Catastrophic Health Expenditure among Females with Breast Cancer in Radioisotope Centre Khartoum: A Cross-Sectional Facility-Based Study
Introduction: Equity is an important health and ethical concept, emphasized and recommended by the World Health Organization (WHO), and one of the health system performance assessment methods. Patients have to pay out of pocket to purchase health services, which might reduce their income and sometimes exhaust their savings and earnings to the point that it will turn catastrophic. Breast cancer is one of the chronic diseases that imposes heavy economic burdens and has high costs. This study attempted to determine the incidence of catastrophic health expenditure among households with women who have breast cancer. Methods: A descriptive, analytical, cross-sectional study design. It was conducted at the outpatient clinic at the Radioisotope Center Khartoum, including households with breast females who have breast cancer patients older than 18 years with a treatment duration of not less than two weeks. 170 women out of 432 were interviewed through a closed-ended questionnaire. Data were processed and analysed using the Statistical Package for the Social Sciences (SPSS V20). The correlation was tested by chi-square and logistic regression. Findings: 79.4% of patients faced catastrophic health expenditures. There were significant relationships between catastrophic health expenditures and coverage with insurance, total household expenditures, and having an extra job. Conclusion: This high incidence of catastrophic health expenditure is alarming, and it means that no one is immune against, so a bunch of protection measures and actions have to be implemented, and polices have to be revised, especially for cancer patients. Also, insurance policies and schemes have to be evaluated and revised. More space and resources have to be given to the early detection of breast cancer alongside education and awareness campaigns.
Abbreviations
AIDS: Acquired Immunodeficiency Syndrome; CI: Confidence Interval; CHE: Catastrophic Health Expenditure; CTP: Capacity to Pay; EXP: Household Consumption Expenditure; FE: Food Expenditure; FFC: Fairness in Financial Contribution Index; FMOH: Federal Ministry of Health; GDP: Gross Domestic Product; HIV: Human Papillomavirus; IARC: International Agency of Research in Cancer; LMC: Low and Middle-Income Countries; MDGs: Millennium Development Goals; NHA: National Health Account; NHIF National Health Insurance Fund; NCD: Non-Communicable Disease; THHE: Total Household Expenditure; UNDP: United Nations Development Program; WHO: World Health Organization; NCI: National Cancer Institute; NCMS: New Corporation Medical Insurance Scheme; NCR: National Cancer Registry; NCS: National Cancer Strategy; OOP: Out-of-Pocket Health Expenditure; OOPCTP: Out-of-Pocket Health Payments Share of Household Capacity to Pay; OR: Odd Ratio; PL: Poverty Line; RDF: Revolving Drug Fund; RICK: Radio Isotope Centre Khartoum; SDG: Sudanese Pound; SE: Household Subsistence Spending; SES: Socioeconomic Status; SMSB: Sudan Medical Specialization Board; SPSS: Statistical Package for the Social Sciences.
Definition of Terms
Out-of-Pocket Health Expenditure (OOP) refers to the payments made by households when they receive health services. Typically, these include doctor’s consultation fees, medication purchases, and hospital bills. Spending on alternative and traditional medicine, health-related transportation, and special nutrition are also included in out- of-pocket payments. It is also important to note that out-of- pocket payments are the net of any insurance reimbursement.
Household Consumption Expenditure (EXP) comprises monetary and in-kind payment for all goods and services and the monetary value of home-made product consumption.
Food Expenditure (Food): is the amount spent on all foodstuffs by the household plus the value of the family’s food production consumed within the household. However, it excludes expenditure on alcoholic beverages, tobacco, and food outside the home (e.g. hotels and restaurants).
Poverty Line (Pl) And Household Subsistence Spending (Se) are the minimum requirements for maintaining a basic life in a society. A poverty line is used in the analysis as subsistence spending. A food shares-based poverty line to estimate household subsistence. This poverty line is defined as the food expenditure of the household whose food expenditure share of total household expenditure is at the 50th percentile in the country.
The Household’s Capacity to Pay (CTP) is defined as its non- subsistence effective income. However, some households may report lower food expenditures than subsistence spending. This indicates that the household’s food expenditures are less than the estimated poverty standard for that country.
Out-of-Pocket Health Payments Share of Household Capacity to Pay (OOPCTP): The burden of health payments is defined as the out-of-pocket payments as a percentage of a household’s capacity to pay.
Fairness in Financial Contribution Index (FFC): To allow for comparisons, the distribution of household financial contribution across households has been summarized using an index called Fairness of Financial Contribution (FFC). This index is designed to weigh heavily on those households that have spent a substantial share of their beyond-subsistence adequate income on health. The index thus reflects overall inequality in household financial contribution to the health system but mainly reflects those households facing catastrophic health expenditure. FFC is based on the mean of the cubed absolute difference between the oopctp of a given household and the (oopctp) norm. FFC ranges between 0 and 1. The fairer the health financing system, the closer FFC will be to 1.
Impoverishment (IMPOOR): A non-poor household is impoverished by health payments when it becomes poor after paying for health services. The variable created to reflect the poverty impact of health payments (impoorh) is defined as 1 when household expenditure is equal to or higher than subsistence spending but is lower than subsistence spending net of out- of-pocket health payments, and 0 otherwise. [1].
Introduction
Healthcare is concerned with the use of health services, financing, and distribution of resources [2], and the enjoyment of healthcare services is an inherent right for every person, and it has to be served in an equitable manner. Healthcare is a social determinant as long as it is affected by social policies; this term was adopted to include receipt/utilization of health services and the allocation of healthcare resources, the financing of healthcare and the quality of healthcare services. Equity in health can be defined as the absence of systematic disparities in health (or in the major social determinants of health) between social groups of different social levels (different positions in a social hierarchy). Inequities in health deepen the discrimination and increase the sufferings of socially underprivileged people concerning their health; health is substantial for wellbeing and vanquishing other effects of social disadvantage [2]. Equality can be evaluated based on particular, measurable outcomes, while equitability is a generic concept, and its judgment opens the gate widely for interpretation. As a matter of fact, those holding the keys of power and authority are likely to set at a community level what is equitable and what is not when it comes to the allocation of resources necessary for health. Accordingly, equality is a decisive juncture in the endeavour towards the achievement of equity in health [2]. Socioeconomic inequalities in health are defined as differences in the incidence or the prevalence of health problems among individuals of high and low socioeconomic status [3].
According to the WHO health system conceptual framework, fair financial contribution and the protection of households from catastrophic healthcare costs are desirable objectives of the health system. Also, the performance of any health system can be evaluated based on the achievement of three goals: improvement in health, the responsiveness of health to people’s expectations [4], and fairness in financing and financial risk protection [5]; this was emphasized by the World Health Organization (WHO) and given high attention [6]. Financial contribution to the health system is said to be fair when payments are assigned according to the financial ability [3], and it is defined as the ratio of the household’s payment for the health system to its capacity to pay (CTP); it has to be monitored and measured annually [6].
Health system financing is concerned with collecting money from variable sources into funds, which will be mobilized and allocated to cover the health care needs of people [7]. Some health system characteristics were given due consideration in assessing financing mechanisms, namely, the extent to which any nation would depend on out- of-pocket (OOP) payments (user fees and patients’ direct payments to private providers) to finance the health system. Besides that, there are other financing sources: taxes, social insurance contributions, private insurance premiums and community financing. So, as far as there is considerable prepayment, financial catastrophewill decline tremendously [8].
Communities have been alarmed by the escalating cost of healthcare globally and the implementation of equity in financial contributions to health systems. These health systems should ensure that people are not deprived of health services because they cannot pay. Making healthcare services accessible to everyone is the mainstay of contemporary healthcare financing in many countries. Equity-based financing systems won the lion’s share in health system deliberations [3]. Different nations used variable methods to finance their health system according to their culture, history and disciplines. These resources include tax-based insurance, social insurance, private insurance and Out-of- Pocket (OOP) payment [9]. The fairness of these financing processes is concluded based on how much households will pay to meet health expenditures. Moreover, OOP payment is a standard measure of the financial burden of seeking healthcare and is measured over a period of a year or less. An effective health insurance scheme will reduce health expenditures and provide protection from large financial losses. [10].
In most developing countries, out-of-pocket (OOP) payment for health services might impose a financial risk upon people and affect their living essentials, and make the choice of either continuing or ceasing treatment at the expense of these essentials a big challenge. Furthermore, the continuation of treatment will deplete the available resources, undermine the income, jeopardize wellbeing and force households to sacrifice assets to keep pace with the high cost of treatment, which might drag them into poverty. Therefore, the spending will turn into a catastrophe [11, 12, 13]. Health expenses might not be costly, but at least they are high enough for poor households to afford, unlike rich people [12, 13, 14]. So, catastrophic health expenditure (CHE) is defined as the spending on health that exceeds 40 per cent of a household’s total costs and its capacity to pay [14, 15, 16]. There are different thresholds and cut-off points to measure the CHE. Therefore, there is no agreement about this issue; it lies within the range of 5-20% of the total household income [13, 17, 18]. On the other hand, health expenditure can be catastrophic if it exceeds 40% of income remaining after subsistence needs have been met [14]. The picture is quite different between developed and developing countries; people in developed countries are protected against CHE due to adequate insurance coverage and a well-funded health system, while those in the developing world are exposed easily to catastrophes because of the inefficiency of health system financing and lack of proper health system funding [14]. There are certain features that would put households at risk of catastrophic health expenditure, such as low income and chronic disease [17, 18].
Cancer is an example of a chronic disease; it killed 7.6 million individuals in 2008, and every year, there are 12.4 million individuals diagnosed with cancer. The worldwide cost of cancer treatment is $895 billion annually [19]. It has been realized that cancer has a profound impact on recently diagnosed patients, old ones and their families, and almost all families who had cancer patients face heavy financial burdens and big economic losses [20, 21, 22]. Cancer patients are more likely to report financial difficulties than persons without cancer [22]. Costs of cancer include direct costs due to treatment, expenses related to treatment like transportation, or indirect expenses related to the changes in lifestyle and needs [23]. Some patients might have a drop in income because of absence from work [24]. Some socially or economically disadvantaged patients may be particularly vulnerable to the adverse financial and economic effects of cancer [25].
Breast cancer is newly diagnosed in more than 1 million women worldwide and causes the death of more than 400,000 women annually [26]. It is growing worldwide, especially in developing regions, where the incidence has increased as much as 5% per year [27]. The escalating cost of breast cancer treatment was acknowledged worldwide and addressed by the 58th World Health Assembly [28]. If household heads were women, the devastating effect would be tremendous; this is the case when sick women have low-income or marginal jobs. It was found in the literature. Several research investigates the CHE in breast cancer patient homes, including Cheng-yao et al.’s study to assess the CHE and determinant in breast cancer patients they observed that the. Before and after insurance settlement, the overall incidence of CHE was 66.28% and 87.95, respectively. Education, illness course, health insurance, style of therapy, and income were all found to be significant predictors of CHE in the logistic regression model. Distress financing was estimated to be at 72.4% and the CHE of breast cancer to be at 84.2% [29], according to another study conducted in India. Distress financing and CHE were more common in rural, impoverished, and agriculturally reliant households. In order to cover the expense of their care, almost 80% of the patients used several different sources of funding [30].
The important indicators According to a different US survey, 31.8% of breast cancer patients said their annual medical costs exceeded 10% of their income. According to models, there was an inverse relationship between rising income and the percentage of breast cancer patients who had uninsurable medical costs and lost their jobs. Breast cancer patients had a drop in the mean number of months without insurance and an increase in costs during the Affordable Care Act’s adoption [31]. Another study in Iran revealed that each patient paid an average of $US 97.87 per month for the services they received, resulting in a 5.07% poverty rate and exposing 13.77% of their households to CHE. Due to the fact that they have to spend a significant portion of their little income on purchasing the necessary services, the poor have been the group most affected by these indicators. [32] Women with cancer were more likely than men with cancer to have poor family support, to be without a spouse, and to pay for transportation, nursing care, and house cleaning. Cancer patients pay heavily greatly to have health services, so they are at high risk of being financially undermined and have catastrophic expenditure [33].
Accordingly, households who had CHE used different strategies to cope with it, such as borrowing money [34] and selling their assets [35]. However, some of these strategies might drag households into poverty; this could be worse for those who lack sufficient property, savings, or access to social networks to help them.
Sudan is one of the biggest countries in Africa; it has rapidly increased in per capita income, with a per capita GDP of US$1,500. In spite of that, the country’s human development outcomes remain weak. Out of 169 countries in Africa, Sudan ranks 154 in UNDP’s 2010 Human Development Index. Its income is 25% more than Sub-Saharan Africa’s average, although there is a high incidence of poverty; about 46.5% of the population is below the poverty line, with a clear discrimination between rural and urban areas, for instance, the incidence of poverty in Khartoum state is 26.0% and 69.4% in North Darfur [36]. The Sudan National Health Account (NHA) stated that almost 63% of the total funds (equivalent to 3% of GDP) were paid by households as out of pocket, whereas 29% were public funds, 4% were donated by international donors or other sources and the remaining 3% were from other private sources. The public expenditure on health among the total health expenditure in 2008 was 30% [37]. All these payments are directed towards healthcare providers and pharmacies on an out- of-pocket basis, rendering access to healthcare quite difficult. In Sudan, general tax-based systems and/or social health insurance systems are combined with large out-of-pocket payments by households. Also, there are many public and private healthcare financing sources. These include:
- The Ministry of Health financing covers all Sudanese citizens not dependent on the income of the beneficiary.
- National Health Insurance Schemes.
- The Armed Forces employment-based social insurance schemes.
- A growing private insurance market.
- Out-of-pocket expenditures.
Breast cancer is the most common cancer in Sudan in general and among females in particular; it puts the patients at risk of incurring catastrophic health expenditures and can drive them into poverty. The GLOBOCAN project provided contemporary estimates of the incidence of mortality and prevalence for major types of cancer. In Sudan, it belongs to the International Agency for Research on Cancer (IARC); its most recent estimates for 2012 state that breast cancer ranks first in Sudan with an incidence rate of 11.7% among both sexes and 31.8% among females, with 24%, and 45.5% figures for mortality and five-year prevalence, respectively [38]. Breast cancer cases in the Radiology and Isotope Center of Khartoum (RICK) represent 29-34.5% of all the cancers seen at RICK [39], it also ranks first among cancers in females, accounting for (46.72%) of females’ cancer. It has an incidence rate of 25.1 per 100,000. Most of the breast cancer cases occur between the middle of both the fourth and sixth decades of life (55%). On the other hand, the least cases occur before mid-teens (0.3%). Most patients presented with late advanced disease, only 5-7% presented with stage I and 13-15% presented with stage II diseases [39]. Although first- line chemotherapy and radiotherapy treatment are provided for all breast cancer patients for free through the Ministry of Finance, other direct and indirect financial costs can still pose a financial threat to these patients.
It is of particular importance in the light that the average household consumes an average of 20% of its income on health expenditures. Nevertheless, there are no known studies that consider the overall incidence of catastrophic health expenditure in Sudan; this study aims to answer the following question: Are availing of free chemotherapy and radiotherapy alone sufficient for protecting breast cancer females from high OOP and catastrophic health expenditure? How many breast cancer females are trapped in the catastrophic outcome? What are the main factors contributing to the catastrophic health expenditure? What are the main coping strategies adopted by families to face such problems?
Materials and Methods
Study Design
An analytic cross-sectional, facility-based design.
Study Area
The RICK (Radiation and Isotopes Centre Khartoum) is among the three centres concerned with cancer management in Sudan. In addition, there is the National Cancer Institute (NCI) at Wad Medani and the Shandi Cancer Center at River Nile State. RICK is the main referral center and treats the largest number of cancer cases in Sudan. Despite the fact that it is affiliated with the curative medicine administration in Khartoum state, it acts as a referential regional cancer receiving cancer cases from all states. Data were collected at the outpatient department (OPD) of RICK. The RICK was established in 1967; It has a capacity of 100 beds. The Department of Radiation Oncology has four external beam machines (two linear accelerators and two Co-60). The waiting period ranges from one day to three months, depending on curative or palliative intent. Seventy per cent of patients are treated with palliative intent, and the remaining patients receive curative intent. The staff is composed of 25 radiation oncologists, 65 radiation technologists, 10 medical physicists and ten biomedical maintenance engineers. For chemotherapy, eighty beds are available for male and female patients. Chemo- radiation is being used for 25 patients daily. Overall, 140-150 patients are receiving chemotherapy. Surgeries for cancer patients are referred to and performed outside the RICK. The clinical pharmacy was started in 2007 [40].
Study Population
Case definition: The following characteristics were considered in this study: Socio-demographic status: age, number of children, educational level, occupation, income and marital status. Health status: duration of diseases, co-morbid diseases, type of treatment, complications.
These patient characteristics affected the capacity to pay and further the catastrophic expenditure.
The basic unit of economic analysis in this study is a female with breast cancer (Cancer that forms in tissues of the breast) above the age of 18 years and her household (i.e. those who share a common kitchen with the patient at the home address).
Inclusion and exclusion criteria: females with breast cancer and their households who attend the outpatient clinic at RICK. Patients with a since they didn’t spend much on treatment, patients with cancer who didn’t report any cancer-related treatment were also excluded.
Sampling
Sample size calculation: For this study, the Cochran formula was used because the caseload was 1303 in the previous year, 2013, which is less than 10000. There is no known previous estimation of overall CHE in Sudan; the catastrophic rate of Sri Lanka was adopted as an estimated proportion of an attribute that is present in the population since it’s the closest country to Sudan in its Gross Domestic Product (GDP) which is the main determinant of economic status. Sudan: 59,940 billion US$ Sri Lanka: 59,410 billion US$ Sample size Equation: 2
2 0 Z n pq e = Where: n0 = the sample size Z = the abscissa of the normal curve that cuts off an area α at the tails. Here, it is equal to 1.96 at a confidence level of 95%) P = is the estimated proportion of an attribute that is present in the population; it was taken as (0.125), the CHE in Sri Lanka (GDP of Sri Lanka ≈ to Sudan). q = 1- p = 1- 0.125 = 0.875 e = desired margin of error (0.05) or the desired level of precision. So, n0 = (1.96)2 x0.125x0.875 / 0.05x0.05 = 168.04 Patients = 168 ≈ 170 patients.
Data-Collection Techniques Used for the Different Study Populations
Tools of data collection: Data were collected by means of a closed-ended questionnaire, which was adopted from the Household Survey Questionnaire 2010. Description of formats and procedures: A face-to-face interview was chosen as the data-collection technique; it involves oral questioning of respondents within the hospital premises; the questionnaire contained many questions about health expenditure and addressed to the patient and the companion. If the house head didn’t attend the interview, then other questions related to expenditure were obtained from the head of the household by telephone calls, and answers to questions posed during the interview were recorded by writing them down right away during the interview itself, Throughout the implementation of research tools, the process was straightforward and flexible to great extent to allow easy and smooth flow of questioning and thereby maximizing the efficiency, any patient with breast cancer who fulfilled the inclusion criteria in the outpatient clinic was selected.
Data were collected within a five-month period. Hundred and seventy patients were interviewed and selected out of 432 patients (the total number of breast cancer patients). Unfortunately, the attendance of patients was not regular and smooth because of the autumn season in Sudan, which cut off roads and suspended transportation, so the scheduled patients could not move and reach the hospital and remained stuck in their places. In addition to the synchronization of Eid al-Fitr and Eid al-Adha, where most people stay with their families and celebrate. Regrettably, two patients who had been questioned had died.
Variables of the Study
- Dependent Variables Catastrophic expenditure (CE): • Out-of-pocket expenditure: by measuring hospitalization (inpatient), health care provider visits (outpatient), medications and laboratory services. • Capacity to pay (CTP).
- Independent variables a) Socio-demographic variables: • Age. • Number of children.
Employment status. Educational level.
- Income Marital status.
- Household head sex. b) Health status variables:
- Duration of disease (time since diagnosis).
- Co-morbid diseases.
- Modality of treatment (radiotherapy, chemotherapy, combination). c) Insurance status. d) Coping mechanisms.
All variables related to expenditure were converted to a monthly figure, while study data were provided in other units (i.e. when the recall period is days, weeks, six months, or one year, the data were adjusted to monthly figures).
Direct health care costs include laboratory investigations, medications, outpatient visits, emergency department and hospital visit costs, and nursing and hospital care.
Indirect costs, including earnings lost owing to travel and transports and changes in diet due to illness.
Putting in mind recall bias on the part of the respondents, and in an attempt to avoid the typical problem of underestimation of household expenditure, the inquiry about expenditure was broken down into monthly expenditure and annual expenditure information on (durable goods or large items) and daily base expenditure such as food and children pocket money.
CHE was estimated using the 40% threshold methodology that has been used by the World Health Organization.
Information on the procedures and treatments (chemotherapy, radiation, surgery) was calculated for each patient to estimate how much they spent throughout the treatment period. The household income was calculated by summation of salaries of all working household members in addition to any regular income from additional resources. The household expenditure on basic life expenses was calculated by adding expenditure on food and housing (rent, cost of water supply and cost of electricity).
In the present study, out-of-pocket expenditure (OPE) was defined as the sum total of all expenditures excluding any reimbursements. CHE was defined as breast cancer- related expenditures exceeding 40% of a household’s capacity to pay (CTP).
Capacity to pay refers to the non-subsistence expenditure which is the difference between the total household expenditure (THHE) and their subsistence expenditure (SE).
The catastrophic health expenditure was calculated as follows: Step 1: Calculation of subsistence expenditure (SE)
- Calculate food expenditure (FE)/total household expenditure (THHE). Identify the 45th - 55th percentile of FE/THHE
- SE = Mean FE of 45th - 55th of FE/THHE
Step 2: Calculation of capacity to pay (CTP)
- CTP = THHE – SE (if FE > SE)
- CTP = THHE – FE (if FE< SE) Step 3: Calculation of catastrophic health expenditure (CHE)
- CHE is present if out-of-pocket expenditure (OPE) is more than 40% of a household’s capacity to pay.
Socioeconomic status (SES) was based on tertiles of THHE; households were categorized into three SES groups: low, middle and high-income groups at the time of analysis.
Data Analysis
Questionnaires were checked for completion on a daily basis. Following data collection, the master sheet was constructed. The CHE was estimated for the patients who received treatment at RICK in a specified period. The CHE was calculated using the capacity to pay approach recommended by WHO. For categorical variables (such as education level, marital status, Number of children, Number of households, Household head extra job members and insurance type), the frequency and percentage were used to describe the demographic profile of the patients with breast cancer. The relationships between CHE and other variables, such as gender, age, education level, insurance status, extra job, disease course, family size, and Economic quintile, were investigated using the chi-squared test, which applied to examine the associations between CHE and other variables. The statistically significant variables were then entered into the multivariate logistic regression. P < 0.05 was considered statistically significant, to assess what household Variable Non- catastrophic catastrophic Who take care of financing characteristics are associated with the probability of incurring catastrophic expenditures The explanatory variables of the model include a set of characteristics including head of the household (HH) age, gender, occupation, education and presence of extra job, household size, health insurance, expenditure in quintiles, to determine the significant predictors of CHE, all analyses were performed in SPSS 20 Ethical considerations were considered through official approval from the Sudan Medical Specialization Board (SMSB) and the Khartoum State Ministry of Health (FMOH). Each patient was enlightened about the purpose and nature of this economic study, and consent was obtained. The confidentiality of the data was ensured, and access to personal data within data sets was restricted to the investigator and not disclosed. The culture of informants was respected throughout the data collection process.
Results
Regarding the distribution of the study sample according to State and residence and its correlation with catastrophic health, most of the households faced with CHE (32.6%) live in Khartoum state, followed by Kordofan’s states (12.6%), there is no significant relation with State and in general this may reflect the distribution of population in general as the Khartoum is the most populated State. It may reflect the accessibility issue for treatment in other states. CHE is observed more among households living in urban areas, about three times more than in rural areas.
Catastrophic health expenditure total P value *P=0.05
Patient’s father Count 2 9 11
% CHE 5.70% 6.70% 6.50%
Patient’s sister Count 0 4 4
% CHE 0.00% 3.00% 2.40%
Patient’s sun Count 3 12 15
% CHE 8.60% 8.90% 8.80%
0.502 Patient’s brother Count 1 17 18
% CHE 2.90% 12.60% 10.60%
Patient’s Husband Count 26 84 110
% CHE 74.30% 62.20% 64.70%
Patient’s Count 3 9 12
% CHE 8.60% 6.70% 7.10%
| Patient’s age Mean -44.8471 Median -45.0000 | % CHE | 0.00% | 12.60% | 10.00% | 0.103 | |
|---|---|---|---|---|---|---|
| 35-44 | Count | 16 | 50 | 66 | ||
| % CHE | 45.70% | 37.00% | 38.80% | |||
| 45-54 | Count | 11 | 50 | 61 | ||
| % CHE | 31.40% | 37.00% | 35.90% | |||
| 55-64 | Count | 5 | 14 | 19 | ||
| % CHE | 14.30% | 10.40% | 11.20% | |||
| 65 | Count | 3 | 4 | 7 | ||
| Household’s age Mean -49.2235 Median -49.0000 | % CHE | 8.60% | 3.00% | 4.10% | ||
| 24-34 | Count | 0 | 5 | 5 | 0.098 | |
| % CHE | 0.00% | 3.70% | 2.90% | |||
| 35-44 | Count | 2 | 23 | 25 | ||
| % CHE | 5.70% | 17.00% | 14.70% | |||
| 45-54 | Count | 17 | 39 | 56 | ||
| % CHE | 48.60% | 28.90% | 32.90% | |||
| 55-64 | Count | 7 | 38 | 45 | ||
| % CHE | 20.00% | 28.10% | 26.50% | |||
| 65 | Count | 9 | 30 | 39 | ||
| % CHE | 25.70% | 22.20% | 22.90% |
Table 1: a) Frequency table of the socio-demographic characteristic and its correlation with the catastrophic health expenditure
Table (1a) shows that CHE is observed most commonly when the patient’s husband is in charge of financial management (62.2%), while the least CHE was seen when the patient’s sister is responsible for financing. CHE records are high in the age groups 35-44 and 45-64, which record a percentage of 37% per each. The last CHE was seen in the age group above 65 years old (10.4%). Speaking about household age, most CHE were seen at age 55-65 (28.9%), while the least was observed at 24-34 and 35-44 years.
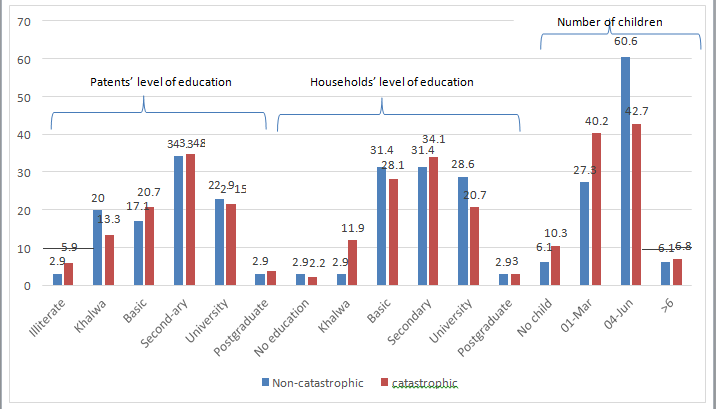
- High CHE is associated with secondary school education in patients and households: 34.8% and 34.1%, respectively.
- Number of children associated with high CHE when there are more than four sons or daughters. No significant relation exists for Patients’ level of education and Households’ level of education.
- Variable
- Catastrophic health expenditure total
- P value
- Non-catastrophic catastrophic
- *P=0.05
- 1-5
- Count
- 12
- 62
- 74
- % CHE
- 35.3%
- 48.8%
- 46.0%
- 6-10
- Count
- 22
- 62
- 84
- Number of household members
- % CHE
- 64.7%
- 48.8%
- 52.2%
- 0.205
- >10
- Count
- 0
- 3
- 3
- % CHE
- 0.0%
- 2.4%
- 1.9%
- Other
- % CHE
- 1
- 7
- 8
- Count
- 2.9%
- 5.2%
- 4.7%
- House wife
- % CHE
- 24
- 97
- 121
- Count
- 68.6%
- 71.9%
- 71.2%
- The occupation status
- Retired
- % CHE
- 2
- 2
- 4
- 0.475
- Count
- 5.7%
- 1.5%
- 2.4%
- Full work
- % CHE
- 8
- 29
- 37
- Count
- 22.9%
- 21.5%
- 21.8% yes
- Count
- 28
- 113
- 141
- % CHE
- $0.0%
- 83.7%
- 82.9%
- Additional work no
- Count
- 7
- 22
- 29
- 0.604
- % CHE
- 20.0%
- 16.3%
- 17.1%
- Government
- Count
- 15
- 35
- 50
- % CHE
- 42.9%
- 25.9%
- 29.4%
- Private
- Count
- 19
- 94
- 113
- 0.145
- Head of household occupation
- % CHE
- 54.3%
- 69.6%
- 66.5%
- Both
- Count
- 1
- 6
- 7
- % CHE
- 2.9%
- 4.4%
- 4.1% yes
- Count
- 14
- 30
- 44
- % CHE
- 40.0%
- 22.2%
- 25.9%
- .030
- Household head extra job
- No
- Count
- 21
- 105
- 126
- % CHE
- 60.0%
- 77.8%
- 74.1%
Table 2: b) Frequency table of the socio-demographic characteristic and its correlation with the catastrophic health expenditure
CHE is higher in households with less than ten members (48.8%), while it declines dramatically when they exceed t 10 members. On the other hand, CHE is higher when the household head has additional work (p<0.05). A high remark was also made on those who work in the private sector (Almost 70%).
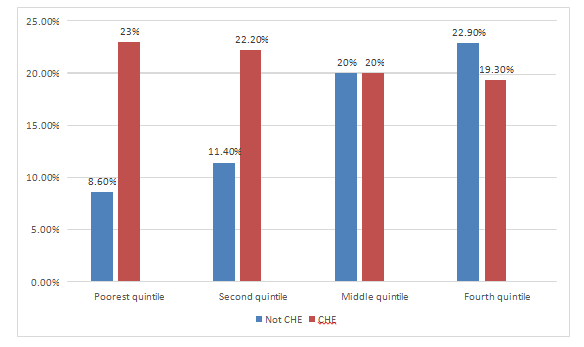
Figure (2) It is apparent that there is a strong association between being in the poorest quintile and the CHE, which is statistically significant (p<0.05), followed by the second quintile, those in the richest quintiles still lower than poor quintiles but not scoring big different.
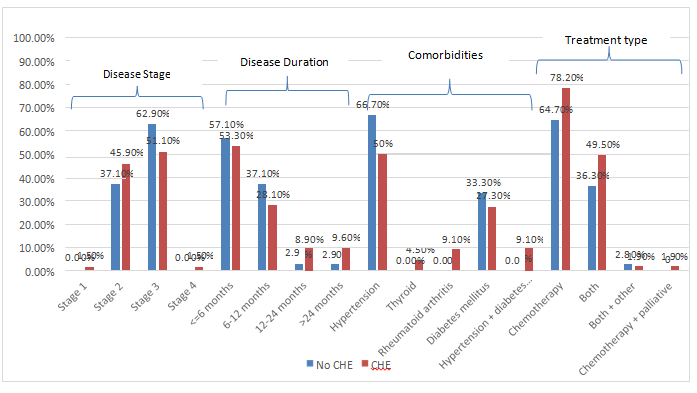
CHE is higher among patients in stages II and III, scoring 45.9% and 51.5%, respectively. CHE is high among patients who had treatment less than six months, almost half the cases. Comorbidities associated with cancer are many, but hypertension scores 50% of cases. None of the variables in this figure show a significant P value.
| Variable Non- Catastrophic Catastrophic | Catastrophic Health Expenditure | Total | P value | |||
|---|---|---|---|---|---|---|
| *P=0.05 | ||||||
| Health insurance | yes | Count | 30 | 74 | 104 | 0 |
| % CHE | 85.7% | 54.80% | 61.20% | |||
| no | Count | 5 | 61 | 66 | ||
| % CHE | ||||||
| 14.30% | 45.2 | 38.80% | ||||
| Insurance company | National Fund Health Insurance | Count | 15 | 23 | 38 | 0.271 |
| % CHE | 50.00% | 31.10% | 36.50% | |||
| State Fund for Health Insurance | Count | 12 | 41 | 53 | ||
| % CHE | 40.00% | 55.40% | 51.00% | |||
| Other insurance companies | Count | 3 | 8 | 11 | ||
| % CHE | 10.00% | 10.80% | 10.60% | |||
| Other | Count | 0 | 2 | 2 | ||
| % CHE | 0.00% | 2.70% | 1.90% | |||
| Total household expenditure & and health insurance | Poorest | Count | 19 | 15 | 34 | 0.178 |
| % CHE | 18.30% | 22.70% | 20.00% | |||
| Second | Count | 23 | 11 | 34 | ||
| % CHE | 22.10% | 16.70% | 20.00% | |||
| Middle | Count | 18 | 16 | 34 | ||
| % CHE | 17.30% | 24.20% | 20.00% | |||
| Fourth | Count | 18 | 16 | 34 | ||
| % CHE | 17.30% | 24.20% | 20.00% | |||
| Richest | Count | 26 | 8 | 34 | ||
| % CHE | 25.00% | 12.10% | 20.00% | |||
| Are you a participant or beneficiary | Beneficiary | Count | 28 | 65 | 93 | 0.331 |
| % CHE | 30.1 | 69.89 | 89.4 | |||
| participant | Count | 2 | 9 | 11 | ||
| % CHE | 18.1 | 81.8 | 10.5 |
Table 3: Frequency table of health insurance and its correlation with catastrophic health expenditure (n =170).
CHE and health insurance: More than half of insured patients are still faced with catastrophic health expenditure (54.8%); with different insurance companies, 55% of people with state government health insurance develop CHE. Insurance is highly significant and reflects a strong association.
| Variable Non- Catastrophic Catastrophic | Catastrophic Health Expenditure | Total | P val | |||
|---|---|---|---|---|---|---|
| *P=0.05 | ||||||
| Coping | yes | Count | 2 | 8 | 10 | |
| % CHE | 5.70% | 5.90% | 5.90% | |||
| no | Count | 33 | 127 | 160 | ||
| % CHE | 94.30% | 94.10% | 94.10% | |||
| Coping mechanism | Borrowing | Count | 5 | 33 | 38 | |
| % CHE | 15.20% | 26% | 23.80% | |||
| Selling of land | Count | 1 | 7 | 8 | ||
| % CHE | 3% | 5.50% | 5% | |||
| Selling of other property | Count | 15 | 42 | 57 | ||
| % CHE | 45.50% | 33.10% | 35.60% | |||
| Reduction of expenditure | Count | 1 | 9 | 10 | ||
| % CHE | 3% | 7.10% | 6.30% | |||
| Relying on Zakat | Count | 0 | 2 | 2 | ||
| % CHE | 0% | 1.60% | 1.30% | |||
| Leaving school (one of the sons) | Count | 0 | 1 | 1 | ||
| % CHE | 0% | 0.80% | 0.60% | |||
| Not applicable | Count | 5 | 11 | 16 | ||
| % CHE | 15.20% | 8.70% | 10% | |||
| Selling of other property borrowing | Count | 3 | 12 | 15 | ||
| % CHE | 9.10% | 9.40% | 9.40% | |||
| Other | Count | 3 | 10 | 13 | ||
| % CHE | 9.10% | 7.90% | 8.10% |
Table 4: Frequency table of coping mechanism and its correlation with catastrophic healthexpenditure (n =170).
CHE and coping mechanisms: The majority of patients who are not insured have the highest CHE scores (94%); there are several coping mechanisms like borrowing and selling. But most of the procedures are borrowings, and the least is Zakat.
| Variable | Frequency | Percent % | |
|---|---|---|---|
| Had you ever reduced the other expenditure due to the treatment | Yes | 82 | 48.2 |
| No | 88 | 51.8 | |
| Do you have enough money for treatment | Yes | 25 | 14.7 |
| No | 145 | 85.3 | |
| Have you ever forgot treatment due to money shortage | Yes | 82 | 48.2 |
| No | 88 | 51.8 |
Table 5: Direct and Indirect Medical Expenditure.
Family 114 67.1
Neighbors 15 8.8
- from where you get it
- Have you ever been able to return the money borrowed
- Yes
- 107
- 62.9
- If yes
- All
- 27
- 25.23
Table 6: frequency table of coping mechanism (n =170).
This table shows the different strategies for coping and financial difficulties encountered during cancer treatment. How do they deal with loans, if there are any?
| Variable | Mean | N | Std. Deviation Mean | Std. Error | |
|---|---|---|---|---|---|
| Total medical expenditure | 4555.9529 | 170 | 7666.15187 | 587.967 | |
| Pair 1 | |||||
| Medical indirect expenditure | 221.0485 | 170 | 225.5597 | 17.29964 |
Table 7: Direct and Indirect Medical Expenditure.
Paired Sample Statistics.
| Variable | N | Correlation | Sig. | |
|---|---|---|---|---|
| Pair 1 | Total medical expenditure & medical indirect total expenditure | 170 | 0.038 | 0.63 |
Table 8: Logistic regression of correlation between different variables and catastrophic health expenditure.
| Total Household Expenditure | |||||
|---|---|---|---|---|---|
| N | Minimum | Maximum | Mean | Std. | |
| Deviation | |||||
| THE Valid N (list wise) | 170 | 715 | 8482.66 | 2355.434 | 1129.23431 |
Table 9: Logistic regression of correlation between different variables and catastrophic health expenditure.
Paired Sample Correlation.
This is another frequency table showing the basic descriptive statistics and the measurement of the central tendency. (Mean of the total medical expenditure direct and indirect and the total household expenditure) Variable B S.E. Wald df Sig. Exp(B) 95% C.I.for EXP(B) PAtient_Age1 -0.26 0.44 0.357 1 0.55 0.771 0.329 1.809 HH_Occupation 0.136 0.48 0.08 1 0.78 1.146 0.447 2.936 HH. education -0.47 0.5 0.898 1 0.34 0.624 0.235 1.655 Lower Upper Sex_HH -0.04 0.77 0.002 1 0.96 0.964 0.214 4.348 Area 0.052 0.48 0.011 1 0.92 1.053 0.408 2.718
| Number_HHmember | -0.27 | 0.45 | 0.373 | 1 | 0.54 | 0.76 | 0.316 | 1.831 |
|---|---|---|---|---|---|---|---|---|
| Extra work | 0.97 | 0.48 | 4.14 | 1 | 0.04 | 2.638 | 1.036 | 6.717 |
| Health insurance | -1.94 | 0.59 | 10.64 | 1 | 0 | 0.144 | 0.045 | 0.461 |
| cooping | -0.02 | 0.95 | 0.001 | 1 | 0.98 | 0.976 | 0.153 | 6.243 |
| Expenditure quantile | 8.744 | 4 | 0.07 | |||||
| Expenditure quantile (1) | 1.95 | 0.79 | 6.131 | 1 | 0.01 | 7.029 | 1.502 | 32.9 |
| Expenditure quantile (2) | 1.629 | 0.73 | 5.005 | 1 | 0.03 | 5.097 | 1.224 | 21.232 |
| Expenditure quantile (3) | 0.674 | 0.62 | 1.167 | 1 | 0.28 | 1.963 | 0.577 | 6.672 |
| Expenditure quantile (4) | 0.384 | 0.6 | 0.404 | 1 | 0.53 | 1.468 | 0.449 | 4.795 |
| Constant | 1.723 | 1.19 | 2.082 | 1 | 0.15 | 5.6 |
Table 10: Logistic regression of correlation between different variables and catastrophic health expenditure.
95%
- Variable
- B
- S.E.
- Wald df
- Sig.
- Exp(B)
- Extra work
- 0.982
- 0.45
- 4.759
- 1
- 0.03
- 2.67
- 1.105
- 6.454
- Health insurance
- -1.702
- 0.54
- 9.895
- 1
- 0
- 0.182
- 0.063
- 0.527
- Expenditure quantile
- 8.34
- 4
- 0.08
- Expenditure quantile (1)
- 1.764
- 0.73
- 5.81
- 1
- 0.02
- 5.835
- 1.39
- 24.486
- Expenditure quantile (2)
- 1.355
- 0.66
- 4.173
- 1
- 0.04
- 3.876
- 1.056
- 14.222
- Expenditure quantile (3)
- 0.505
- 0.59
- 0.741
- 1
- 0.39
- 1.657
- 0.525
- 5.227
- Expenditure quantile (4)
- 0.326
- 0.58
- 0.318
- 1
- 0.57
- 1.386
- 0.446
- 4.305
- Constant
- 1.227
- 0.63
- 3.824
- 1
- 0.05
- 3.411
Table 11: Logistic regression of correlation between different variables and catastrophic health expenditure.
This table 6 predicts the association between catastrophic health expenditure and different variables; the result shows a strong association between catastrophic health expenditure and insurance, extra jobs, and different quantiles of social class. The second table shows the model, which also includes these three variables.
Discussion
This cross-sectional study was investigated the OOP payments, catastrophic health expenditure attributed to breast cancer in Sudan, based on the WHO suggestions, 40% of capacity to pay (CTP) was chosen to calculate the catastrophic health expenditure (CHE) [14] there were 135 patients (79.4%) out of 170 households with breast cancer patients who attend the outpatient at the RICK faced catastrophic health expenditures. The incidence of CHE in our study was higher than in the Chinese study as they record 66.82% CHE among breast cancer patients [29] and 13.7% of the Iranian households with breast cancer patients [32], which is less than what was found in an Indian study where the CHE of breast cancer was estimated at 84.2% [30].
There is no known previous estimate of overall catastrophic expenditure in Sudan, but there are two studies that are concerned with catastrophic expenditure in specific diseases; one inspects the economic burden of AIDS/HIV. It was found that CHE among HIV/AIDS patients is equal to 55.7% [41]. However, the treatment is provided free to all HIV patients. The other study was conducted in the Red Sea [42], and it found that CHE incidence among visceral leishmaniosis patients (VL) is more than 75%. The latter result is closer to the current research’s result. The lack of national incidence of CHE makes it challenging to say if the existing figure is acceptable compared to other diseases since the government allocates a high proportion of funds to cancer treatment free-of-charge policy.
A free-of-charge policy for breast cancer treatment was implemented in 2007. However, patients must pay some user fees (e.g. chemotherapy of 15 doses for 350 SDG, doctor fee of 3 SDG, chemotherapy 11 SDG for each dose and others). Some researchers claimed that abolishing user fees would lead to greater access for the poor and reduce the risks of catastrophic health expenditures. Another survey found that it does not decrease catastrophic expenditure among the poor, although it increases the utilization rate [28]; the Radiation and Isotopes Center in Khartoum (RICK) and the National Cancer Institute (NCI) in Wad Madani provide radiotherapy and chemotherapy treatments. The RICK is the referential institute in Sudan. It hosts more than 80% of breast cases (1303) in comparison to just 141 cases in NCI during the year 2013, and 1242, 1063, and 1072 for 2012, 2011, and 2010 consequentially in comparison with 280,249 and 177 in NCI, in addition, it offers treatment at the minimal cost so it is deemed affordable to poor patients and provides chemotherapy and radiotherapy free of charge.
One hundred and seventy patients participated in this study, representing 15 out of Sudan’s 18 states; this reflects the heterogeneous sample and allowed for the inspection of different economic strata. Most of the patients were from Khartoum (the Capital), which accounts for 35.88%, which shows the highest incidence of CHE (32.6%); this raises the question about the accessibility to treatment , considering that there are limited numbers of treatment centers (RICK in Khartoum, NCI in Wad Madani and Shandi Oncology Center; the latter has no radiotherapy department), so there are few choices for patients; this also had a high transportation cost for patients who live in the other states in a sprawling country, that explains the high indirect medical cost. Most patients reside in urban areas (72%), and most CHE are found in urban areas (71.1%); this aligns with studies in Iran and Nigeria [3, 43] unlike what found in Turkey, Serbia and another study in Iran, in which the CHE is more in the rural area [44, 45]. The odd ratio for the distribution of patients according to the area is not significant: 1.053 (95% CI= 0.408- 2.718). Differences might be a result of the lower capacity of rural residents to meet costs, seeking behavior and accessibility to the facility.
The household head sex shows no significant relationship, although the percentage incurs CHE 75% when the household is female. An interesting finding in Indian rural areas shows that female-headed households have 2% lower probability of experiencing financial catastrophe than households with male head [46]. However, a significant correlation was observed between the two variables in the study performed in the 17th district of Tehran [3, 47], and many studies stated that male-headed households are not a protective factor against CHE. The sex of the household head is not a determinant of catastrophic expenditure [3]. The majority of respondents were in the productive ages of 35-44 years (38.8%) and 45 – 54 years (35.9%); this finding is consistent with studies in the previous year yield the same affected age group [48]. and [49, 50, 51]. Moreover, age > 40 years is a determinant of CHE; this is in agreement with many previous searches [43, 52, 53, 54]. The highest incidence of CHE was found in the age group 45-54 years and 45-54 years, which scored 37%. The mean age of the patient is 44.85, and the median is 45. But the result shows no significant relationship.
Regarding household heads, most of them were at the age of 40-49(32.9%), the mean is 49.2, and the median is 49. Most of the CHE were found at 45-54 years (28.9%) and 55- 64 years 28.1%). There is a weak association between age and catastrophic health expenditure reflected by the small odds (OR: 0.771, 95% CI= 0.329-1/809). Education and health are the two most important characteristics of human Capital. The close relationship between education and health was documented by many authors [55].
Education may contribute to CHE by different means. Educated people are more likely to take care of their health, thus reducing OOP health expenditure. On the other hand, educated people have a better chance of having a good income and a fixed job (55). As mentioned in the previous study, education is an indicator of income, then with an increase in education probability of catastrophic OOP health expenditure goes down [46, 56]; In this study the relation between CHE and education not significant and it does not protect rich households from catastrophic payments [14, 41]. although it has an appositive relation with economic status (P=0.02). This is not inconsistent with Cheng-yao study in China where the education has an impact on CHE [29]. Most of the heads of households working in the private sector have catastrophic health expenditure (69.6%), with OR=1.146 (95% CI=0.447-2.936). On the other hand, there is an association between the type of occupation and the economic status (P=0.02). There is a great percentage of households’ heads who don’t have extra jobs suffer from catastrophic health expenditure (77.8%), which is statistically significant (p<0.01), OR: 2.638 (95% CI= 1.036-6.717). Based on the results, most of the patients who have catastrophic health expenditure are in grade III of breast cancer (51.1%) with no statistical significance; most of the treatment carried out is chemotherapy (60%).
This finding is supported by CHE estimated in Shiraz Hospital, Iran. Patients showing a disease duration of less than six months have the greatest incidence of CHE
(53.3%); this is inconsistent with many previous studies since the treatment will be different and more complicated with advanced disease [25] [29]. There are other diseases associated with breast cancer, like hypertension, thyroid, diabetes mellitus, rheumatoid arthritis and irritable bowel syndrome. Hypertension was reported as the most common among those patients who suffered catastrophic health expenditure (40.9%), as the same finding of many studies [14, 57, 58, 59].
Family size didn’t show a significant relation with CHE (OR=0.076, CI=0.31-1.8), which was in the same line with the Iranian study [3]. Thailand is not consistent with other findings from many countries [56]; another study in Egypt expresses the large family size as a protective factor against CHE [41]. Those who have 4-6 children account for 52%, while those who have 1-3 children account for 41%. Households composed of 1-5 and 6-10 members showed the highest incidence of CHE, 48.8% per each; this is less than what was found in one study [3], in agreement with other studies [1, 59], and in disagreement with this study [60]. The weak association between family members’ count and catastrophic health expenditure is reflected by the low odds (OR: 0.760, 95% CI= 0.316-1.831. The economic status in the present study shows statistical significance (P=0.025) and is associated logically throughout different quartiles, expressing a negative relationship; the finding is also supported by the logistic regression with OR of 0.013 for the poorest quantile and clear enhancement of this factor in the model also exist, which make it clear that its strongest variable predicts the CHE under this study, this is not coherent with finding in Shiraz hospital [3] Another study in Iran states that households with higher SES levels are less likely to incur CHE, but a significant fraction of all SES subgroups are exposed to these catastrophic costs [32], a considerable previous research support this relationship [46, 60, 56].
There is a statistically significant effect of the economic status upon the catastrophic health expenditure in the first quintile (p<0.05) and high OR: 7.029 (95% CI=1.502), and the second quintile (p<0.05) and high OR: 5.097 (95% CI=1.224-21.232), the other quintile has an effect but not that significant.
There were many strategies for coping, but catastrophic health was seen most commonly in households that sold other properties (33.1%), which is the most frequent coping strategy in Iran [32]. They share many coping strategies in South Africa, including reduced expenditure on clothing and food, use of savings, borrowing money, and taking on extra work [61]. On the other hand, the majority of patients who had coped have CHE (94.1%), which means coping was not effective in preventing catastrophic health expenditure. The OR of coping was 0.976 (95% CI=0.153- 6.243). Most of the patients received external financial support (75.3%), and most of this support came from the family (97. 66%). The majority of patients have financial support because of their illness (98%), and most of them (85%) said that they didn’t get help regularly. The majority of patients borrowed money from their families (67.1%).
Sixty-three per cent of patients said that they returned borrowed money, and among those who returned the money, the majority (75%) didn’t return it completely; this is consistent with Iranian and Cambodian studies, they have spent a large part of their meagre income on buying the needed services, and for this purpose, most of them have been forced to sell their assets, borrow, or take a bank loan [34, 32]. This may predict future liability to more catastrophic expenditure. A logistic regression model was implemented. It was assumed that there are some features that had an impact and effect upon that household faced catastrophic health expenditure, like socio-demographic characteristics, breast cancer treatment, insurance and economic status.
The model revealed that those households who had an extra job and were in the first quintile had a statistically significant relationship with catastrophic health expenditure (p<0.05) with strong OR: 5.836 (95% CI=1.390-24/486) and those who had an extra job and were in the second quintile had a statistically significant relationship with catastrophic health expenditure (p<0.05) with OR: 3.876 (95% CI=1.056- 14.222). Interestingly, to find that having extra jobs has positive productivity to catastrophic healthcare expenditure, those who tend to achieve extra jobs might face high expenditure even before the disease occurs, or it may be a part of a coping strategy. The logistic regression shows that health insurance has a significant relation with CHE (p<0.05), with a negative B value, meaning health insurance is a protective factor against CHE; this sounds logical and consistent with many previous studies [3, 29] [61, 62, 63].
Conclusion
The study, at a glance, reviews the evidence on financial fairness as a major goal of the health system and a core jargon in equity, explores the different mechanisms of financing the health systems and discusses the lack of policy to guard against bankruptcy due to health expenditure which required an evidence base recommendation and solution. OOP health expenditure for breast cancer patients was shown to be financially catastrophic for most households in this study and difference tools of coping mechanism was explored to substantial out-of-pocket expenditures to save lovely mothers and daughters.
Also, Policies targeted at minimizing CHE can address aspects connected to healthcare outcomes in the families of patients with severe diseases like breast cancer. It has been demonstrated that certain socioeconomic and non- socioeconomic factors strongly affect CHE in the examined households, and since the socioeconomic factor are not easily changeable, the modification should target the nonsocial aspect such as health insurance and social support to those who are more liable to develop CHE.
The economic analysis reveals that all households at different expenditure quintiles are exposed to catastrophic health expenditure to various degrees, and the poorest are the most at-risk group. The study also demonstrates the crucial role of health insurance in decreasing catastrophic healthcare expenditures.
Recommendations
The pattern of out of pocket among households with breast cancer shows that catastrophic healthcare expenditure coincides with both the health reform and poverty alleviation goals, so we recommend that:
- Identifying the at-risk subgroups for catastrophic and impoverishing payments and identifying these risk sources can be critical in effective policy-making to reduce these indicators
- Improve and expand current insurance coverage to be more effective against catastrophic healthcare expenditure; and make special consideration with poor households since they are more liable to develop catastrophic health expenditure
- Integrate indicator of financial fairness as core indicator in the existing health information system and guarantee accurate data sources in terms to assess the performance of the health system. With this high rate of CHE, further study to evaluate the impoverishment effect needed as a major contributing issue with SDG1
- Modify the healthcare delivery system to reduce the economic burden of cancer health, especially in the poorest households (Affordable user fees) Future research to assess the possibility of untraditional health financing mechanisms, health policy to make use of social responsibility and involvement of other stakeholder, NGOs responsibility to support especially the indirect medical expenditure
- Orient breast cancer females and their households by the cost of treatment and its peak in the first six months, providing them a better chance to develop coping plans regarding expenditure according to different treatment faces.
Limitations of the Study
As with any cross-sectional study, there was a probability of recall bias. Thus, it is not excluded that patients forgot, underestimated, or overestimated some of the information asked. To overcome such bias, research questions were carefully selected, and appropriate data collection methods were used. All respondents were interviewed while they received treatment or came for follow-up, meaning nearby expenditure information.
Although the study is hospital-based, it is believed the result can be generalized as there are only two major public cancer centers in Sudan, the Radiation and Isotope Centre (RICK) and the National Cancer Institute of the University of Gezira (NCI -UG), with 80% of cases covered by RICK. Breast cancer is the most frequently seen malignancy at both centers. And people come from all states to receive treatment in this referral center.
The study demonstrates the current CHE and ignore long term implication of the out-of-pocket payment and especially if the disease metastasized and require intensive treatment.
Further research is recommended to monitor these findings and discuss the limitations encountered in this study. As well as an assessment of Overall CHE at the country level.
References
-
Ke Xu (2005) Distribution of health payments and catastrophic expenditures Methodology. World Health Organization.
-
Braveman P, Gruskin S (2003) Defining equity in health. J Epidemiol Community Health 57(4): 254-258.
-
Kavosi Z, Keshtkaran A, Hayati R , Ravangard R, Khammarnia M (2014) Household financial contribution to the health System in Shiraz, Iran in 2012. Int J Health Policy Manag 3(5): 243-249.
-
Collins C, Green A, Hunter D (1999) Health sector reform and the interpretation of policy context. Health Policy 47(1): 69-83.
-
Maynard A, Bloor K (1995) Health care reform: informing difficult choices. Int J Health Plann Manage 10(4): 247- 264.
-
Christopher J, Murray L, Xu K, et al. (2003) Assessing the Distribution of Household Financial Contributions to the Health System: Concepts and Empirical Application. World Health Organization.
-
Smith RA, Caleffi M, Albert U-S, Chen THH, Duffy SW, et al. (2006) Breast cancer in limited-resource countries: early detection and access to care. Breast Journal 1: 16- 26.
-
Xu K, Evans DB, Carrin G, Aguilar-Rivera AM, Musgrove P, et al. (2007) Protecting households from catastrophic health spending. Health Aff (Millwood) 26(4): 972-983.
-
Boyle P, Levin B (2008) World Cancer Report 2008. WHO.
-
Christopher J, Murray L, Evans DB (2003) Health systems performance assessment: debates, methods and empiricism. World Health Organization, Economic Evaluation and Analysis (EEA), pp: 927.
-
Berki S E (1986) A look at catastrophic medical expenses and the poor. Health Aff (Millwood) 5(4): 138-145.
-
Russell S (2004) The Economic Burden of Illness for Households in Developing Countries: A Review of Studies Focusing on Malaria, Tuberculosis, and Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome. American Society of Tropical Medicine and Hygiene 71(2): 147-155.
-
Wyszewianski L (1986) Financially catastrophic and high-cost cases: definitions, distinctions, and their implications for policy formulation. Inquiry 23(4): 382- 394.
-
Xu K, Evans DB, Kawabata K, Zeramdini R, Klavus J, et al. (2003) Household catastrophic health expenditure: a multicountry analysis. Lancet 362(9378): 111-117.
-
Wagstaff A, Doorslaer EV (2003) Catastrophe and impoverishment in paying for health care: with applications to Vietnam 1993-1998. Equity in Health Care 12(11): 921-933.
-
Wagstaff A, Bilger M, Sajaia Z, Lokshin M (2011) Health equity and financial protection. World Bank, pp: 1-196.
-
Merlis M (2002) Family Out-of-Pocket Spending for Health Services: A Continuing Source of Financial Insecurity. The common wealth fund, pp: 1-48.
-
Waters HR, Anderson GF, Mays J (2004) Measuring financial protection in health in the United States. Health Policy 69(3): 339-349.
-
(2010) The Global Economic Cost of Cancer. American Cancer Socity.
-
Berkman BJ, Sampson SE (1993) Psychosocial effects of cancer economics on patients and their families. Cancer 72(9): 2846-2849.
-
Gordon L, Scuffham P, Hayes S, Newman B (2007) Exploring the economic impact of breast cancers during the 18 months following diagnosis. Psychooncology 16(12): 1130-1139.
-
Arndt V, Merx H, Stegmaier C, Ziegler H, Brenner H (2004) Quality of life in patients with colorectal cancer 1 year after diagnosis compared with the general population: a population-based study. J Clin Onco 22(23): 4829-4836.
-
Moore KA (1999) Breast cancer patients’ out-of-pocket expenses. Cancer Nurs 22(5): 389-396.
-
Bennett JA, Brown P, Cameron L, Whitehead LC, Porter D, et al. (2009) Changes in employment and household income during the 24 months following a cancer diagnosis. Support Care Cancer 17(18): 1057-1064.
-
Arozullah AM, Calhoun EA, Wolf M, Finley DK, Fitzner KA, et al. (2004) The financial burden of cancer: estimates from a study of insured women with breast cancer. The Journal of Supportive Oncology 2(3): 271-278.
-
Parkin DM, Bray F, Ferlay J, Pisani P (2005) Global cancer statistics, 2002. CA Cancer J Clin 55(2): 74-108.
-
Stewart BW, Kleihues P (2003) World Cancer Report. World Health Organization.
-
(2005) WHA58.33 Sustainable health financing, universal coverage and social health insurance. WHO.
-
Sun CY, Shi JF, Fu WQ, Zhang X, Liu GX (2021) Catastrophic Health Expenditure and Its Determinants among Households with Breast Cancer Patients in China: A Multicentre, Cross-Sectional Survey. Front Public Health 9: 704700.
-
Mohanty SK, Wadasadawala T, Sen S, Maiti S, Jishna E (2024) Catastrophic health expenditure and distress financing of breast cancer treatment in India: evidence from a longitudinal cohort study. International Journal for Equity in Health 23(1): 145.
-
Berlin NL, Albright BB, Moss HA, Offodile AC (2024) Catastrophic health expenditures, insurance churn, and non-employment among women with breast cancer. Cancer Spectr 8(2): pkae006.
-
Ahmadi F, Farrokh-Eslamlou H, Yusefzadeh H, Alinia C (2021) Incidence of household catastrophic and impoverishing health expenditures among patients with Breast Cancer in Iran. BMC Health Services Research 21(1): 327.
-
Emanuel EJ, Fairclough DL, Slutsman J, Alpert H D Baldwin D, et al. (1999) Assistance from Family Members, Friends, Paid Care Givers, and Volunteers in the Care of Terminally Ill Patients. N Engl J Med 341(13): 956-963.
-
Damme WV, Leemput LV, Por I, Hardeman W, Meessen B (2004) Out-of-pocket health expenditure and debt in poor households: evidence from Cambodia. Trop Med Int Health 9(2): 273-280.
-
Skarbinski J, Walker HK, Baker LC, Kobaladze A, Kirtava Z, et al. (2002) The Burden of Out-of-Pocket Payments for Health Care in Tbilisi, Republic of Georgia. JAMA 287(8): 1043-1049.
-
(2013) Sudan Interim Poverty Reduction Strategy Paper. Fund, International Monetary.
-
(2010) Country cooperation strategy for WHO and Sudan: 2008–2013. World Health Organization.
-
Ferlay J, Soerjomataram I, Ervik M, Dikshit R (2012) GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide. IARC.
-
Elhoweris M (2011) Sudan First International Conference on Breast Cancer 5th-7th December 2011, Khartoum Sudan.
-
(2012) National Cancer Strategy 2012-2016. Non communicable disease, Federaal Ministry of Health.
-
Ahmed R (2011) Catastrophic Health Expenditure and Poverty in Egypt: an Analysis of Household Survey Data.
-
Meheus F, Abuzaid AA, Baltussen R, Younis BM, Balasegaram M, et al. (2013) The Economic Burden of Visceral Leishmaniasis in Sudan: An Assessment of Provider and Household Costs. Am J Trop Med Hyg 89(6): 1146-1153.
-
Ukwaja KN, Alobu I, Abimbola S, Hopewell PC (2013) Household catastrophic payments for tuberculosis care in Nigeria: incidence, determinants, and policy implications for universal health coverage. Infect Dis Poverty 2: 21.
-
Arsenijevic J, Pavaova M, Groot W (2013) Measuring the catastrophic and impovershing effect of household health care spending in Serbia. Social science and medicine 78: 17-25.
-
Yardim MS, Cilingiroglu N, Yardim N (2010) Catastrophic health expenditure and impoverishment in Turkey. Mahmut Saadi Yardim, Nesrin Cilingiroglu. Health Policy 94(1): 26-33.
-
Pal R (2010) Analysing Catastrophic Oop Health Expenditure in India: Concepts, Determinants and Policy Implications. Indira Gandhi Institute of Development Research, India.
-
Chu TB, Liu TC, Chen CS, Tsai YW, Chiu TW (2005) Household out-of-pocket medical expenditures and national health insurance in Taiwan: income and regional inequality. BMC Health Services Research 5: 60.
-
Ageep AK (2011) Benign breast tumors in Red Sea State, Sudan. Journal of Cancer Research and Experimental Oncology 3(7): 84-87.
-
Amir H, Kitinya JN, Parkin DM (1994) A comparative study of carcinoma of the breast in an African population. East Afr Med J 71(4): 215-218.
-
Hassan I, Onukak EE, Mabogunje OA (1992) Breast cancer in Zaria, Nigeria. J R Coll Surg Edinb 37(3): 159- 161.
-
Anyanwu SN (2000) Survival following treatment of primary breast cancer in eastern Nigeria. East Afr Med J 77(10): 539-43.
-
Su TT, Kouyate B, Flessa S (2006) Catastrophic household expenditure for health care in a low-income society: a study from Nouna District, Burkina Faso. Bull World Health Organ 84(1): 21-27.
-
Anbari Z, Mohammadbeigi A, Mohammadsalehi N, Ebrazeh A (2014) Health Expenditure and Catastrophic Costs for Inpatient- and Out-patient Care in Iran. Int J Prev Med 5(8): 1023-1028.
-
Choi JW, Cho KH, Choi Y, Han KT, Kwon JA, et al. (2014) Changes in economic status of households associated with catastrophic health expenditures for cancer in South Korea. Asian Pac J Cancer Prev 15(6): 2713-2717.
-
Grossman M (1999) The Human Capital Model of the Demand for Health. Handbook of Health Economics.
-
Donnell OO, Rannan-Eliya RP, Somanathan A, Adhikari SR, Harbianto D, et al. (2005) Who benefits from public spending on health care in Asia?.
-
Jiang C, Ma J, Zhang X, Luo W (2012) Measuring financial protection for health in families with chronic conditions in Rural China. BMC Public Health 12: 988.
-
Gotsadze G, Zoidze A, Rukhadze N (2009) Household catastrophic health expenditure: evidence from Georgia and its policy implications. BMC Health Services Research 9(69).
-
Bindra EM, Andrés AR, Enemark U (2014) Correlates of out-of-pocket and catastrophic health expenditures in Tanzania: results from a national household survey. BMC Int Health Hum Rights 14(5).
-
Bhojani U, Thriveni BS, Devadasan R, Munegowda C, Devadasan N, et al. (2012) Out-of-pocket healthcare payments on chronic conditions impoverish urban poor in Bangalore, India. BMC Public Health volume 12: 990.
-
Dyer SJ, Sherwood K, McIntyre D, Ataguba JE (2013) Catastrophic payment for assisted reproduction techniques with conventional ovarian stimulation in the public health sector of South Africa: frequency and coping strategies. Hum Reprod 28(10): 2755-2764.
-
Yardim MS, Cilingiroglu, N, Yardim N (2009) Catastrophic health expenditure and impoverishment in Turkey. Health Policy 94(1): 26-33
-
Barros AJD, Bastos JL, Dâmaso AH (2011) Catastrophic spending on health care in Brazil: private health insurance does not seem to be the solution. Cad Saude Publica 27(S2): S254-S262.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda