Benefits and Drawbacks of Proton-Pump Inhibitors as a Protective Agent for Aspirin Users in Long-Term Care and Geriatrics - A Systematic Review
Background: The potential benefits and drawbacks of Proton-Pump Inhibitors (PPIs) for older adults who take lower doses of aspirin over an extended period remain uncertain and poorly protected. It is crucially important to understand if PPI shall be efficient for those using aspirin from the risk of gastrointestinal bleeding (GIB) in either short or long-term care. Objective: to review and examine the benefits and drawbacks of proton-pump inhibitors (PPIs) as a protected agent in longterm care and geriatrics, particularly for low-dose aspirin users, providing practical insights for clinicians. Our findings have practical implications for clinicians, highlighting the need to consider the long-term use of PPIs to optimise patient outcomes. Care. Methods: The review adheres to PRISMA guidelines, incorporating studies investigating PPIs' efficacy and safety in elderly patients. Systematic searches were conducted using PubMed, Google Scholar, NCBI, and Cochrane Reviews for the sources associated with the merits OR benefits AND demerits of PPI AND users of aspirin dose (GI bleeding in particular). We included studies without known pre-existing cardiovascular disease, with at least 1,000 participants for RCTs, over 100 for observational studies, and a follow-up period of 12 months. Data extraction focused on study characteristics such as demographics, PPI dosage, clinical outcomes, and adverse effects. Due to the heterogeneity of study designs and outcomes, a narrative synthesis was performed to ensure a comprehensive review. Main Results: Of the 3123 studies, only 6 were included in the full review. As identified in the review, PPIs have lowered the risk of uncomplicated peptic ulcers in elderly aspirin/non-steroidal anti-inflammatory medication users. Conclusion: Proton Pump Inhibitors (PPIs) effectively prevent gastrointestinal complications in elderly patients using NSAIDs or aspirin, but their long-term use requires careful consideration to optimise patient outcomes. Balancing symptom management and risk mitigation is essential, as is following evidence-based guidelines for safe and effective therapy. Limitations of current RCTs highlight the need for further research, particularly involving non-communicating long-term care patients. Policy implications emphasise using PPIs with NSAIDs and aspirin in symptomatic elderly individuals and caution in the long-term use of high-dose PPIs.
Abbreviations
ASA: Acetylsalicylic Acid; ICH: Intracerebral Haemorrhage; COPD: Chronic Obstructive Pulmonary Disease; NSAIDs: Non-Steroidal Anti-Inflammatory Drugs; CHD: Coronary Heart Disease.
Introduction
Aspirin (Acetylsalicylic Acid; ASA) is among the most extensively utilised drugs worldwide [1], having considerable clinical proof exhibiting its antipyretic, analgesic, and anti- inflammatory characteristics. Aspirin even demonstrates antiplatelet activity by irreversibly inhibiting the manufacture of eicosanoid thromboxane A2 (TXA2), a potent stimulator of aggregating platelets [2]. This aspect causes the efficiencies of aspirin in preventing occlusive cardiovascular activities that include myocardial infection [3], transient ischaemic attack [4], and stroke [5, 6], as per the demonstration of primary and secondary prevention using randomised trials.
The benefits of low-dose aspirin are closely tied to several significant effects, with the most clinically relevant being its impact on extracranial bleeding, particularly gastrointestinal (GI) bleeding [7]. Additionally, aspirin carries an increased risk, albeit rare, of intracranial (also known as intracerebral) haemorrhage (ICH) [8]. In a study involving elderly individuals living in the community, researchers discovered the associations related to gastric cancer (GC) risk: Chronic use of omeprazole increases GC risk by 9% per year. New-onset GC cases are more common among omeprazole users. Chronic aspirin use decreases GC risk by 10% annually among omeprazole users. The lowest GC rate is observed in individuals using aspirin without omeprazole [9]. A large population-based observational study found that using low-dose aspirin for at least one year is associated with a significant 54% reduction in gastric cancer risk and a 41% reduction in oesophageal cancer risk. These findings support the protective effects of low- dose aspirin against these gastrointestinal cancers [10]. In a recent study, researchers found that low-dose aspirin use had specific effects on patients with chronic obstructive pulmonary disease (COPD) at least one year is associated with a significant 25% lower risk of lung carcinoma and a 26% decrease in lung carcinoma-related mortality [11]. In a separate study, researchers found that smoking was an independent risk factor for developing gastroduodenal mucosal breaks in individuals who were continuously using low-dose aspirin. Healthcare providers must consider these risk factors when managing low-risk aspirin patients [12]. In a retrospective cohort study involving elderly Koreans with cardiovascular risk factors, findings highlight the potential benefits of low-dose aspirin in reducing cardiovascular events and cancer risk among elderly individuals. Healthcare providers should carefully consider the benefit-risk balance when recommending aspirin therapy for primary prevention in this population [13]. Along with establishing the range of risks in bleeding related to low-dosage aspirin usage, it is essential to recognise the factors that tend to influence bleeding risk with aspirin treatment and the extent of these impacts on risk. For instance, several patients will seem to be having concomitant medicines, which have been exhibited to raise the risk level of GI bleeding provided if they are taken individually. This includes anticoagulants, non-steroidal anti- inflammatory drugs (NSAIDs), and other antiplatelet agents [14]. At the same time, the remaining patients shall have a history of peptic ulcer that is famous for increasing the upper GI bleeding (UGIB) risk in a considerable way [15].
A systematic review of RCTs and observational research in recent times analysed the risk of bleeding concerning aspirin treatment. The identification of the presence and age of Helicobacter pylori were made, and they are considered as the elements that shall raise the GI bleeding risk events in every person who takes aspirin; this review has anyhow involved just less observational research and all of those were carried out in the UK [16]. Decisions about prescribing low-dosage aspirin to this population of patients in clinical practice needs an exact and determined analysis with regards to personal bleeding risks. When an acid-suppressing agent is co-administered in patients who take prophylactic low- dosage aspirin, it has demonstrated a decreased risk of aspirin-related gastrointestinal bleeding [14, 17, 18, 19].
PPIs are the preferable agents suggested in the clinical guidelines for utilisation in patients with gastrointestinal risk factors [20, 21, 22]. The gastro-protective impacts of PPIs are restricted in terms of the upper gastrointestinal tract without security in the case of the lower gastrointestinal tract to fight against aspirin-induced bleeding. In addition, PPIs have been demonstrated to affect microbiota all over the gastrointestinal tract yet, specifically in the lesser region of the gastrointestinal tract [18], which could raise the susceptibility to gastrointestinal disorders and enteric infections [14, 23, 24, 25].
Administrating PPIs for the long term is also valuable for the prevention of Aspirin-induced gastroduodenal ulcer recurrence. It is also highly efficient compared to H2RAs, reducing recurrence to 1/10th of that observed in placebo- treated groups [26, 27, 28]. Similarly, cases administered with PPIs and NSAID reportedly reduced the recurrence rate to 1/10th of the placebo group compared to six months to one year of observation time [29]. As several patients with cardiovascular or cerebrovascular illnesses have been treated with anti-thrombotic drugs like aspirin, preventing aspirin- induced ulcers is very significant in preventing NSAID- induced ulcers. Additionally, some researchers asserted the demerits of PPIs, including Possible Allergic Reactions to Drug Chemicals [30], Dementia [31], Collagenous Colitis [32], and more. Little clinical research has demonstrated the contribution of PPIs towards injury in a tiny bowel among the users of low-dosage aspirin [33, 34]. Still, it seems imprecise if this transforms into a greater risk of lower gastrointestinal bleeding (LGIB) since the observations from the restricted observational data have blended with this topic [14, 35]. Because endoscopic procedures are not routinely performed, the origin of the bleeding is frequently unknown, and patients are treated conservatively with high-dose PPIs [36]. However, few studies state the adverse effects of long-term PPI use, including the risk of Clostridium difficile infection, dementia, pneumonia, antiplatelet agents and kidney disease [ 37-42 ]. Significantly, Hypomagnesemia occurs in up to 65% of critically sick patients, according to some research, and may raise the risk of Short long-term problems [43, 44].
Some studies stated the economic burden of GIT bleeding related to aspirin use. For example, in males with a higher risk of Coronary Heart Disease (CHD), Aspirin was cost-effective for primary prevention; however, the study employed crude assessments of GI bleeding [45]. Similarly, Saini SD, et al. [46] concluded that adding generic, low-cost omeprazole to the treatment regimen of individuals 65 and older on aspirin for secondary prevention could be cost-effective. According to the study by Earnshaw SR, et al. [47], in men older than 45 years with more significant than 10-year, 10% CHD risks, Aspirin medication is less expensive and more effective than no treatment. Adding a PPI is not cost-effective for men who have an average risk of GI bleeding, but it may be for confident men who have a higher risk of GI bleeding. According to rigorous modelling, aspirin was determined to be cost-saving or cost-effective for males with intermediate and higher CHD risk levels [48].
The prevalence of PPI use, particularly among elderly patients on aspirin therapy, underscores the critical need for a comprehensive understanding of their benefits and potential risks. This review is specifically designed to meet this need, thoroughly analysing the benefits and drawbacks of PPIs in long-term care and geriatrics and offering practical considerations for clinicians.
Methods
This systematic review pursued the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. PRISMA is an evidence-based minimum for reporting in systematic reviews and meta-analyses [49].
Criteria Used to Consider Reviews for Inclusion
The eligibility of the trials was ensured if they met the following criteria:
- Were a randomised clinical trial (RCT) or observational study that discussed the advantages and drawbacks of PPIs;
- Enrolled participants without known pre-existing cardiovascular disease.
- Registered geriatrics participants and long-term care individuals without a history of gastrointestinal bleeding (GIB) or with a follow-up of at least 12 months; aspirin doses alone had a follow-up of at least 12 months.
- Enrolled over 1,000 participants for RCTs and over 100 for observational studies.
- Focused on human subjects and was published in the English language. Non-primary articles published only as abstracts, reviews, commentaries, or letters were excluded.
- Provided information on any of the prespecified primary and secondary cardiovascular outcomes and primary and secondary bleeding outcomes.
In the first stage, the titles and abstracts of all retrieved articles were screened to determine if the studies met the inclusion criteria. The full text of potentially relevant studies was retrieved and reviewed in the second stage using the same selection and disagreement resolution methods as in the first stage. The following information was independently extracted from the included studies and jointly verified for accuracy: first author’s surname, year of publication, country of study, study design, number of participants, duration of drug exposure, relevant outcomes, outcome definitions, and characteristics of participants.
Search Methods for the Identification of Reviews
The reference lists of the included studies identified in the search were thoroughly screened to identify additional research. After eliminating duplicates, the abstracts and titles of the results were screened to ensure clarity and relevance. The authors independently analysed the full texts of the remaining results for inclusion based on predetermined criteria. The final list of included studies was determined through discussion.
Systematic searches of PubMed, Google Scholar, NCBI, and Cochrane Reviews were conducted for sources related to the merits, benefits and demerits of PPIs and aspirin users, particularly focusing on gastrointestinal bleeding.
Data Extraction and Management
Data extraction was focused on capturing key study characteristics, including population demographics, PPI dosage and duration, clinical outcomes, and reported adverse effects. We conducted a quality assessment using established criteria to evaluate the study design, methodology, and risk of bias. The authors independently extracted data using piloted forms to ensure consistency and accuracy. Data were transcribed into a structured database, capturing essential attributes such as Baseline Participant Characteristics, Age, gender, and relevant health conditions of study participants. Research Drug and Control Treatment: Details of the PPI and any control treatments used in the studies. Inclusion Criteria: Specific criteria for participant selection in each study. Endpoint Data: Primary and secondary outcomes measured in the studies. Follow-up Duration: The length of time participants were monitored in each study.
Data extraction focused on study characteristics, including population demographics, PPI dosage and duration, clinical outcomes, and reported adverse effects. Quality assessment was conducted using established criteria to evaluate study design, methodology, and risk of bias.
The authors independently extracted data through piloted forms, and transcriptions were made into the given database. The data extracted from every report seem to include the attributes of baseline participants, research drug and control treatment, inclusion criteria, endpoint data, and follow-up duration.
Data Synthesis
This review used narrative synthesis. Meta-analysis was deemed unsuitable because the studies were heterogeneous regarding methods, participants, settings, and outcomes. The synthesis steps began with the author’s organisation of the extracted data. As shown in the results and discussion sections, a narrative description of the PPI’s advantages and drawbacks identified from the review was reported and discussed.
Results
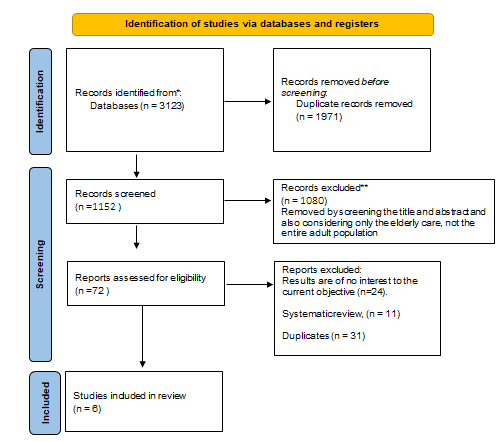
Description of the included reviews Figure 1 shows the studies in the systematic review and the reasons for excluding the others. Out of 3123 studies, only 6 met the inclusion criteria and were included in the review.
| Year | Study design | Population | Region/ Country | Male | Female | Patients | PPIs | |
|---|---|---|---|---|---|---|---|---|
| TeramuraGrönblad M, et al. [50]. | 2010 | Cross-sectional study. | Residents in nursing homes | Helsinki, Finland | 383 | 1604 | 1987 | Users |
| Pilotto A, et al. [51]. | 2004 | Endoscopic examination and structured interviews. | Elderly patients | Italy | 248 | 428 | 3111 | Both users and non-users |
| Maggio M, et al. [52]. | 2013 | Time-dependent Cox regression in discharged patients. | Older patients are charged from acute care hospitals | Italy | 226 | 265 | 491 | Users |
| Wallerstedt SM, et al. [53]. | 2016 | A cohort study in individuals aged ≥65. | Elderly patients | Sweden | 1,25,192 | 1,53,013 | 2,78,205 | 32,421 were on long-term treatment with PPI |
| Sakamoto Y, et al. [54]. | 2013 | Associations between antiulcer drugs and endoscopic findings. | Elderly patients | Japan | 94 | 64 | 158 | Both users and non-users |
| Hsiao FY, et al. [55]. | 2009 | Retrospective cohort study using health database. | Elderly patients | Taiwan | 7212 (PPI users) | 4789 (PPI users) | 14,627 | 12,001 receiving aspirin 2626 receiving clo-Pidogrel |
| Hsiao FY, et al. [55]. | 2009 | Retrospective cohort study using health database. | Elderly patients | Taiwan | 1566 (Clopidogrel) | 1060 (Clopidogrel) | 14,627 | 12,001 receiving aspirin 2626 receiving clo-Pidogrel |
Table 1: Baseline characteristics of the included reviews.
Table 1 shows that the Study designs for the included studies were Cross-sectional, Endoscopic examination and structured interviews, Time-dependent Cox regression in discharged patients, a cohort study in individuals aged ≥65, Associations between antiulcer drugs and endoscopic findings, and a Retrospective cohort study using a health database.
| Benefits of PPIs | Drawbacks of PPIs | |
|---|---|---|
| TeramuraGrönblad M, et al. [50]. | The well-known benefits of PPIs have led to their increased and long-term use as “all-purpose” protectors of the GI tract among older patients. | Increased risk of diarrhoea and prior hip fractures among PPI users. |
| Pilotto A, et al. [51]. | Reduced risk of peptic ulcers in both acute and chronic NSAID/aspirin users. | Long-term PPI treatment may be associated with uncommon, adverse, and severe effects. |
| Maggio M, et al. [52]. | PPIs are no longer significantly associated with an increased risk of the combined endpoint. | High-dose PPIs are associated with increased mortality. |
| Wallerste dt SM, et al [53]. | long-term use of PPI occurs in 12% of the older population, | An increased risk of overuse of PPI in individuals treated with many drugs is that such treatment may reflect multiple comorbidities and, thus, a more significant treatment complexity. |
| Wallerste dt SM, et al [53]. | and for 38% of these, no disease- or drug-related reason can be identified. | greater treatment complexity |
| Sakamoto Y, et al. [54]. | PPIs significantly reduced open ulcers in LDA users. | Potential overuse without PPIs and possible drug interactions and side effects. |
| Hsiao FY, et al. [55]. | Aspirin plus PPI reduced the risk of recurrent hospitalisation for major GI complications. | PPI has few side effects, especially related to short-term use. |
Table 2: Benefits and Drawbacks of PPIs.
Table 2 shows the Benefits and Drawbacks of PPIs.
Benefits of PPIs
PPIs offer significant therapeutic benefits for managing acid-related disorders, particularly in elderly patients:
Gastroesophageal Reflux Disease (GERD)
PPIs effectively reduce gastric acid production, alleviate GERD symptoms, and prevent complications such as esophagitis and Barrett’s oesophagus. Studies demonstrate significant improvements in symptom control and quality of life for patients on PPIs.
Peptic Ulcer Prevention
According to our findings, PPIs reduce the risk of uncomplicated peptic ulcers in elderly aspirin/NSAID users, both acute and chronic. This was observed among 676 elderly NSAID or aspirin users and 2,435 non-users who underwent upper gastrointestinal endoscopy consecutively. The gastric and duodenal ulcers and Helicobacter pylori infection were diagnosed through endoscopic and histological evaluations of the stomach mucosa. PPI use was associated with a lower incidence of peptic ulcers in both acute (OR 0.70, 95% CI: 0.24–2.04) and chronic (OR 0.32, 95% CI: 0.15–0.67) NSAID/aspirin users [50]. Conversely, the use of H2-blockers significantly increased the risk of peptic ulcers in both acute (OR 10.9, 95% CI: 3.87–30.9) and chronic (OR 6.26, 95% CI: 2.56–15.3) NSAID/aspirin users compared to non-users.
PPI treatment reduced the absolute risk of peptic ulcers by 36.6% in acute and 34.6% in chronic NSAID/aspirin users. The number needed to treat to prevent one peptic ulcer in elderly NSAID/aspirin users was three in both acute and chronic users. Study Barrison AF, et al. [56] evaluated the association between PPI usage and the risk of death or the combined endpoint of death or rehospitalisation in older patients discharged from acute care hospitals. One in nine people over 65 uses PPIs long-term, although four out of ten of these individuals have no identifiable justification for PPI use. Nursing home residency, female sex, and a higher number of medications all indicate non-rational long-term PPI usage [57].
Reduced Ulcer Incidence in LDA Patients
Open ulcers among low-dose aspirin (LDA) patients were significantly reduced in those using PPIs compared to those using mucosal protective agents or those who did not receive any antiulcer medication (p < 0.001). NSAID patients on PPIs had a significantly lower incidence of open ulcers than those not given antiulcer medication (p = 0.012). Approximately 70% of patients had open-type atrophic gastritis [53].
Peptic Ulcer Disease Management
In patients with peptic ulcer disease, PPIs promote healing and reduce the risk of recurrence, especially in those using NSAIDs like aspirin. Clinical trials have shown a reduction in ulcer-related complications with PPI therapy. Patients with high GI risk who receive antiplatelet medication along with PPIs have a lower chance of repeat hospitalisation. However, this was not the case when clopidogrel was combined with a PPI [54].
Drawbacks and Risks of PPIs
While PPIs can protect aspirin users against GI complications, their use must be carefully balanced against potential risks, particularly in elderly patients and those on high doses. The studies suggest that PPIs should be prescribed with clear medical justification to manage the benefits and risks effectively.
Several studies have identified potential risks associated with the use of proton-pump inhibitors (PPIs), particularly in high doses and long-term use among older adults.
Increased Risks
Studies Teramura-Grönblad M, et al. [50] and Maggio M, et al. [52] highlight risks such as increased rates of diarrhoea, hip fractures, and even mortality, especially with high-dose PPIs. Study Wallerstedt SM, et al. [53] points out that PPIs are often used long-term without a clear medical indication in older populations, leading to unnecessary exposure to these risks. Study Hsiao FY, et al. [55] indicates that the protective effects of PPIs may not extend to patients on clopidogrel, suggesting that PPI benefits might be specific to the type of antiplatelet therapy used.
Risk Estimates
Ulcer Risk: After adjusting for factors such as age, gender, H. pylori infection, and antisecretory drug use, the risk of peptic ulcers was found to be higher in acute PPI users (gastric ulcer: odds ratio [or] 14.47, 95% CI: 3.19–6.26; duodenal ulcer: OR 14.39, 95% CI: 1.73–3.31) compared to chronic users (gastric ulcer: OR 14.80, 95% CI: 1.97–3.99; duodenal ulcer: OR 14.68, 95% CI: 1.22–2.33) [51].
Mortality Risk: All-cause mortality was observed to be associated with PPI use (hazard ratio [HR] 1.51, 95% CI: 1.03–2.77), with high-dose PPI users having an even higher risk of death compared to non-users (HR 2.59, 95% CI: 1.22– 7.16) [51].
Diarrhoea Risk: PPI users experienced diarrhoea more frequently (19.7%) than non-users (12.9%) (p < 0.001) and had a history of hip fractures more often (28.5% vs 19.4%, p < 0.001). Logistic regression analysis showed an independent association between PPI use and diarrhoea (OR 1.60, 95% CI: 1.20–2.15) [50].
Gastrointestinal Complications
Recurrent hospitalisations for major GI issues were recorded as follows: 0.125 per person-year for aspirin users, 0.103 per person-year for aspirin plus PPI users, 0.128 per person-year for clopidogrel users, and 0.152 per person-year for clopidogrel plus PPI users. PPI users had a significantly lower adjusted risk of hospitalisation for major GI problems compared to non-users (HR 0.76, 95% CI: 0.64–0.91). Among clopidogrel users, PPI use did not significantly reduce risk (HR 1.08, 95% CI: 0.89–1.33) [55].
Other Risks
In the first study, 433 residents were taking PPIs. Univariate analysis linked regular PPI use with factors such as poor functional status, a more significant number of comorbidities, more medications, and lactose intolerance. PPI users were also more likely to have a history of ventricular or duodenal ulcers, malignancy, or coronary heart disease [50].
Discussion
Nursing home patients are the frailest segment of the senior population and are frequently cared for by primary care physicians. They have various comorbidities and are commonly given a large number of concurrent medications [58, 59]. As a result, they are vulnerable to drug-drug interactions and other undesirable consequences. Furthermore, few nursing home patients have the opportunity for a full appraisal of their medication following admission [56]. As a result, their usage of those pharmaceuticals meant for a limited time is frequently extended for lengthy periods. This study tests the benefits and drawbacks of using PPIs as a protective agent for aspirin users in long-term care and senior residents.
Teramura-Grönblad M, et al. [50] highlight that PPI users have some issues like an increased number of comorbidities, a more significant number of medications, and intolerance of lactose. Users were more likely than non-users to have had a previous duodenal or ventricular ulcer, malignancy, or coronary heart disease. However, previous studies shared contradictory results, such as PPIs being the most efficient medications for reducing stomach acid secretion [50]. Primary care physicians commonly use them to treat acid- peptic illnesses [56, 57, 60]. Furthermore, they lower the risk of GI bleeding associated with nonsteroidal anti-inflammatory medications (NSAIDs) and low-dose aspirin [61]. However, in line with our study review, the therapy of PPIs has also been linked to an increased incidence of hip fractures [62]. PPIs have been hypothesised to impair calcium absorption by inducing hypochlorhydria and limiting bone regeneration by inhibiting osteoclastic vacuolar proton pumps [63].
One of the systematic review’s limitations was its inclusion of non-RCTs, which are susceptible to selection bias, confounding bias, and baseline differences between the experimental and control groups. This potential bias should be considered when interpreting the results, particularly in the context of the available safer PPIs combined with aspirin and clopidogrel.
Conclusion
Proton Pump Inhibitors (PPIs) prevent gastrointestinal complications, especially in elderly patients using NSAIDs or aspirin; their long-term use should be judiciously considered to optimise patient outcomes. It’s essential to balance managing symptoms and minimising potential risks. Like any other pharmacological therapy, PPI medication has potential side effects. However, for most patients, the benefits of improved quality of life outweigh the risks. Following evidence-based guidelines is essential to ensure effective and safe PPI therapy. Limitation The chosen randomised controlled trials (RCTs) do not address the challenge of non-communicating long-term care patients, making it difficult to identify aspirin-induced acidity in this population.
Policy Implications
Evidence-based guidelines are essential for effective and safe PPI therapy, especially in elderly populations. The available data suggest the following policy implications regarding Proton Pump Inhibitors (PPIs):
Conjunction with NSAIDs and Aspirin
- PPIs should be used alongside nonsteroidal anti- inflammatory medications (NSAIDs) and aspirin in symptomatic elderly individuals who require treatment for a limited period.
- This combination helps mitigate the risk of gastrointestinal (GI) complications, especially GI bleeding, which can occur due to NSAID or aspirin use [64].
Randomised Controlled Trials (RCTs)
- Further research is needed through well-designed randomised controlled trials that specifically include elderly and fragile patients.
- These trials should address the challenge of non- communicating long-term care patients and provide evidence on the effectiveness and safety of PPIs in this population.
Balancing Benefits and Risks
- Clinicians must exercise caution when considering long- term use of high-dose PPIs in older patients.
- The advantages (GI protection) and risks (potential adverse effects) of prolonged PPI therapy should be carefully weighed for each patient.
References
-
Vane J, Botting R (2003) The mechanism of action of aspirin. Thromb Res 110(5–6): 255-258.
-
Warner TD, Nylander S, Whatling C (2011) Anti- platelet therapy: cyclo-oxygenase inhibition and the use of aspirin with particular regard to dual antiplatelet therapy. Br J Clin Pharmacol 72(4): 619-633.
-
Baigent C, Blackwell L, Collins R, Emberson J, Godwin J, et al. (2009) Aspirin in the primary and secondary prevention of vascular disease: a collaborative meta- analysis of individual participant data from randomised trials. Lancet 373(9678): 1849-1860.
-
Ikeda Y, Shimada K, Teramoto T, Uchiyama S, Yamazaki T, Oikawa S, et al. (2014) Low-Dose Aspirin for Primary Prevention of Cardiovascular Events in Japanese Patients 60 Years or Older With Atherosclerotic Risk Factors. JAMA 312(23): 2510-2520.
-
Mohr JP, Thompson JLP, Lazar RM, Levin B, Sacco RL, et al. (2001) A Comparison of Warfarin and Aspirin for the Prevention of Recurrent Ischemic Stroke. N Engl J Med 345(20): 1444-1451.
-
Gorelick PB (2003) Aspirin and Ticlopidine for Prevention of Recurrent Stroke in Black Patients. JAMA 289(22): 2947-2957.
-
Derry S, Loke YK (2000) Risk of gastrointestinal haemorrhage with long term use of aspirin: meta- analysis. BMJ 321(7270): 1183-1187.
-
He J, Whelton PK, Vu B, Klag MJ (1998) Aspirin and Risk of Hemorrhagic Stroke. JAMA 280(22): 1930-1935.
-
Gingold-Belfer R, Issa N, Boltin D, Beloosesky Y, Koren- Morag N, et al. (2023) Gastric cancer risk in the elderly is associated with omeprazole use and inversely associated with aspirin use. Eur J Gastroenterol Hepatol. 35(9): 968-973.
-
García Rodríguez LA, Soriano-Gabarró M, Vora P, Cea Soriano L (2020) Low-dose aspirin and risk of gastric and oesophageal cancer: A population-based study in the United Kingdom using The Health Improvement Network. Int J Cancer 147(9): 2394-2404.
-
Yu SY, Ip MS, Li X, Cheung KS, Ren QW, et al. (2022) Low- dose aspirin and incidence of lung carcinoma in patients with chronic obstructive pulmonary disease in Hong Kong: A cohort study. PLoS Med 19(1): e1003880.
-
Tseng ZF, Hsu PI, Peng NJ, Kao SS, Tsay FW, et al. (2021) Omeprazole vs famotidine for preventing gastroduodenal injury in high-risk low-risk aspirin users: A randomised controlled trial. J Chin Med Assoc. 84(1): 19-24.
-
Jung M, Lee S (2020) Efficacy of Aspirin in the Primary Prevention of Cardiovascular Diseases and Cancer in the Elderly: A Population-Based Cohort Study in Korea. Drugs Aging 37(1): 43-55.
-
Lanas Á, Carrera-Lasfuentes P, Arguedas Y, García S, Bujanda L, et al. (2015) Risk of Upper and Lower Gastrointestinal Bleeding in Patients Taking Nonsteroidal Antiinflammatory Drugs, Antiplatelet Agents, or Anticoagulants. Clin Gastroenterol Hepatol 13(5): 906- 912.e2.
-
Hernández-Díaz S, García Rodríguez LA (2006) Cardioprotective aspirin users and their excess risk of upper gastrointestinal complications. BMC Med 4(1): 22.
-
Thorat MA, Cuzick J (2015) Prophylactic use of aspirin: a systematic review of harms and approaches to mitigation in the general population. Eur J Epidemiol 30(1): 5-18.
-
Lin KJ, Hernández–Díaz S, García Rodríguez LA (2011) Acid Suppressants Reduce Risk of Gastrointestinal Bleeding in Patients on Antithrombotic or Anti- Inflammatory Therapy. Gastroenterology 141(1): 71-99.
-
Mo C, Sun G, Lu ML, Zhang L, Wang YZ, et al. (2015) Proton pump inhibitors in prevention of low-dose aspirin-associated upper gastrointestinal injuries. World J Gastroenterol 21(17): 5382-5392.
-
Moayyedi P, Eikelboom JW, Bosch J, Connolly SJ, Dyal L, et al. (2019) Pantoprazole to Prevent Gastroduodenal Events in Patients Receiving Rivaroxaban and Aspirin in a Randomized, Double-Blind, Placebo-Controlled Trial. Gastroenterology 157(2): 403-412.e5.
-
Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, et al. (2020) 2019 ESC Guidelines for diagnosing and managing chronic coronary syndromes: The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J 41(3): 407-477.
-
Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, et al. (2020) 2019 ESC Guidelines on diabetes, pre- diabetes, and cardiovascular diseases developed with the EASD. Eur Heart J 41(2): 255-323.
-
Abraham NS, Hlatky MA, Antman EM, Bhatt DL, Bjorkman DJ, et al. (2010) ACCF/ACG/AHA. ACCF/ACG/AHA 2010 Expert Consensus Document on the concomitant use of proton pump inhibitors and thienopyridines: a focused update of the ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. Circulation 122(24): 2619-2633.
-
Bruno G, Zaccari P, Rocco G, Scalese G, Panetta C, et al. (2019) Proton pump inhibitors and dysbiosis: Current knowledge and aspects to be clarified. World J Gastroenterol 25(22): 2706-1719.
-
Freedberg DE, Lebwohl B, Abrams JA (2014) The Impact of Proton Pump Inhibitors on the Human Gastrointestinal Microbiome. Clin Lab Med 34(4): 771-785.
-
Jackson MA, Goodrich JK, Maxan M-E, Freedberg DE, Abrams JA, et al. (2016) Proton pump inhibitors alter the composition of the gut microbiota. Gut 65(5): 749-756.
-
Sugano K, Kinoshita Y, Miwa H, Takeuchi T (2012) Randomised clinical trial: esomeprazole for preventing nonsteroidal anti-inflammatory drug-related peptic ulcers in Japanese patients. Aliment Pharmacol Ther 36(2): 115-125.
-
Hawkey CJ, Karrasch JA, Szczepañski L, Walker DG, Barkun A, et al. (1998) Omeprazole Compared with Misoprostol for Ulcers Associated with Nonsteroidal Antiinflammatory Drugs. N Engl J Med 338(11): 727- 734.
-
Yeomans ND, Tulassay Z, Juhász L, Rácz I, Howard JM, et al. (1998) A Comparison of Omeprazole with Ranitidine for Ulcers Associated with Nonsteroidal Antiinflammatory Drugs. N Engl J Med 338(11): 719-726.
-
Sugano K, Choi M-G, Lin J-T, Goto S, Okada Y, et al. (2014) The LAVENDER study is a multinational, double-masked, randomised, placebo-controlled, prospective study of esomeprazole in preventing recurrent peptic ulcers in low-dose acetylsalicylic acid users. Gut 63(7): 1061- 1068.
-
Lin C-Y, Wang C-W, Hui C-YR, Chang Y-C, Yang C-H, et al. (2018) Delayed-type hypersensitivity reactions induced by proton pump inhibitors: A clinical and in vitro T-cell reactivity study. Allergy 73(1): 221-229.
-
Badiola N, Alcalde V, Pujol A, Münter L-M, Multhaup G, et al. (2013) The Proton-Pump Inhibitor Lansoprazole Enhances Amyloid Beta Production. Ginsberg SD, editor. PLoS One 8(3): e58837.
-
Mori S, Kadochi Y, Luo Y, Fujiwara-Tani R, Nishiguchi Y, et al. (2017) Proton pump inhibitor-induced collagen expression in colonocytes is associated with collagenous colitis. World J Gastroenterol 23(9): 1586-1593.
-
Endo H, Sakai E, Taniguchi L, Kessoku T, Komiya Y, et al. (2014) Risk factors for small-bowel mucosal breaks in chronic low-dose aspirin users: data from a prospective multicenter capsule endoscopy registry. Gastrointest Endosc 80(5): 826-834.
-
Watanabe T, Sugimori S, Kameda N, Machida H, Okazaki H, et al. (2008) Minor Bowel Injury by Low-Dose Enteric- Coated Aspirin and Treatment With Misoprostol: A Pilot Study. Clin Gastroenterol Hepatol 6(11): 1279-1282.
-
Nagata N, Niikura R, Aoki T, Sakurai T, Moriyasu S, et al. (2015) Effect of proton pump inhibitors on the risk of lower gastrointestinal bleeding associated with NSAIDs, aspirin, clopidogrel, and warfarin. J Gastroenterol 50(11): 1079-1086.
-
Lanas A, Dumonceau J-M, Hunt RH, Fujishiro M, Scheiman JM, et al. (2018) Nonvariceal upper gastrointestinal bleeding. Nat Rev Dis Prim 4(1): 18020.
-
Clooney AG, Bernstein CN, Leslie WD, Vagianos K, Sargent M, et al. (2016) A comparison of the gut microbiome between long-term users and non-users of proton pump inhibitors. Aliment Pharmacol Ther 43(9): 974-984.
-
Freedberg DE, Kim LS, Yang Y-X (2017) The Risks and Benefits of Long-term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology 152(4): 706-715.
-
Arai N, Nakamizo T, Ihara H, Koide T, Nakamura A, et al. (2017) Histamine H2Blocker and Proton Pump Inhibitor Use and the Risk of Pneumonia in Acute Stroke: A Retrospective Analysis on Susceptible Patients. Mills K, editor. PLoS One 12(1): e0169300.
-
Momosaki R, Yasunaga H, Matsui H, Fushimi K, Abo M (2016) Proton Pump Inhibitors versus Histamine-2 Receptor Antagonists and Risk of Pneumonia in Patients with Acute Stroke. J Stroke Cerebrovasc Dis 25(5): 1035- 1040.
-
Niu Q, Wang Z, Zhang Y, Wang J, Zhang P, et al. (2017) Combination Use of Clopidogrel and Proton Pump Inhibitors Increases Major Adverse Cardiovascular Events in Patients With Coronary Artery Disease. J Cardiovasc Pharmacol Ther 22(2): 142-152.
-
Wijarnpreecha K, Thongprayoon C, Chesdachai S, Panjawatanana P, Ungprasert P, et al. (2017) Associations of Proton-Pump Inhibitors and H2 Receptor Antagonists with Chronic Kidney Disease: A Meta-Analysis. Dig Dis Sci 62(10): 2821-2827.
-
Cheungpasitporn W, Thongprayoon C, Kittanamongkolchai W, Srivali N, Edmonds PJ, et al. (2015) Proton pump inhibitors linked to hypomagnesemia: a systematic review and meta-analysis of observational studies. Ren Failure 37(7): 1237-1241.
-
Park CH, Kim EH, Roh YH, Kim HY, Lee SK (2014) The Association Between the Use of Proton Pump Inhibitors and the Risk of Hypomagnesemia: A Systematic Review and Meta-analysis. Green J, editor. PLoS One 9(11): e112558.
-
Pignone M, Earnshaw S, Tice JA, Pletcher MJ (2006) Aspirin, Statins, or Both Drugs for the Primary Prevention of Coronary Heart Disease Events in Men: A Cost–Utility Analysis. Ann Intern Med 144(5): 326.
-
Saini SD, Schoenfeld P, Fendrick AM, Scheiman J (2008) Cost-effectiveness of Proton Pump Inhibitor Cotherapy in Patients Taking Long-term, Low-Dose Aspirin for Secondary Cardiovascular Prevention. Arch Intern Med 168(15): 1684-1690.
-
Earnshaw SR, Scheiman J, Fendrick AM, McDade C, Pignone M (2011) Cost-Utility of Aspirin and Proton Pump Inhibitors for Primary Prevention. Arch Intern Med 171(3): 218-225.
-
Greving JP, Buskens E, Koffijberg H, Algra A (2008) Cost-effectiveness of Aspirin Treatment in the Primary Prevention of Cardiovascular Disease Events in Subgroups Based on Age, Gender, and Varying Cardiovascular Risk. Circulation 117(22): 2875-2883.
-
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, et al. (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Systematic Reviews 10: 89.
-
Teramura-Grönblad M, Hosia-Randell H, Muurinen S, Pitkala K (2010) Use of proton-pump inhibitors and their associated risks among frail elderly nursing home residents. Scand J Prim Health Care 28(3): 154-159.
-
Pilotto A, Franceschi M, Leandro G, Paris F, Cascavilla L, et al. (2004) Proton-pump inhibitors reduce the risk of uncomplicated peptic ulcers in older people, either acute or chronic users of aspirin/non-steroidal anti- inflammatory drugs. Aliment Pharmacol Ther 20(10): 1091-1097.
-
Maggio M, Corsonello A, Ceda GP, Cattabiani C, Lauretani F, et al. (2013) Proton Pump Inhibitors and Risk of 1-Year Mortality and Rehospitalization in Older Patients Discharged From Acute Care Hospitals. JAMA Intern Med 173(7): 518-523.
-
Wallerstedt SM, Fastbom J, Linke J, Vitols S (2017) Long-term use of proton pump inhibitors and prevalence of disease- and drug-related reasons for gastroprotection-a cross-sectional population-based study. Pharmacoepidemiol Drug Saf 26(1): 9-16.
-
Sakamoto Y, Shimoyama T, Nakagawa S, Mikami T, Fukuda S (2014) Proton Pump Inhibitor Treatment Decreases the Incidence of Upper Gastrointestinal Disorders in Elderly Japanese Patients Treated with NSAIDs. Intern Med 53(11): 1107-1111.
-
Hsiao FY, Tsai YW, Huang WF, Wen YW, Chen PF, et al. (2009) A comparison of aspirin and clopidogrel with or without proton pump inhibitors for the secondary prevention of cardiovascular events in patients at high risk for gastrointestinal bleeding. Clin Ther 31(9): 2038- 2047.
-
Barrison AF, Jarboe LA, Weinberg BM, Nimmagadda K, Sullivan LM, et al. (2001) Patterns of proton pump inhibitor use in clinical practice. Am J Med 111(6): 469- 473.
-
Vigneri S, Termini R, Leandro G, Badalamenti S, Pantalena M, et al. (1995) A Comparison of Five Maintenance Therapies for Reflux Esophagitis. N Engl J Med 333(17): 1106-1110.
-
Avorn J, Gurwitz JH (1995) Drug use in the nursing home. Ann Intern Med 123(3): 195-204.
-
Hanlon JT, Schmader KE, Ruby CM, Weinberger M (2001) Suboptimal Prescribing in Older Inpatients and Outpatients. J Am Geriatr Soc 49(2): 200-209.
-
Salas M, Ward A, Caro J (2002) Are proton pump inhibitors the first choice for acute treatment of gastric ulcers? A meta-analysis of randomised clinical trials. BMC Gastroenterol 2(1): 17.
-
Porro GB, Lazzaroni M, Petrillo M, Manzionna G, Montrone F, et al. (1998) In patients receiving continuous NSAID treatment, Prevention of gastroduodenal damage with omeprazole. A double-masked placebo-controlled study. Ital J Gastroenterol Hepatol 30(1): 43-47.
-
Yang YX, Lewis JD, Epstein S, Metz DC (2006) Long-term proton pump inhibitor therapy and risk of hip fracture. JAMA 296(24): 2947-2953.
-
Moayyedi P, Cranney A (2008) Hip fracture and proton pump inhibitor therapy: balancing the evidence for benefit and harm. Am J Gastroenterol 103(10): 2428- 2431.
-
Wolfe MM, Sachs G (2000) Acid suppression: Optimizing therapy for gastroduodenal ulcer healing, gastroesophageal reflux disease, and stress-related erosive syndrome. Gastroenterology 118(2): S9-31.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda