Primary Health Care Providers And Contemporary Diagnosis & Management Of Chronic Heart Failure
Heart failure (HF) represents a complex clinical syndrome affecting multiple organs and systems of the body, which is a global public health concern because of its high prevalence, mortality, and medical cost. Asia, with its vast population, diverse ethnicities, and complex health care systems, faces challenges in the prevention and management of HF. In Asia, and particularly in India comprehensive data regarding the epidemiology and burden of HF remain limited. HF remains a serious public health problem in Asia with significant regional variation; thus, strengthening the prevention and standardized management of HF in Asia is urgently needed. Chronic Heart failure is associated with shorter life expectancy, increased frequency of hospitalization and poor quality of life (QoL) but does not attract the attention of the policy makers and even health professionals like the Heart attack or Stroke. The leading causes of heart failure are Ischaemic heart diseases and Hypertensive heart diseases. In India CHF patients are younger & sicker than those in developed countries & are unable to tolerate the high levels of medication recommended by West guidelines. Advanced therapies and devices commonly used in developed countries are often out of reach for many HF patients in India. A stark statistic reveals that 50% of individuals diagnosed with heart failure (HF) face mortality within 5 yrs. There is a glaring unmet need in HF with a shortage of approved therapies in certain forms of the condition Materials and Methods: This article is based on half dozen cases of Chronic heart failure the author managed or referred for management in 2023 and 2024, representing the most common reasons and two rare conditions of chronic heart failure in Karnatak & India. Indian management practices are captured as practiced or seen being done in tertiary care hospitals mostly in private sector. The literature review adds latest developments in CHF management globally. Outcomes: Of the six cases reported the youngest two and 2 elderly patients survived current episode & two elderly succumbed to Cardiac/Hepatic/or Renal /or multi organ failure.
Abbreviations
CVDs: Cardiovascular Diseases; CHF/CCF: Chronic Heart (Cardiac) Failure; QoL: Quality of Life; RHD: Rheumatic Heart Disease; CKD: Chronic Kidney Disease; IHD: Ischaemic Heart Disease; VHD: Valvular Heart Disease; AF: Atrial Fibrillation;
DM: Diabetes Mellitus; T2D: Diabetes Type 2. Introduction
Heart failure (HF) represents a complex clinical syndrome affecting multiple organs and systems of the body. It is a global public health concern because of its high prevalence, mortality, and medical cost. Developing countries, Asia, in Particular India with their vast populations, diverse ethnicities, and complex health care systems, face challenges in the prevention and management of HF. In India comprehensive data regarding the epidemiology and community level burden of HF is limited. Chronic Heart failure is associated with shorter life expectancy, increased frequency of hospitalization and poor quality of life (QoL). While Heart attacks, Cardiac arrests find media and health systems attention and response, Chronic Heart failure, does not attract due attention of the people, policy makers and even health professionals like any of them. HF remains a serious public health problem in Asia and India with significant regional variation; thus needs an urgent strengthening of its prevention and standardized management practices [1].
Heart attack, cardiac arrest and heart failure are terms often used interchangeably, but they mean different things. Cardiac arrest is caused by disruption to the heart’s rhythm, whereas a heart attack is linked to blood circulation issues. Heart failure is a long-term condition and can occur when the heart is unable to pump blood according to one’s body needs. Basic health checkups like, Blood Pressure, Blood sugar monitoring and eye tests help screening of these diseases and have the potential to save many lives [2].
Chronic Heart failure is associated with shorter life expectancy, increased frequency of hospitalization and poor quality of life (QoL). It is a major public health challenge in India. As the actual data of CHF (CCF) is sparse, Indian data is based on extrapolation of risk factors of CHF, like hypertension, ischemic heart disease (IHD), obesity, diabetes mellitus (DM), & rheumatic heart disease (RHD), AF = atrial fibrillation; CKD = chronic kidney disease; and VHD = valvular heart disease. The burden of chronic heart failure (CHF) in India is high, with estimates of prevalence ranging from 1.3 million to 4.6 million people and the annual incidence between 0.5 & 1.8 million cases. HF is the most common cardiac cause of hospitalization & re-hospitalization for the elderly patients with CCF [3].
In India CHF patients are younger & sicker than those in developed countries & are unable to tolerate the high levels of medication recommended by West guidelines. Advanced therapies and devices commonly used in developed countries are often out of reach for many HF patients in India. A stark statistic reveals that 50% of individuals diagnosed with heart failure (HF) face mortality within 5 yrs. There is a glaring unmet need in HF with a shortage of approved therapies in certain forms of the condition [3, 4].
While most global attention is towards hear attacks, chronic Heart failure a progressive and debilitating disease is increasing in epidemic proportions & affecting People worldwide and needs similar attention if not more! [1]
This article is based on half dozen cases of Chronic heart failure the author facilitated management in 2023 and 2024, representing the most common reasons of chronic heart failure and two rare conditions. Indian management practices are captured as seen and the literature review adds latest developments in CHF management globally.
Case Reports
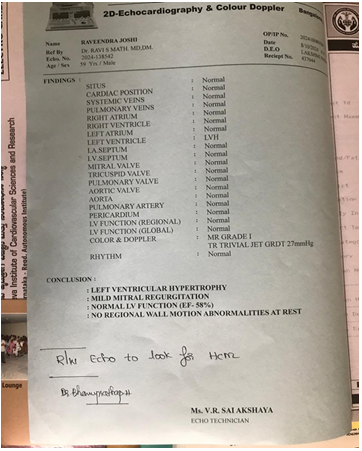
Case 1: Poor management of hypertension led heart failure: Ravi Joshi aged 50 years, a known hypertensive for 5 years, poorly maintaining his Blood pressure approached a general practitioner in Bengaluru 0n 8th October 2024 with the Complaints of i) Discomfort in chest -2 Weeks ii) Fatigue- 4 Weeks iii) Breathlessness on taking stair iv) Had put on weight of 25 kg (65-90 kg). His medical student daughter took him to Jayadeva Cardiac OPD, a public sector super- speciality hospital. Apart from raised BP of 165/105, his 2 D echocardiography showed Left ventricular Hypertrophy, Mild mitral valve regurgitation, a normal function efficiency (EF- 58%) with no regional wall motion abnormalities. Diagnosed as Stage 2 CHF his BP is being aggressively managed for the last 8 weeks (Figure 1 ).
Case 2: Post angiopasty led electrolyte and acid-base abnormalities led heart Failure: Mr Rammurthy Age-67 years, heavily built (overweight) known Hypertensive for 10 years, poorly, well managed, But since year it had become resistnat to the treatment being given. Complained of chest pain on 15 September 2024, an Angiography followed by 2 stents in first week of October wnet home feeling well. On 19th October 2024, had a few vomittings and the situation worsened to admit in ICU. He had electrolyte depletion, as electrolyte and acid-base abnormalities are common in people with congestive heart failure, due to the pathophysiology of heart failure or to adverse events of therapy. Alternately he must have had Electrolyte disorders could have triggeed microvascular dysfunction, leading to death on 21 October 2024.
Case 3: Chronic Liver function failure leading to Cardio- Hepato-renal failure: Srinivas Murthy 67 year, known hypertensive and diabetic for 7 years complained of poor appetite since April 2024 and weakness. A physician suspected mild Jaundice and got liver functions tested on 21 August 2024 which inferred icteric sample due to raised Bilirubin (5.3mg/dl) Serum Albumin (1.9), SGOT (70 u/l) SGPT (52u/l). He was on antibiotics and diuretics for pedal oedema. In early September 24 he developed Ascites, for which peritoneal fluid was tapped thrice in 6 weeks. He went into anuria on 7 September and was admitted to a medical college ICU. All efforts to revive was done but Cardio-Hepatic renal failure and died with 48 hrs.
Case 4: CHF due to Hypertension and CKD: Name: Sridhar Joshi, Age- 74 years, known hypertensive for 5 years, Irregular treatment complained of swelling of both feet. Consulted a Urologist, identified as CKD with CHF after Kidney function tests, scanning of pelvis and was advised water restriction, diuretics. Cardiologists’ consultation & 2 D doppler revealed CCF with Mild LVF. Hypertension took 8 weeks to stabilize starting from 2 drugs, increasing to 5 drugs for 4 weeks. Now BP is maintained with 3 drugs. Left Knee osteoarthritis, limits walking or exercise, complicating the management of BP.
Case 5: A Rare case of Cardiomyopathy in an Infant, beating end stage CHF: A private super speciality Paediatric Cardiac surgeon reported that a 10-month-old baby was brought with complaints of not eating properly for weeks, barely interacted, had swollen belly, failed to grow normally. Parents suspected Development delays and feeding/dietary intake problem initially and waited for almost first 9 months. At the hospital an investigation by an electrocardiogram revealed that the child was suffering from end stage heart failure caused by restrictive Cardiomyopathy case leading to chronic heart failure almost at the end stage. Fortunately, they got a heart from an accident case child and did the transplant on 18th August 2024 and the baby is doing well with increased activities, a healthy appetite, and steady weight gain after 6 weeks.
Case 6: Atrial Fibrillation induced CHF in a Female with Hypertension and Diabetes: Name: Kalavathy, Age: 65, diabetic for 20 years, well managed, hypertensive for 5 years on Atenolol 50 mg daily in January 2023 complained of Breathlessness, Fatigue, Bilateral swelling of feet. A comprehensive Blood count and other tests showed all but raised Blood urea level (11 mg/dl) as normal. ECG- reported Bradycardia, ECHO- showed Good LV function. A Diagnosis of HFpEF, due to Drug Induced Bradycardia & Hyperkalaemia was made. Just Stopping Atenolol Improved the condition after a hospital stay for 4 days. She is doing fine since then with other anti-hypertensives.
A Summary of our Case Reports
Chronic heart failure does not distinguish between rich and poor, however it affects more men than women of aged 40 years and above. Poorly managed Hypertension, diabetes type II, Dyslipidaemia, Chronic Kidney diseases, Chronic liver disease and drug induced atrial fibrillation especially due use of Atenolol for blood pressure maintenance.
Discussions
Among the cardiovascular diseases diagnosed 50% of individuals had Chronic heart failure (HF) and faced survival rate of just 5 yrs due to poor management of its causes, due to lack of condition-specific approved therapies and guidelines [1].
In 2023, and entire last decade, India has witnessed most attention of the media, individuals and professionals towards a rise in heart attack cases, particularly among younger people. In 2023 the number of cardiac emergencies was 35% higher than in 2018 and 29% higher than in 2022 Gujarat, led the number of cardiac emergencies in 2023, as EMRI 108 received a call every 7.5 minutes. The reasons for the increase in heart attacks in India include i) Sedentary lifestyle ii) poorly managed High blood pressure, obesity, and diabetes iii) Stress -a major risk factor for Hypertension, sudden cardiac deaths and coronary artery diseases.
Epidemiology of CHF in India: Heart failure is a condition in which the heart, fails to pump blood, commensurate to the requirements of the metabolizing tissues of any individual. It is either due to a detectable or even detectable abnormality of cardiac function or only with an elevated diastolic blood filling pressure. Heart failure is a growing global health concern, prevalence rising, especially in India, it affects 3 - 5% of adult population resulting in a burden of 30-60 million cases at any time. In India CHF patients are younger & sicker than those in developed countries and some of the patients are unable to tolerate the high levels of medication recommended by western guidelines. Advanced therapies and devices used in developed countries are often out of reach for many Heart Failure patients in India [3, 5].
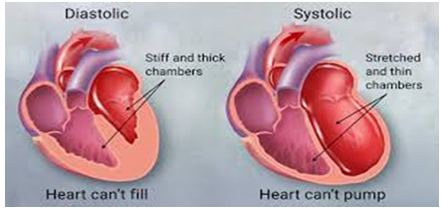
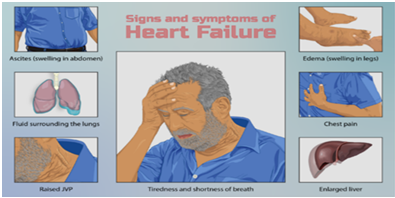
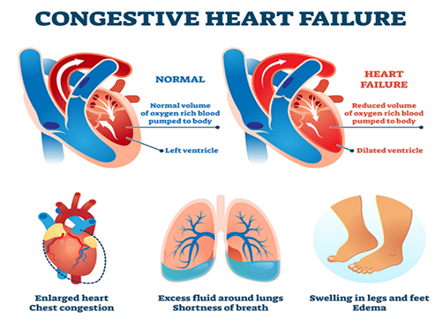
Heart failure is either predominantly systolic or diastolic (Figure 2). Patients with systolic heart failure also have some amount of diastolic dysfunction. A patient heart failure presents to practitioner with symptoms (Figure 3) of i) Exertional dyspnoea and/or dyspnoea at rest or Orthopnoea ii) Chest pain/ pressure iii)) Fatigue and weakness and palpitations iv) Nocturia and oliguria v) Anorexia, weight loss, nausea and on examination physicians finds the signs of i) Tachycardia, weak, rapid, and thready pulse ii) Exophthalmos and/or visible pulsation of eyes iii) ) Distention of neck veins iv) Rales and wheezing on auscultation of the chest due to pulmonary oedema, v) ECG shows S 3 gallop and/or pulsus alternans vi) Increased intensity of P 2 heart sound vii) Hepatojugular reflux viii) hepatomegaly, Ascites / Anasarca ix) Central or peripheral cyanosis, or x) Pallor. Chronic kidney disease (CKD), type 2 Disease, Obesity are known risk factors [3].
The primary health care providers are challenged with an initial diagnosis, referral decisions and long-term continuous management. Most general practitioners use the Framingham criteria for the diagnosis of heart failure which depends upon the concurrent presence of either two major criteria or one major and two minor criteria (Table 1) [3].
| Sl. No | Major Criteria | Minor Criteria- only if they cannot be attributed to another medical conditions |
|---|---|---|
| 1. | Paroxysmal nocturnal dyspnoea | |
| 2. | Weight loss of 4.5 kg in 5 days in response to treatment | Nocturnal cough |
| 3. | Neck vein distention & Hepatojugular reflux | Dyspnoea on ordinary exertion |
| 4. | Rales, Acute pulmonary oedema | A decrease in vital capacity by 1/3 the maximal value recorded |
| 5. | S 3 gallop | Pleural effusion |
| 6. | Central venous pressure >16 cm water | Tachycardia (rate of 120 bpm) |
| 7. | Circulation time of 25 seconds or longer | Hepatomegaly |
| 8. | Radiographic cardiomegaly | Bilateral ankle oedema |
| 9. | Pulmonary oedema, visceral congestion, or cardiomegaly at autopsy |
Table 1: Framingham criteria.
The age distribution of CHF cases by countries: Heart Failure (HF) is a multi-faceted and life-threatening syndrome characterized by significant morbidity and mortality, poor functional capacity and quality of life, and high costs. HF affects more than 64 million people annually worldwide.
While the age distribution of chronic heart failure in India is i) Under 30 years: 22.53% ii) 30–50 years: 24.29% and Over 50 years: 14.91%. A large-scale survey conducted across India, Teens accounted for 6% and young adults 3% and rest who suffered from heart problems in 2020 were 60 years and above [6]. Compared to this:
In US in 2022 CHF cases were among adults aged 18–44 was 0.9% years, 5.9% among those aged 45–64 years and 18.2% among those aged ≥65 years [7].
In the UK Heart failure affects around 920,000 people and causing 200,000 new cases each year. The prevalence of heart failure increases with age, from 1 in 35 people aged 65–74 to 1 in 7 people aged 85 or older. The average age of first diagnosis is 76 years old [8].
Categorization of Heart Failures
The New York Heart Association (NYHA) as Class I to IV
- Class I: No limitation of physical activity
- Class II: Slight limitation of physical activity
- Class III: Marked limitation of physical activity
- Class IV: Symptoms occur even at rest; discomfort with any physical activity
The American College of Cardiology (ACC) / American Heart Association (AHA) staging
- Stage A: High risk of heart failure but no structural heart disease or symptoms of heart failure- Risk factors in this stage include hypertension, coronary vascular disease, diabetes, obesity, exposure to cardiotoxic agents, Genetic variants and Family history of cardiomyopathy
- Stage B: Structural heart disease but no symptoms of heart failure
- Stage C: Structural heart disease & symptoms of heart failure
- Stage D: Refractory heart failure requiring specialized interventions (Figure 4).
Additional ACC/AHA/ and Heart Failure Society of America (HFSA) Disease-Staging Terminology Characterizes the Syndrome as a Continuum
- “At risk for HF” for stage A: Applied to asymptomatic patients with risk factors such as diabetes or hypertension but no known cardiac changes
- Pre-HF” for stage B: Adds cardiac structural changes or elevated natriuretic peptides, But still absence of symptoms
- “Symptomatic HF” for stage C: Structural disease with current or previous symptoms
- “Advanced HF” for stage D: Characterized by severe debilitating symptoms or repeated hospitalizations even with guideline-directed medical therapy (GDMT)
The Indian Cardiology Association (ICA) has a consensus Classification
- HF with reduced ejection fraction (HFrEF): HF with an LVEF of ≤40%
- HF with mildly reduced ejection fraction (HFmrEF): HF with an LVEF of 41% to 49%
- HF with preserved ejection fraction (HFpEF): HF with an LVEF of ≥50%
- HF with improved ejection fraction (HFimpEF): HF with a baseline LVEF of ≤40%, a ≥10-point increase from baseline LVEF, and a second measurement of LVEF >40% (Figures 6 & 7).
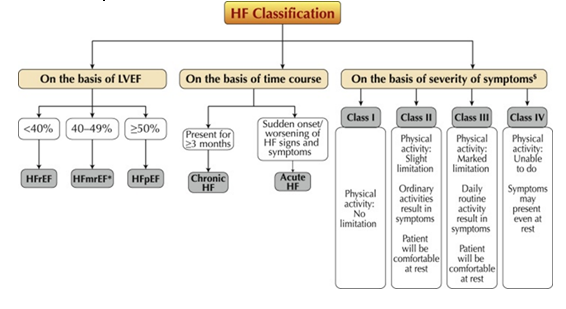
As there is no single agreed classification system for HF. Fig. 4 summarizes the commonly followed classification systems in HF management by the clinicians in India based on either LVEF, Time Course or Severity of Symptoms.
Hear Failure based on Left Ventricular Ejection Factor: Left ventricular ejection fraction (LVEF) is the central measure of left ventricular systolic function. LVEF is the fraction of chamber volume ejected in systole (stroke volume) in relation to the volume of the blood in the ventricle at the end of diastole (end-diastolic volume). Stroke volume (SV) is calculated as the difference between end-diastolic volume (EDV) and end-systolic volume (ESV). LVEF is calculated from: LVEF: [SV/EDV] x 100. Left ventricular ejection factor the cut off being 40% as against expected normal range of normal adults at 60%.
The simplest classification used clinically as follows: Hyperdynamic = LVEF greater than 70%, Normal = LVEF 50% to 70% (midpoint 60%) Mild dysfunction = LVEF 40% to 49% (midpoint 45%), Moderate dysfunction = LVEF 30% to 39% (midpoint 35%) and Severe dysfunction = LVEF less than 30%.
LVEF is a continuous variable with a normal distribution that changes with age and sex, so there is no single precise threshold for “normal”. However, current guidelines mandate treatment based on LVEF, categorizing heart failure as: Heart failure with reduced ejection fraction (HFrEF): Heart failure with mild reduced ejection fraction (HFmrEF): LVEF 40-49% and Heart failure with preserved ejection fraction (HFpEF): LVEF ≥50% [5]. Heart Failure Classification based on Time Course Hear failure present for 3 months or more is termed chronic heart failure and that either of sudden onset or worsening of signs and symptoms is called Acute Heart Failure.
The ICD-10-CM diagnosis code for left ventricular failure is I50.1. This code is used for reimbursement purposes. I50.2: Systolic heart failure, I50.3: Diastolic (congestive) heart failure, I50.4: Combined systolic and diastolic heart failure, I50.8: Other heart failure and I50.9: Unspecified heart failure
Pathophysiology of Heart Failure
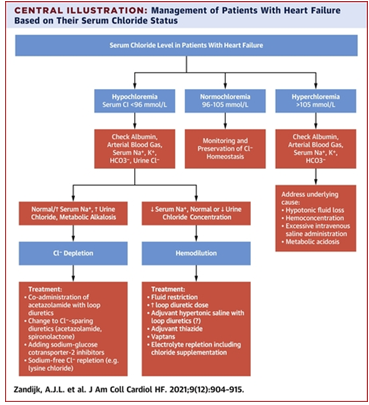
Electrolyte Disturbances: Recently studies have shown that chloride plays a significant role in HF pathophysiology and prognosis. Chloride an electrolyte was neglected in the medical literature and clinical practice for heart failure (HF) until recently.: i) Chloride abnormalities: Chloride abnormalities are a prognostic marker for HF ii) Hypochloraemia: is an independent predictor of adverse outcomes in both acute and chronic HF. iii) Role in fluid homeostasis: Chloride is a major electrolyte that plays a role in fluid homeostasis. Chloride is associated with the cardiorenal and neurohormonal systems iv) Diuretics: Diuretic agents can cause higher urinary chloride excretion and serum hypochloraemia.
Investigations used for CHF Diagnosis
Biomarkers: Common biomarkers prescribed include- i) Complete blood cell (CBC) count, Iron studies to rule out Anaemia, Urinalysis, Electrolyte levels & KFT for CKD, Liver function studies to rule out hepatic causes, Fasting blood glucose levels, Hb1Ac for T2D, Lipid profile, Thyroid stimulating hormone (TSH) levels, B-type natriuretic peptide levels and N-terminal pro-B-type natriuretic peptide levels.
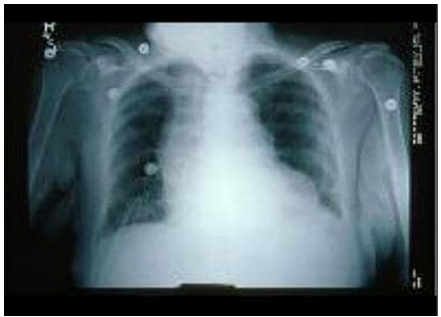
Imaging & Other Tests: i) Electrocardiography- ECG, ii) Two-dimensional (2-D) echocardiography for cardiac functioning and Atrial Fibrillation, iii) Chest radiography for Lungs & Pleural fluids iv) nuclear imaging v) Maximal exercise testing vi) Pulse oximetry or arterial blood gas vii) Non-invasive stress testing. Chest radiograph shows an enlarged cardiac silhouette and Oedema at the lung bases, signs of heart failure Management of CHF (CCF):
Knowing the fact that common causes of chronic heart failure are led by Hypertension, Diabetes, ischemic heart disease, dilated cardiomyopathy, and rheumatic heart disease and the key risk factors include older age, elevated serum creatinine levels, diabetes, and conditions like COPD, Asthma, Cirrhosis, Non-alcoholic Fatty liver & renal dysfunction (Figure 8).
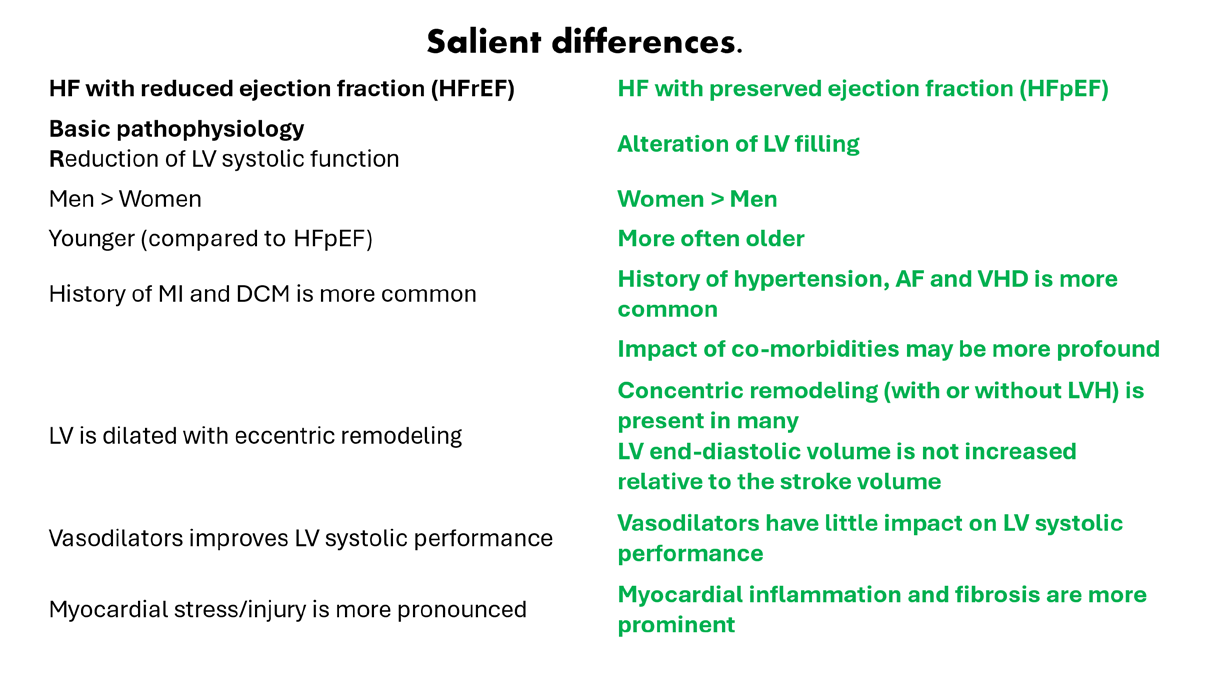
A clinician needs to be aware of distinguishing between heart failure with reduced ejection factor and with preserved ejection factor for better management. The following chart summarises the key feature of these two categories. The management of CHF involves two approaches namely medical management and surgical management. Medical management is either non-pharmacological management that includes Oxygen and non-invasive positive pressure ventilation, Dietary sodium & fluid restriction, Physical activity as appropriate, and attention to weight gain & Pharmacological therapies, using Diuretics, vasodilators, inotropic agents, anticoagulants, Beta blockers, ACEIs, ARBs, CCBs, digoxin, nitrates, B-type natriuretic peptides, Inhibitors, ARNIs, soluble guanylate cyclase stimulators, SGLT2Is, and MRAs.
Surgical treatment options include Electrophysiologic intervention, Revascularization procedures, Valve replacement/repair, Ventricular restoration, Extracorporeal membrane oxygenation, Ventricular assistance devices, Heart transplantation and a Total artificial heart. The latest surgical procedure in the western world is called Cardiac Resynchronization Therapy – which is like a conventional pacemaker except the leads are placed on both the right and left ventricles of the heart, rather than only the right ventricle, to resynchronize the heart in a more natural way.
The CHF treatment strategies have evolved in the past two decades. Primary prevention is crucial for those at risk for HF (stage A) or pre-HF (stage B). The revised stages of HF emphasize the new terminologies of “at risk” for HF for stage A and pre-HF for stage B.
**
- Urgent Referrals: Family / primary care physicians must refer those with advanced HF to review current HF management, HF patients with iron deficiency anaemia, coronary artery disease (CAD), AF, valvular heart disease, cardiomyopathy, hypertension, type 2 diabetes, sleep disorders, and malignancy, Patients with previous HFrEF with a left ventricular (LV) EF above 40% should be referred to as having improved LVEF.
- Pre HF-Status: The pre-HF state, encompasses asymptomatic patients, with either structural or functional cardiac abnormalities or have elevated plasma levels of natriuretic peptides or cardiac troponin be managed with non-pharmaceutical therapy.
- HF with preserved ejection fraction or mildly reduced ejection fraction: The first-line treatment of patients or with HF with preserved ejection fraction or mildly reduced ejection fraction includes SGLT2 inhibitors and diuretics. The timely initiation of disease-modifying therapies & the optimization of treatment are crucial. SGLT2Is are a class 2a (moderate) recommendation in HF with mildly reduced ejection fraction (HFmrEF).
- HF with preserved EF (HFpEF):** SGLT2Is (class 2a), MRAs (class 2b), & ARNIs (class 2b).
- Treatment of hypertension (class 1 [strong]) and of atrial fibrillation (AF) (class 2a); use of ARBs (class 2b); Avoid the use of nitrates or phosphodiesterase-5 (PDE5) inhibitors. **
- Amyloid heart disease:** Screening for serum and urine monoclonal light chains, bone scintigraphy, genetic sequencing, tetramer stabilizer therapy, & anticoagulation.
- If the LVEF is over 40%, one must establish increased filling pressures by non-invasive (natriuretic peptide, diastolic function on imaging) or invasive testing (hemodynamic measurement) to consider as CHF.
Reassessment after initiation of these therapies is recommended to evaluate patient symptoms, health status and left ventricular function. Lifestyle modification and treatment of comorbidities such as diabetes mellitus, ischemic heart disease and atrial fibrillation are crucial through each stage of HF [5].
Use of Beta-blockers: Beta-blockers are the cornerstone of heart failure management, with reduced ejection fraction (HFrEF) and particularly elderly, Diabetes and CKD patients. They play a crucial role in improving survival, reducing hospitalizations, and enhancing quality of life. For example, Metoprolol (Lopressor & Toprol XL), reduces all-cause mortality by 43% in elderly patients & Reduces hospitalizing in T2D. However, initiating beta-blocker therapy requires caution. Treatment must be started with low doses, gradually increasing while monitoring the patient. Betablockers are also preferred over digoxin in patients with atrial fibrillation and Asthma as they are effective in reducing heart rates without exacerbating bronchospasm. Before initiating therapy, optimizing diuretic treatment to alleviate congestion is essential. They must be discontinued if adverse effects like bradycardia or hypotension occur as was done in our case of Ms. Kalavathy.
Chloride in Heart Failure: The recent knowledge regarding chloride as a prognostic marker in HF have increased the interest in the pathophysiology and interactions of chloride abnormalities with HF-related factors and treatments. Chloride is among the major electrolytes that play a unique role in fluid homeostasis and is associated with cardiorenal & neurohormonal systems. Hypochloraemia is an independent predictor of adverse outcomes in acute or chronic HF. Chloride abnormalities is managed through administration of acetazolamide etc. as shown in the chart-3 below. Chloride depletion managing is challenging, as it often results in the death of the patient as was the case of Mr. Ramamurthy (Figure 9) [5, 9].
Advanced Medical Therapy: Advanced medical therapy and Implantable devices are the management strategies to be left to cardiologist. Just to make a passing mention these include:
- Lifestyle changes: Reducing fluids and salt, exercising regularly, and avoiding tobacco.
- Medications: Giving diuretics to reduce fluids, digitalis and ACE inhibitors to boost heart strength, and beta blockers, ACE inhibitors, calcium channel blockers, or antiarrhythmics to control high blood pressure, arrhythmias, or coronary artery disease.
- Invasive therapies: Cardiac resynchronization therapy (CRT), pacemakers, implantable cardioverter- defibrillators (ICDs), coronary artery bypass grafting (CABG), percutaneous coronary intervention (PCI), valve replacement or repair, and ventricular restoration.
- Mechanical circulatory devices: Cardiologists use implantable devices to treat when medications do not reduce a patient’s symptoms. • Cardiac Contractility Modulation (CCM) Devices: In the last decade, a CCM which improves the overall function of the heart is being used.
The device stimulates the heart with timed electrical pulses throughout the day and ensures a better quality of life. **
- Implantable Cardioverter-Defibrillators (ICD): ICDs are Implanted trans-venously or subcutaneously, for patients at higher risk for infection or for very young patients. Both prevent sudden cardiac death (cardiac arrest).
- Cardiac Resynchronization Therapy:** Most recent devise is a conventional pacemaker in which the leads are placed on both the right and left ventricles of the heart, to resynchronize the heart in a more natural way for heart failure due to electrical desynchrony. Patients who had a pacemaker for many years (leads on only right ventricle) and develop heart failure due to lack of synchrony between the right and left ventricle, are benefitted with this devise.
Surgical Interventions
Right heart catheterization and hemodynamic: These procedures are useful in tailoring therapy in advanced heart failure and in acute settings. In preparation for listing for cardiac transplantation, a right heart catheterization is performed on all candidates to assess for pulmonary hypertension and cardiac output [10]. Heart transplantation: This is the standard therapy for progressive end-stage heart failure when there is no other therapeutic alternative left [10, 11].
Conclusion
Heart failure (HF) is a clinical syndrome characterized by dyspnoea, fatigue and fluid retention accompanied by objective evidence of cardiac dysfunction. In Asia, comprehensive data regarding the epidemiology and burden of HF remain limited. The burden of HF in India is high, and estimates of prevalence range from 2 million to 20 million, with an annual incidence of 0.5–2.0 million. The syndrome affects 2% of the adult population, men more commonly than women (<80 years old), with the incidence & prevalence rising steeply with age. There is a significant co-occurrence of HF and CKD as almost half of patients with HF have a degree of renal impairment, and HF is prevalent in 25%- 50% of patients with CKD, depending on the stage & age The annual number of deaths from CVD in India is projected to 5 million (2023) Even in developed countries like America about 6.7 million individuals over the age of 20 years, about a million in UK and 8.9 million patients in China among adults aged 35 and older, currently live with heart failure. References
5. Ramic-Catak A, Mesihovic-Dinarevic S, Prnjavorac B, Naser N, Masic I (2023) Public Health Dimensions of Cardiovascular Diseases (CVD) Prevention and Control – Global Perspectives and Current Situation in the Federation of Bosnia and Herzegovina. Mater Sociomed 35(2): 88-93.
6. Ellerbeck (2020) What’s the difference between a heart attack, cardiac arrest and heart failuseveral
7. Gautam V, Ramani (2010) Chronic heart failure: contemporary diagnosis and management, Review Mayo Clin Proc 85(2): 180-195.
8. Mishra S (2017) Management protocols for chronic heart failure in India, Indian Heart J 1: 105-127.
9. Feng J (2020) Epidemiology & Burden of Heart Failure in Asia.
10. Minhas A (2023) Age distribution of CHF patients in 2020.
11. Bozkurt B, Ahmad T,Alexander KM, Baker WL, Bosak K et al. (2023) Heart Failure Epidemiology and Outcomes Statistics: A Report of the Heart Failure Society of America. J Card Fail 29(10): 1412-1451.
12. Bellanca L, Linden S, Farmer R (2023) Incidence and prevalence of heart failure in England: a descriptive analysis of linked primary and secondary care data - the PULSE study. BMC Cardiovasc Disord 23(1): 374.
13. Bozkurt B (2024) Contemporary pharmacological treatment and management of heart failure. Nat Rev Cardiol 21: 545-555.
14. Krishna Gaddam K, Yelamanchili P, Sedghi Y, Hector
Ventura O (2009) Advanced Heart Failure and Management Strategies. Ochsner J 9(4): 227-233. 15. Arietje JL (2021) Chloride in Heart Failure: The Neglected Electrolyte.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda