirable side effects [38]. Given the importance of addressing VC and TE in children with ASD, along with the adverse effects of medications, there is an urgent need to explore innovative approaches to tackle these issues, especially within the school environment. One promising intervention is exercise, which has been demonstrated to impact both VC Howells K, et al. [19] and TE [22, 39, 40, 41, 42, 43, 44, 45, 46].
The finding of this study was the improvement in TE both as a group and on an individual basis following the DA intervention. While causality couldn’t be established due to the study’s design, it’s reasonable to speculate that each element of DA could have contributed to the changes in TE. The collective impact of these elements may have had a cumulative effect on the observed increase in TE after the DA intervention.
In summary, the study demonstrates that the DA intervention significantly improved TE in children with ASD. This holistic approach, incorporating physical activity, exercise, music, rhythmic movement, and drumming, led to notable enhancements in TE for participants. Given the challenges faced by children with ASD in areas like verbal communication and task engagement, educators and therapists are encouraged to consider implementing the DA intervention in their settings. Its positive impact on TE highlights the potential benefits of creative interventions in addressing the unique needs of children with ASD, emphasizing the importance of incorporating innovative approaches like DA into educational and therapeutic practices.
Limitations and Future Directions
The interpretation of this study’s results must account for various limitations. Influencing factors, both internal and external, such as the sample size, participant recruitment methods, environmental setting, data collection, and metrics for VC and TE, could have altered the outcomes. The single- subject ABAB intervention withdrawal design used does not eliminate the possible influences of maturation or the curriculum of the therapeutic day program attended by the study’s children. Notably, during the study, one participant, Oliver, received concurrent speech therapy, which, although separate from the DA intervention sessions, might have affected the results.
Recent trends in ASD research suggest that multi- sensory interventions can significantly influence ASD’s core characteristics [47]. Previous studies on DA programs indicate their effectiveness in enhancing motor skills, executive functions, attention, and behavioral control [37, 48, 49]. The current study’s outcomes have tangible clinical implications, demonstrating that the DA program can improve TE. The program’s simplicity, featuring movements such as bouncing, rolling, or drumming on the ball, allows participation even for those with limited motor skills. Hence, educators and clinicians should consider incorporating the DA program into professional practices.
However, this research is among a few that investigate the DA program’s impact on VC and TE in children with ASD, indicating the necessity for further studies. A deeper understanding of the DA program’s functional relationship with VC and TE will yield crucial clinical insights for employing DA as an early intervention strategy for ASD’s core characteristics.
Conclusion
In this study, TE increased among participants, though VC did not. Despite a zero-attrition rate, various elements may have influenced how the DA intervention impacted VC and TE behaviors. The study’s strengths lie in its withdrawal intervention design, which allowed participants to serve as their own controls, enhancing the reliability of the findings. Additionally, randomizing post-intervention activities helped mitigate external validity threats.
While these results should be cautiously generalized, the findings endorse the DA’s efficacy as a multisensory, antecedent-based intervention that integrates physical activity (PA), as well as musical and rhythmic movements with percussion to promote TE in children with ASD during post- intervention activities. The DA is increasingly recognized as an engaging, inventive medium beneficial for both children and adults [9, 10, 12, 48, 49, 50]. Further research into Drums Alive programs (e.g., Ability Beats, Drumtastic, Kids Beats) could significantly enhance learning environments and outcomes for those with ASD. Take out the word DrumFit. This study corroborates previous work and adds further evidence to the positive influence of DA interventions on TE in children with ASD.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Texas Woman’s University (Experiential Student Scholar Program AY 2020-2021.)
Declaration of Conflicting Interests
The authors declare that they have no competing interests.
References
-
Paris J, Phillips J (2013) Making the DSM-5 Concepts and Controversies. Springer Science + Business Media, New York, USA.
-
Hume K, Steinbrenner JR, Odom SL, Morin KL, Nowell SW, et al., (2021) Evidence-Based Practices for Children, Youth, and Young Adults with Autism: Third Generation Review. J Autism Dev Disord 51(11): 4013-4032.
-
Sterling-Turner HE, Robinson SL, Wilczynski SM (2001) Functional Assessment of Distracting and Disruptive Behaviors in the School Setting. School Psychology Review 30(2): 211-226.
-
Palmen A, Didden R, Lang R (2012) A systematic review of behavioral intervention research on adaptive skill building in high-functioning young adults with autism spectrum disorder. Research in Autism Spectrum Disorders 6(2): 602-617.
-
Neitzel J (2010) Positive Behavior Supports for Children and Youth with Autism Spectrum Disorders. Preventing School Failure: Alternative Education for Children and Youth 54(4): 247-255.
-
Wong C, Odom SL, Hume KA, Cox AW, Fettig A, et al. (2015) Evidence-Based Practices for Children, Youth, and Young Adults with Autism Spectrum Disorder: A Comprehensive Review. Journal of Autism and Developmental Disorders 45(7): 1951-1966.
-
Antecedent-based Intervention. Autism Focused Intervention Resources & Modules.
-
Warreyn P, Roeyers H (2014) See what I see, do as I do: Promoting joint attention and imitation in preschoolers with autism spectrum disorder. Autism 18(6): 658-671.
-
Ekins C, Wright J, Schulz H, Wright PR, Owens D, et al. (2019) Effects of a Drums Alive® Kids Beats Intervention on Motor Skills and Behavior in Children With Intellectual Disabilities. PALAESTRA 33(2).
-
Knappová V, Kavalířová G (2013) Drumming on Exercise Balls as The Means for Development of Coordination 7(3): 137-145.
-
Litchke LG, Bracken MM (2018) A qualitative study on the social-emotional benefits of Drumtastic Ability Beats® for children with autism spectrum disorder. American Journal of Recreation Therapy 17(3): 37-47.
-
Yang Q, Yang J, Keener E, Oh J, Gomes A, et al. (2021) Drums-Alive Intervention Effect on the Motor and Functional Skills in Youth with Intellectual Disabilities and Autism Spectrum Disorder: A Pilot Study. Advances in Physical Education 11(1): 35-46.
-
Richards S (2019) Single Subject Research.
-
Ledford JR, Gast DL (2013) Measuring procedural fidelity in behavioural research. Neuropsychological Rehabilitation 24(3-4): 332-348.
-
Lim HA (2009) Use of Music to Improve Speech Production in Children with Autism Spectrum Disorders: Theoretical Orientation. Music Therapy Perspectives 27(2): 103-114.
-
Paul R (2008) Interventions to Improve Communication in Autism. Child and Adolescent Psychiatric Clinics of North America 17(4): 835-856.
-
Tryfon A, Foster NE, Ouimet T, Doyle-Thomas K, Anagnostou E, et al. (2017) Auditory-motor rhythm synchronization in children with autism spectrum disorder. Research in Autism Spectrum Disorders 35: 51-61.
-
Zatorre RJ, Chen JL, Penhune VB (2007) When the brain plays music: auditory–motor interactions in music perception and production. Nature Reviews Neuroscience 8(7): 547-558.
-
Howells K, Sivaratnam C, May T, Lindor E, McGillivray J, et al. (2019) Efficacy of Group-Based Organised Physical Activity Participation for Social Outcomes in Children with Autism Spectrum Disorder: A Systematic Review and Meta-analysis. Journal of Autism and Developmental Disorders 49(8): 3290-3308.
-
Kaplan RS, Steele AL (2005) An Analysis of Music Therapy Program Goals and Outcomes for Clients with Diagnoses on the Autism Spectrum. Journal of Music Therapy 42(1): 2-19.
-
Lim HA (2010) Effect of ‘Developmental Speech and Language Training Through Music’ on Speech Production in Children with Autism Spectrum Disorders. Journal of Music Therapy 47(1): 2-26.
-
Wan CY, Schlaug G (2010) Neural pathways for language in autism: the potential for music-based treatments. Future neurology 5(6): 797-805.
-
Preis J, Amon R, Robinette DS, Rozegar A (2015) Does Music Matter? The Effects of Background Music on Verbal Expression and Engagement in Children with Autism Spectrum Disorders. Music Therapy Perspectives 34(1): 106-115.
-
LaGasse AB (2014) Effects of a Music Therapy Group Intervention on Enhancing Social Skills in Children with Autism. Journal of Music Therapy 51(3): 250-275.
-
Wozniak RH, Leezenbaum NB, Northrup JB, West KL, Iverson JM (2016) The development of autism spectrum disorders: variability and causal complexity. Wiley Interdisciplinary Reviews: Cognitive Science 8(1-2): e1426.
-
De Vries D, Beck T, Stacey B, Winslow K, Meines K (2015) Music as a therapeutic intervention with autism: a systematic review of the literature. Therapeutic recreation journal 49(3): 220-237.
-
Ji Z, Feng T, Mei L, Li A, Zhang C (2019) Influence of acute combined physical and cognitive exercise on cognitive function: an NIRS study. PeerJ 7: e7418.
-
Ragone G, Good J, Howland K (2021) How Technology Applied to Music-Therapy and Sound-Based Activities Addresses Motor and Social Skills in Autistic Children. Multimodal Technologies and Interaction 5(3): 11.
-
Chayer C, Freedman M (2001) Frontal Lobe Functions. Current Neurology and Neuroscience Reports 1(6): 547- 552.
-
Collins A, Koechlin E (2012) Reasoning, learning, and creativity: frontal lobe function and human decision- making. PLoS biology 10(3): e1001293.
-
Rueckert L, Grafman J (1998) Sustained attention deficits in patients with lesions of posterior cortex. Neuropsychologia 36(7): 653-660.
-
Rossi AF, Pessoa L, Desimone R, Ungerleider LG (2008) The prefrontal cortex and the executive control of attention. Experimental Brain Research 192(3): 489- 497.
-
Ashburner J, Ziviani J, Rodger S (2008) Sensory Processing and Classroom Emotional, Behavioral, and Educational Outcomes in Children With Autism Spectrum Disorder. American Journal of Occupational Therapy 62(5): 564-573.
-
Richler J, Huerta M, Bishop SL, Lord C (2010) Developmental trajectories of restricted and repetitive behaviors and interests in children with autism spectrum disorders. Development and Psychopathology 22(1): 55- 69.
-
De Vries M, Geurts H (2015) Influence of Autism Traits and Executive Functioning on Quality of Life in Children with an Autism Spectrum Disorder. Journal of Autism and Developmental Disorders 45(9): 2734-2743.
-
Corsello CM (2005) Early Intervention in Autism. Infants & Young Children 18(2): 74-85.
-
Williams KE (2018) Moving to the Beat: Using Music, Rhythm, and Movement to Enhance Self-Regulation in Early Childhood Classrooms. International Journal of Early Childhood 50(1): 85-100.
-
Baribeau DA, Anagnostou E (2014) An Update on Medication Management of Behavioral Disorders in Autism. Current Psychiatry Reports 16(3): 437.
-
Ferreira JP, Ghiarone T, Cabral Júnior CR, Furtado GE, Carvalho HM, et al. (2019) Effects of Physical Exercise on the Stereotyped Behavior of Children with Autism Spectrum Disorders. Medicina 55(10): 685.
-
Lee J, Vargo KK, Porretta DL (2018) An Evaluation of the Effects of Antecedent Exercise Type on Stereotypic Behaviors. Journal of Developmental and Physical Disabilities 30(3): 409-426.
-
Miramontez SKH, Schwartz IS (2016) The Effects of Physical Activity on the On-Task Behavior of Young Children with Autism Spectrum Disorders. International Electronic Journal of Elementary Education 9(2): 405- 418.
-
Nakutin SN, Gutierrez G, Campbell J (2019) Effect of Physical Activity on Academic Engagement and Executive Functioning in Children with ASD. School Psychology Review 48(2): 177-184.
-
Neely L, Rispoli M, Gerow S, Ninci J (2014) Effects of Antecedent Exercise on Academic Engagement and Stereotypy During Instruction. Behavior Modification 39(1): 98-116.
-
Nicholson H, Kehle TJ, Bray MA, Heest JV (2010) The effects of antecedent physical activity on the academic engagement of children with autism spectrum disorder. Psychology in the Schools 48(2): 198-213.
-
Oriel KN, George CL, Peckus R, Semon A (2011) The Effects of Aerobic Exercise on Academic Engagement in Young Children With Autism Spectrum Disorder. Pediatric Physical Therapy 23(2): 187-193.
-
Pokorski EA, Barton EE, Ledford JR, Taylor AL, Johnson E, et al. (2019) Comparison of Antecedent Activities for Increasing Engagement in a Preschool Child with ASD during a Small Group Activity. Education and Training in Autism and Developmental Disabilities 54(1): 94-103.
-
Unwin KL, Powell G, Jones CR (2021) The Use of Multi- Sensory Environments with Autistic children: Exploring the Effect of Having Control of Sensory Changes. Autism 26(6).
-
Ekins C, Wright PR, Liebich M, Wright J, Schulz H, et al. (2021) The Effects of a Drums Alive® Kids Beats Intervention on the Physical Performance and Motor Skills of Children with Developmental Delays. Open Journal of Pediatrics 11(4): 832-839.
-
Yoo GE, Kim SJ (2018) Dyadic Drum Playing and Social Skills: Implications for Rhythm-Mediated Intervention for Children with Autism Spectrum Disorder. Journal of Music Therapy 55(3): 340-375.
-
Ekins C, Owens DP (2018) Drums Alive®: A Research- Based, Multi-Disciplinary Drumming Fitness Approach to Brain and Body Health and Wellness. Palaestra 32(4): 22-28.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda