Reactive Hypoglycaemia- A challenge for Diabetes Management!
Imagine you get a routine blood sugar test done and your post prandial blood sugar (PPBS) level is reported lower than fasting blood sugar level, contrary to the common perception of the reverse by your family physician, you and general population is reported. This rare phenomenon is called Reactive Hypoglycaemia! Reactive hypoglycaemia (RH) is a condition characterized by recurrent episodes of hypoglycaemia occurring after consumption of carbohydrate rich meals usually within four hours after meals. Type 2 diabetes (T2D) patients experience RH less frequently than type 1 diabetes (T1D) patients. Most RH episodes in T2D are mild to moderate, therefore this is noticed as surprise outcome in a routine check-up among prediabetics or early diabetics Majority of such clients are symptomless or may have Symptoms varying from almost mild or self-resolving weakness after meals to severe manifestations if BS falls below 70mg/ Dl. Severe symptoms include loss of consciousness, seizures, falls, and impaired cognition that may lead to hospitalization for emergency treatment. Managing RH poses challenges to the doctors also due to limited & often ineffective treatment options known till day. Materials and Methods: This article is an outcome of the diagnostic and management challenge the author is facing as a family physician in one case currently. 62 years old lady sought second opinion as lab report on 10 Augst 2024 reported her FBS as 136 mg/dl and PPBS 2 hrs after breakfast as 114mg/Dl in a routine check-up. Repeat test report on 15 August showed PPBS= 108mg/Dl and FBS= 146 mg/Dl and Hb1Ac =7.65 % making us to. Diagnose her as Early diabetes case. She was put on Metformin 500mg BD after main meals. Outcome: A comprehensive whole-body check-up on 5th September 2024 showed abnormal biomarkers of i) Fasting Blood Glucose level=136mg/dl, PPBS= 103 mg/Dl, and Hb1Ac=6.8%. Total Cholesterol=211mg/dl- borderline high, Transferrin saturation=15.8%, Vitamin D Total= 10.2 mg/Dl and Uric Acid=6.4 mg/dl. Two weeks of metformin had yielded some effect. Current approach adopted is to correct Vit D efficiency first and try to identify the Hypoglycaemia timings (after 4 hours of lunch) and consider giving Metformin an hour before the BS starts rising beyond 140mg/Dl. Though ideal to use the continuous Glucose monitoring tools, affordability is the constraint.
Abbreviations
FBS: Fasting Blood Sugar; PPBS: Post-prandial Blood Sugar; Hb1Ac: Glycosylated Haemoglobin; RH: Reactive hypoglycaemia.
Introduction
Reactive hypoglycaemia (RH) is a condition characterized by recurrent episodes of hypoglycaemia occurring after consumption of carbohydrate rich meals usually within four hours [1]. Type 2 diabetes patients experience hypoglycaemia less frequently than type 1 diabetes patients. Most hypoglycaemia episodes in type 2 diabetes are mild to moderate. Often this condition is noticed in a routine check- up among prediabetics or early diabetics. Symptoms of RH if any vary from almost mild and self-resolving to severe manifestations if BS falls below 70mg/Dl such as loss of consciousness, seizures, falls, and impaired cognition that may lead to frequent hospital admissions. Managing reactive hypoglycaemia (RH) poses challenges due to limited and often ineffective treatment options [1].
Adolescents, adults and senior Citizen’s’ live these days are stressful because of Scholastic demands, competitiveness and performance or getting a good job or keeping the expected performance in the jobs on hand. Almost everyone is constantly on their toes, and their health is the last thing that comes to their mind. Public health professionals estimate that about 75% of the Indian population never goes for diagnostic tests until they are sick, and their doctors advises to do so. While this negligence leads to a rising incidence of chronic health problems of diabetes, cardiovascular diseases, stress-related illnesses, etc. and in several cases, it minimizes their chances to fight it back.
Health is the greatest asset of all time and cannot be neglected for anything. However it requires regular upkeep, and that’s where the preventive health checkups are becoming a norm among educated lot. The advancement in diagnostic approaches like biomarkers in the body fluids like blood, urine, CSF etc and Imaging (Xray/scanning etc) have made it possible to detect the problem before it turns serious with the help of a full-body health checkup. It is also not uncommon that Biomarkers lead to unnecessary interventions. The issue of this article is where the outcomes of a routine lab reports are contrary to normative expectations.
The common perception both among people and some practitioners is that post- meals or post prandial blood sugar (PPBS) level must be higher than fasting blood sugar (FBS) level. In a recent case the author is challenged of managing of an elderly lady whose postprandial blood glucose (103 mg/ Dl) was remarkably lower than that of fasting level (156mg/ Dl) and it was not a lab error! as, the repeat investigation in the same lab and another lab within fortnight yielded similar results. Clinical laboratories which process many blood samples daily for estimation of FBG and PPBG level, report that in some cases (10%) that FBS may be higher than the PPBG in both diabetics and healthy population. This is known as “Reactive Hypoglycaemia” or postprandial hypoglycaemia [1, 2].
Blood glucose level as a biomarker primarily depends upon individual characters of type and quantity of food intake, physical activity and the body’s metabolic response and pre-analytical factors like smoking, caffeinated drinks, use of hypoglycaemic drugs, heavy exercise, anxiety and delay in sample processing. Careful attentions to these modifiable factors by both clinician and laboratory staff are essential to ensure accurate glucose measurement.
This article is an outcome of the diagnostic and management challenge the author is facing as a family physician in one case currently.
Case Report
Ms Veda a 62-year-old lady came to the author for a second opinion as her blood sugar lab report on 10 Augst 2024, reported a FBS of 136 mg/dl and PPBS after 2 hrs after breakfast was 114mg/Dl, a conflicting reading to the best of her and her family doctors understanding. As Hb1Ac was not done, she was advised to get it done and was done on 15 August 2024, which reported it to be 7.65 a definitive diagnostic parameter for Early diabetes. She was put on Tab. Glycomet SR (Metformin) 500 mg, after lunch and Dinner. She was also advised to take smaller frequent feeds every 3 hours and increase the quantity of proteins, vegetables especially green leafy vegetables (GLV) and fruits. Concerned with the peculiar type of diabetes the family went in for a whole-body check-up on 5 September 2024.
The results: i) Abnormal Biomarkers: Fasting Blood Glucose level=136mg/dl, PPBS= 103 mg/dl, Hb1Ac=6.8%, Total Cholesterol=211mg/dl- borderline high, Transferrin saturation=15.8%, Vitamin D Total= 10.2 mg/Dl and Uric Acid=6.4 mg/dl, ii) Normal Parameters for C reactive Protein-(0.39mg), Serum Creatinine=0.84 mg, Serum electrolytes Na=141mEq/l, K=4.32 mEq/land Chlorides108 mEq/L, Total Protein=7.26g/dl, Albumin=4.27g/ dl, Globulin=2.99g/dl, Albumin /Globulin ratio-1.43, Alkaline Phosphate=95u?l, Total Bilirubin= 0.5mg/dl, DB=0.18 mg/dl, Indirect=0.32 mg, SGOT & SGPT- 20 U/Dl each, Gamma GT=21,Total Calcium=9.4 mg/dl, Albumin= 4.27 g/, adjusted Calcium=9.19mg/dl, Iron
profile=55 mcg/dl Total Iron Binding capacity 348mcg/ dl, Unsaturated Iron Binding 293mcg/dl, Serum Ferritin Ing=243.6mg/dl, T3= 1.08 ng/dl, T4= 9.3mcg/dl, TSH=2.48mcIU/ml, Vit B12 Assay=27.9 pmol/L, Iron Profile (Ferritin)-74.48ng/dl, PPBS=103mg/Dl . All Haematological biomarkers were within normal limits, Urine examination for sp. gravity, colour, pH, protein- albumin, ketone bodies, nitrites, urobilinogen, Urine Glucose, Bilirubin negative- all were also within normal limits.
Based on the FBS and Hb1Ac level a diagnosis of early diabetes is made now by the current criteria. To manage with diet modification or begin with oral antidiabetics is a dilemma!
The patients’ dietary habits needed streamlining as her staple diet is rice and consumption of fruits, proteins and Fats fall short of requirements. However, diet management in terms of a family practice of late-night dinner (around 10 00 PM) appears to be operationally difficult immediately. Shifting low Carbohydrate, high protein and high roughage is another challenge due the perception of light food at night, which means having only rice in the night for many Indian traditional families. Current approach adopted is to correct Vit D efficiency first and meanwhile try to identify the Hyperglycaemia timings (probably after 4 hours of each main meal and consider Metformin an hour before the BS starts rising beyond 140mg/Dl. Though ideal to use the continuous Glucose monitoring tools, affordability is the constraint.
A repeat PPBS on18 September 2024 showed 173mg/Dl, that facilitating Metformin tablet after 2 hrs of main meals, advancing dinner later by 2030. A weeks of this treatment has brough down PPBS 2hrs to 102 mg/dk and after 4 hrs to 140mg/dl.
Hypoglycaemia due to Metformin Toxicity: A young lady of 25 years, known diabetic who was put on Metformin 1000 mg after all three meals. On day 3 she accidentally took all three tables of the day her husband had kept aside before going to office after lunch. After 4 hours she felt fatigued through stable. On examination she was hypotensive, and blood test showed lactic acidosis. She was managed with 50% dextrose water boluses; she took 24 hours of renal replacement therapy.
Discussion
Definition
Reactive hypoglycaemia, postprandial hypoglycaemia, or sugar crash is a term describing recurrent episodes of symptomatic hypoglycaemia occurring within four hours [1, 2] after a high carbohydrate meal in people with and without diabetes [1]. The term is not necessarily a diagnosis since it requires an evaluation to determine the cause of the hypoglycaemia. The condition is related to homeostatic systems to control the blood sugar level. It is described as a sense of tiredness, lethargy, irritation, or hangover, although the effects can be lessened if a lot of physical activity is undertaken in the first few hours after food consumption.
Causes of Hypoglycaemia
RH can occur in patients with insulin resistance and mild type 2 diabetes [3]. One of the early changes with the onset of type 2 diabetes is a decrease in first-phase insulin release leading to postprandial hyperglycaemia. This is followed by an exaggerated second phase insulin release and subsequent hypoglycaemia [4]. Idiopathic RH or functional post- prandial hypoglycaemia, where the cause remains unclear or unknown [5]. RH is an increasingly recognized and disabling complication of upper gastrointestinal (GI) surgery affecting 10-30% of patients. The condition is believed to result from accelerated gastric emptying causing hyperglycaemic peaks and excessive release of the incretin hormones, GLP-1 and GIP, resulting in hyperinsulinemia [6].
One need to remind the patient and the population in general the fact that the organ that is responsible for fasting value of blood glucose is liver, whereas it is the pancreas that is responsible for PPBG value. Several hours after dinner, blood glucose level drops leading to decrease in production & insulin level and rise in glucagon level. Glucagon is responsible for maintaining adequate blood glucose level in fasting condition via activation of metabolic pathways like gluconeogenesis and glycogenolysis in liver. Higher FBG level is due to increase in glucagon to insulin ratio as seen in diabetes, where liver is involved in excess glycogen breakdown and gluconeogenesis. Despite having sufficient insulin, individual may have higher FBG value due to insulin resistance causing impaired fasting glucose tolerance and diabetes mellitus. Higher FBG is mainly due to high carbohydrate meal at bedtime or not taking enough diabetic medication. The anxiety in an individual with disturbed sleep may also cause high FBG. The lesser-known entities like Dawn phenomenon and Somogyi effect (Figure 1) also contribute to higher FBG in the morning. These are the body’s response to hypoglycaemia by release of counter regulatory hormones like glucagon, epinephrine and cortisol which can be treated by altering type and time of meal and medication [2, 4, 5].
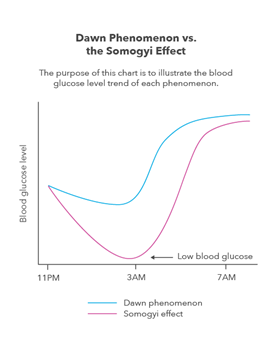
The dawn phenomenon is an early-morning rise in blood sugar, in people with diabetes. It is a common cause of high blood sugar in the morning for people with diabetes. Human body naturally produces hormones in the early morning that signal the liver to increase glucose production, which provides energy to help us to wake up. However, among diabetics their pancreas may not produce enough insulin to respond to the rise in blood sugar. Symptoms of the dawn phenomenon include Increased thirst, Increased hunger, Frequent urination, Headache, Irritability, and Blurred vision. The dawn phenomenon can be diagnosed with continuous glucose monitoring (CGM) [7].
It affects about half of people with type 1 or type 2 diabetes. To prevent high blood sugar levels when diabetics go to bed, they must eat dinner regularly, avoid large meals, eat meals with a higher protein to carbohydrate ratio, and eat dinner earlier in the evening. Oral anti-diabetes medications and long-acting insulin injections don’t help much in dawn phenomenon. The most effective approach for combating dawn phenomenon is taking insulin with an insulin pump. Other causes of morning hyperglycaemia include too little medication, which wears off overnight, under-calculating and or mistiming medication dose with evening /night meal and the Somogyi effect, which is injected insulin lowers the blood sugar too much overnight, and the body responds by releasing hormones that cause patients’ blood sugar to increase too much. The Somogyi effect happens when a hypoglycaemia episode overnight leads to high blood sugar hyperglycaemia in the morning due to a surge of hormones. It affects people with diabetes who take insulin [8].
The alleged mechanism for the hypoglycaemia is correlated with an abnormally rapid rise in blood glucose after eating. This normally leads to insulin secretion spike, which in turn initiates rapid glucose uptake by tissues, either storing it as glycogen or fat, or using it for energy production. The consequent fall in blood glucose is indicated as the reason for the “sugar crash”. Another cause might be hysteresis effect of insulin action, i.e., the effect of insulin is still prominent even if both plasma glucose and insulin levels were already low, causing a plasma glucose level eventually much lower than the baseline level.[4]. This condition may be confused with the after-effects of consuming large amounts of protein, which also produces fatigue, but is the result of the body prioritising the digestion of ingested food.
Immediately after food intake, insulin is released from pancreas that maintains blood glucose by activating glycolysis pathway along with suppression of glycogenolysis and gluconeogenesis pathway. The common cause of decreased postprandial glucose level is intake of antidiabetic medication and strenuous activity before sampling. Individuals with lesser PPBG level than FBG should be evaluated for possibility of meal induced hypoglycaemia also known as reactive hypoglycaemia. Various causes for this are-i) high insulin sensitivity, ii) exaggerated response of glucagon-like peptide-1, iii) defects in counter regulatory hormones like glucagon and iv) massive weight reduction. Chewing and eating slower can reduce the reactive glucose surge post meal. Other causes of lower PPBG includes gastroparesis seen in diabetic patient which an alter the rate and amount of food passing into small intestine causing erratic changes in blood sugar level. Some people deliberately eat less or eat non-carbohydrate meal before testing for PPBG level. It should be noted that fasting and postprandial glucose level help us adjust the dose of diabetic medications properly and glycated haemoglobin (HbA1c) helps to know whether there is an overall control to prevent complications. Due to individual variation of FBG and PPBG and large imprecision in analysis, some researchers have advocated the use of HbA1c only for diabetes diagnosis. [2].
It is essential to understand that laboratory error, though present in few cases is not always the cause for higher fasting blood glucose level than postprandial level. Healthy subjects with such laboratory finding should be followed for possibility of getting diabetes mellitus type 2 and should be advocated for lifestyle change along with dietary modification. In diabetics, changing the medication dosage, form or time should be considered along with counselling for a forementioned factors that affects laboratory result.
While all three tests namely i) FBS - Fasting Blood Sugar, ii) PPBS - Postprandial Blood Sugar, and iii) HbA1c- Glycosylated Hemoglobulin) are used to assess diabetes, the most reliable confirmatory test for diagnosing diabetes is generally considered to be the Fasting Blood Sugar (FBS) test. It provides a more accurate snapshot of the baseline blood glucose level without the fluctuations caused by meals; however, HbA1c is used alongside FBS to monitor long-term blood sugar control due to its ability to reflect average blood sugar levels over a period of 3 months. FBS: Considered as the gold standard for diagnosing diabetes as it measures blood glucose after a period of at least 8 hours of fasting, providing a clear picture of the blood sugar level without external influences. PPBS: This is useful in assessing how our blood sugar responds to a meal. It varies depending on what and when we eat it, making it less reliable for definitive diagnosis. Oral Glucose Tolerance Test (OGTT): This test is done to diagnose gestational diabetes, in which, blood sample is collected, and then lady is made to drink glucose (75 G) water. After 1-2 hrs of drinking glucose, her blood is checked again. the level of sugar in your body. HbA1c: This test measures the percentage of haemoglobin in your blood that has glucose attached to it, an indicator of our average blood sugar level over the past 2-3 months. While FBS is more reliable to separate diabetics from non-diabetics, HbA1c is used as a diagnostic test for diabetes providing that stringent quality assurance tests are in place. Epidemiological studies have concluded that FBS is more accurate than HbA1c. The best cutoff point for defining high HbA1c is 6% as HbA1c.
a hormone called glucagon which directs the liver to break down stored energy. The liver then releases glucose back into the bloodstream to normalize blood sugar levels. Too much alcohol disables the liver to release glucose back into the bloodstream, causing temporary hypoglycaemia. Medication: Taking heavy doses of diabetes medication also cause hypoglycaemia. Anti-malarial drugs, certain antibiotics, certain pneumonia medications have an increased risk of medication-induced hypoglycaemia, especially among children & people with kidney failure. Anorexia: Eating disorders like anorexia results in consuming not enough food for their body to produce sufficient glucose.
Hepatitis: Hepatitis prevent the liver from working properly. Adrenal or Pituitary gland disorders: These organs of the human body produce the hormones that control glucose production and therefore any disorder of these parts may lead to hypoglycaemia. Kidney problems: The kidneys help the body process medication and excrete waste. Any problem of the kidneys, medication build up in the bloodstream, which change blood sugar levels and lead to hypoglycaemia. Pancreatic Tumours: Tumours in the pancreas cause it to produce too much insulin, and high insulin levels will make blood sugar levels drop. Metformin Toxicity Induced Hypoglycaemia: Metformin toxicity can induce Hypoglycaemia due to anaerobic metabolism, decreased oral fluid intake and decreased glucose production and absorption.
Diabetes Diagnosis 2024 Guidelines
Diabetes is diagnosed based on A1C or either the fasting plasma glucose (FPG) value, 2-h after a 75-g oral glucose tolerance test (OGTT), or regular meals or random glucose value accompanied by classic hyperglycaemic symptoms (e.g., polyuria, polydipsia, and unexplained weight loss) or hyperglycaemic or hypoglycaemic crises.
- Causes of Hypoglycaemia Without Diabetes
- Alcoholism: Drinking too much alcohol can make it difficult for the liver to function. It may no longer be able to release glucose back into the bloodstream. As the pancreas releases
- The current guidelines using A1C ≥6.5% (≥48 mmol/mol), after the test performed in a laboratory using a NGSP method certified and standardized to the DCCT assay.
- * OR
- FPG ≥126 mg/dL (≥7.0 mmol/L). Fasting is defined as no caloric intake for at least 8 h.
- * OR
- 2-h PG ≥200 mg/dL (≥11.1 mmol/L) Oral Glucose Tolerance Test (OGTT), performed using a glucose load containing the equivalent of 75 g anhydrous glucose dissolved in water.
- *OR
- In an individual with classic symptoms of hyperglycaemia or hypoglycaemic crisis, & a random plasma glucose ≥200 mg/dL or <70 mg /dL respectively
- A1C 5.7–6.4% (39–47 mmol/mol)
- OR
- FPG 100 mg/dL (5.6 mmol/L) to 125 mg/dL (6.9 mmol/L) (IFG)
- OR
- 2-h PG during 75-g OGTT 140 mg/dL (7.8 mmol/L) to 199 mg/dL (11.0 mmol/L) (IGT
Table 1: Criteria for the diagnosis of diabetes in nonpregnant individuals.
Hypoglycaemia is when blood sugar levels fall dangerously low (70mg/Dl). It occurs in people with diabetes but can affect others without diabetes as well. Untreated severe hypoglycaemia (<55mg/Dl) can be life-threatening. Treatments focus on returning blood sugar to safe levels of more than 70mg/Dl. In people with diabetes, taking too much insulin or not eating enough or exercising too much after taking insulin leads to Hypoglycaemia.
The Difference Between mmol/L and mg/dL of Blood sugar
Both sets of units are used to measure blood sugar level, and both give a measurement of the concentration of glucose in the blood, albeit in slightly different ways. While mmol/L gives the molarity, which is the number of molecules of a substance within a specified volume, in this case within 1 litre. mg/dL gives the concentration by the ratio of weight to volume, - milligrams per Dl.
mmol/L is the most common measurement used in the UK with mg/dL predominantly used in the USA, India and continental Europe.
Blood glucose typically varies from 4 mmol/L to 6 mmol/L for people without diabetes. Blood sugar (also called blood glucose) needs to be tightly controlled in the human body to minimise the risk of complications developing.
Formula to calculate mmol/l from mg/dl:
$$ m m o l / l = m g / d l / 1 8 $$
Formula to calculate mg/dl from mmol/l:
$$ m g / d l = 1 8 \times m m o l / l $$
Best Practices for Diagnosing RH in Smaller Settings
Use of CGM: use of continuous glucose monitoring for a short cycle of 2 weeks would help identifying the timing of Hyperglycaemia and mild hypoglycaemia and link to the routine diets quantities and contents and modify the same to keep sugar levels under safe range. However, the cost ranges from around 5000 to 40,000, depending on the device- example:
- Abbott’s FreeStyle Libre System includes a reader and a biosensor that provides continuous readings for up to 14 days. The cost for this system is around ₹11,000.
- Medtronic’s CGM transmitter system costs over ₹40,000.
- Amici Care CGM Real-Time Bluetooth Blood Sugar Check meter costs ₹14,549, and the transmitter costs ₹7,349 If the Patient Can’t Afford CGM: Monitor the BS using simple glucometer at different times i) fasting, pre-breakfast (just before BF), post breakfast (2hrs after BF), and similarly two times around (before and 2 hrs after) lunch and dinner. If the PPBS indicates hypoglycaemia repeat the blood sugar 4 hrs after the same meal as we did in our case.
It’s rare to diagnose a case RH until the patient lands in an emergency of Hypoglycaemia that occurs only when PPBS goes below 70 mg/dl. Accidentally may be identified in routine examination when FBS is lower than PPBS as was in our case.
Best Approaches for the Treatment
Standard Treatment Practice: Once diabetes is confirmed urgent treatment must be started to get the PPBS around 1440-150 mg/dl, as we have done. The clinician must advise the patient to avoid simple sugars, eating sumptuous sweets, increase the frequency of their meals, and reduce the size of their meals. Patients may require 6 small meals and 2-3 snacks per day. Increased protein and fibre in the meal may be beneficial. Choosing a variety of foods including containing high protein (meat and nonmeat based on patients’ dietary habits), more fruits and vegetables, dairy products, and whole grains. When drinking alcohol, eat food with it. Alpha-glucosidase inhibitors (AGIs- e.g., acarbose, Voglibose and miglitol) are usually prescribed when diet and physical activity alone aren’t enough to control blood sugar levels. The therapeutic goal must be to decrease PPG at 4hrs and HgA1C levels to near normal using the lowest effective acarbose dose, combined with metformin, or sulfonylureas, or insulin [1].
- Acarbose: Acarbose is a modified bacterial enzyme that is not absorbed much by the body. It’s taken three times a day with meals. It may rarely cause liver injury.
- Miglitol: A synthetic pseudo polysaccharide that is absorbed from the gastrointestinal tract. It’s taken three times a day with meals.
Emergency Management of Hypoglycaemia: If someone is experiencing hypoglycaemia and is conscious, help them by giving a drink containing sugar or make them eat a tablespoon of sugar directly. Diabetic associations across the world recommend the “15-15 rule”, which is eat or drink 15 grams of fast-acting carbohydrates, like sugar or glucose tablets, fruit juice, or honey. After 15 minutes, check their blood sugar again and repeat the process, until their blood sugar reaches at least 70 mg/dL. Consider a glucagon injection or nasal spray if available. It is better such patients are advised to carry Glucagon with them and learn self-injecting.
Dosage: For Injection Dosage Form (Powder for Solution): Adults and children 6 years and older and weighing 25 kilograms (kg) or more—1 (mL) injected subcutaneous (SC), or Intra- muscularly (IM), or into a vein (IV). The dose may be repeated while waiting for emergency assistance.
Children younger than 6 years of age and weighing less than 25 kg—0.5 mL injected under your skin, into a muscle, or into a vein.
For Injection Dosage Forms (Autoinjector or Prefilled Syringe): Adults and children 12 years of age and older—1 mg or 0.2 mL injected Subcutaneously. An additional dose of 1 mg or 0.2 mL may be repeated if there has been no response after 15 minutes while waiting for emergency assistance.
Children 2 to 11 years of age and weighing 45 kg or more—1 mg or 0.2 mL SC injection. An additional dose may be repeated if there has been no response after 15 minutes while waiting for emergency assistance.
Children 2 to 11 years of age and weighing less than 45 kg—0.5 mg or 0.1 mL SC injection. An additional dose may be repeated if there has been no response after 15 minutes while waiting for emergency assistance.
Children younger than 2 years of age—Use and dose must be determined by your doctor. If the person is unconscious, do not give them anything to drink if they are unable to swallow, as they are at risk of choking. Severe hypoglycaemia can cause serious complications, including seizures, coma, and even death.
Literature Review
- A literature review found following studies complimenting occurrence of Reactive Hypoglycaemia, mostly landing in emergency department of tertiary care institutions: Emergency Hypoglycaemic Episodes: A retrospective study of a total of 1196 hypoglycaemic episodes encountered, of which 772 had complete data that was analysed at the Emergency Department of a Medical college Hospital during August 2010- July 2013, Underlying causes for hypoglycaemia in the diabetic group (535) was due to medication 320 (60%), infections 108 (20%), and chronic kidney disease 61 (11.40%). Common underlying causes of hypoglycaemia in nondiabetic group 237, (30.69%) included infections 107 (45.15%), acute/chronic liver disease 42 (17.72%), and malignancies 22 (9.28%). Among diabetic subjects on antidiabetic medications (n = 320), distribution over 24 h duration clearly reported two peaks at 8th and 21st hr. [9].
- Another prospective study aimed to know the clinical profile of patients more than 18years of age presenting with Capillary Glucose Random Blood Sugar value less than 70mg/dl from the period of September 2018-May 2020 included 123 participants among which 69.1% of them were known Diabetes Mellitus with mean duration of 6.9 years. 71.5% presented with severe Hypoglycaemia. Neuroglycopenic symptoms were the most common presenting symptom among the diabetics however, autonomic symptoms were the most predominant symptom among non-diabetic population. Drug induced Hypoglycaemia was the most common cause among diabetic population (43.5%) and among non-diabetic group 28.9%, probably due to heavy food intake after fasting [10].
- Pancreatic Insulinoma: A 69-year-old man presented with episodes of postprandial blurry vision, sweating, and confusion for the last 2 years that were becoming more frequent over the last several weeks. Home blood glucose measurements revealed postprandial hypoglycaemia (glucose level, 45-70 mg/dL), and symptoms were consistent with the Whipple triad. Continuous glucose monitoring revealed only postprandial hypoglycaemia within 2 hours following meals. An outpatient fast was conducted with detectable insulin (6 μIU/mL) and C-peptide (2.0 ng/mL) levels with an elevated proinsulin (20.8 pmol/L) level when the serum blood glucose level dropped to 47 mg/dL (21 hours after the initiation of the fast). A computed tomography scan of the abdomen and pelvis showed a 1.6-cm hyper-enhancing lesion in the distal body of the pancreas. An endoscopic ultrasonography with fine- needle aspiration’s pathology revealed a low-grade, well-differentiated, neuroendocrine tumour, lymph vascular invasion, regional lymph node metastases, that confirmed a pancreatic neuroendocrine tumour [11].
- Recurrent Hypoglycaemia: A retrospective review of 11 cases presenting with recurrent RH symptoms reported that two patients experienced successful resolution of symptoms through lifestyle modifications. Metformin alone was effective in treating seven out of nine patients who received pharmacological treatment. Two patients with previous upper gastrointestinal surgery showed a partial response to metformin and benefited further from additional long-acting GLP-1 analogue. Pharmacological intervention led to significant reductions in insulin and C-peptide levels in repeat mixed meal tolerance tests A flash glucose monitoring technology (CGM) was useful in early detection & preventing episodes of hypoglycaemia in one of these patients with persistent symptoms [12, 13, 14].
These findings highlight the potential efficacy of escalated treatment strategies for RH, including the use of metformin, GLP-1 analogues, and flash glucose monitoring technology.
Research Gap and Future Guidance
Recent understanding is indicative of hypoglycaemia a common effect of treatment for diabetes and is prevalent among both T1D and T2D patients and reactive Hypoglycaemia more among T1D than T2D. Hypoglycaemia may acutely increase the risk of CV complications, because of reduced blood flow in the heart and electrical disturbances leading to arrhythmia and prolonged QT interval. In addition, chronic hypoglycaemia or recurrent hypoglycaemia may accelerate the development of subclinical CVD & atherosclerosis and exacerbate ischemia in the brain, increasing risks for dementia & stroke. Advanced age, treatment with sulfonylureas or insulin, & co-morbid renal disease are recognised as risk factors for reactive hypoglycaemia.
Improved glycaemic control definitively decreases the risk for microvascular diabetes complications, but not lowering on CVD risk and some have suggested an increased CVD risk with very tight glycaemic control. Therefore, the treatment of diabetes is recommended to be individualized to balance the goals of achieving adequate glycaemic control to prevent microvascular complications, while also avoiding hypoglycaemia and related complications [15, 16].
More aggressive glycaemic control should therefore be a goal among younger patients without substantial CVD to prevent later microvascular complications, and older patients and those with co-morbid conditions such as coronary artery disease, dementia, cerebrovascular disease, and renal disease should maintain the best glycaemic control possible while also preventing significant hypoglycaemia.
Conclusion
Bimodal distribution with peaks in incidences of hypoglycaemic attacks at 8th and 21st hours based on hourly distribution in a day can be correlated with the times just before next meal.
None of the patients should be neglected without proper evaluation of the ethology of hypoglycaemia and the problem should be addressed at each individual level.
Hypoglycaemia is mainly medication related in diabetics and infection is the leading cause in nondiabetics.
This problem needs to be addressed by treating physician from the perspective of patient education, and modification of medications as well.
More aggressive glycaemic control should therefore be a goal among younger patients without substantial CVD to prevent later microvascular complications, and older patients and those with co-morbid conditions such as coronary artery disease, dementia, cerebrovascular disease, and renal disease should maintain the best glycaemic control possible while also preventing significant hypoglycaemia. Increasing incidence of death over the years is alarming, and further studies are needed to conclude the root cause.
References
-
Younes YR, Cron N, Field BCT, Nayyar V, Clark J, et al. (2024) Proposed treatment strategy for reactive hypoglycaemia. Frontiers in Endocrinology 15: 1332702.
-
Bora K, Barman B, Ayubi AW (2018) The curious case of postprandial glucose less than fasting glucose: Bora K, et.al, Clin Chem Lab Med 56(9): e223-e225.
-
Faludi G, Bendersky G, Gerber P (1968) Functional hypoglycaemia in early latent diabetes. Ann N Y Acad Sci 148(3): 868-874.
-
Mitrakou A, Kelley D, Mokan M, Veneman T, Pangburn T, et al. (1992) Role of reduced suppression of glucose production and diminished early insulin release in impaired glucose tolerance. N Engl J Med 326(1): 22-29.
-
Güemes M, Melikyan M, Senniappan S, Hussain K (2016) Idiopathic postprandial hyperinsulinaemic hypoglycaemia. J Paediatric Endocrinol Metab 29(8): 915-292.
-
Goldfine AB, Patti ME (2016) How common is hypoglycaemia after gastric bypass?. Obes (Silver Spring) 24(6): 1210-1211.
-
Castro MR (2022) The dawn phenomenon: What can you do?. Mayo Clinic.
-
(2023) Somogyi-effect. Cleveland Clinic.
-
Kumar JG, Abhilash KPP, Saya RP, Tadipaneni N, Bose JM (2017) A retrospective study on epidemiology of hypoglycaemia in Emergency Department. Indian J Endocrinol Metab 21(1): 119-124.
-
Dhivyaramani L, Gnanadurai KR (2023) Profile of Patients with Hypoglycaemia Presenting to the Emergency Medicine Department of a Tertiary Care Hospital. Indian Med Assoc 121(2): 44-48.
-
Maher MD, Desai DN, Bajaj M (2022) Metastatic Insulinoma Presenting with Postprandial Hypoglycaemia. AACE Clin Case Rep 8(4): 154-157.
-
Pant V, Gautam K, Santosh P (2019) Postprandial Blood Glucose can be less than Fasting Blood Glucose and this is not a Laboratory Error. J Nepal Med Assoc 57(215): 67-68.
-
(2024) Diagnosis, Classification & Standards of Care in Diabetes-2024. Diabetes Care 47(1): S20-S42.
-
Guanyu W (2014) Raison d’être of insulin resistance: the adjustable threshold hypothesis. J R Soc Interface 11(101): 20140892.
-
Aldobeaban S, Mzahim B, Alshehri AA (2018) Recurrent hypoglycemia secondary to metformin toxicity in the absence of co-ingestions: a case report. J Med Case Rep 12: 223.
-
Snell-Bergeon JK, Wadwa RP (2012) Hypoglycaemia, Diabetes, and cardiovascular disease. Diabetes Technol Ther 14(1): 51-58.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda