Multidisciplinary Approach for Rehabilitation of Patients with Central Vision Loss: Benefits on the Quality of Life
Background: Low vision is one of the leading causes of disability induced by chronic eye diseases. Therefore, low vision can affect Quality Life because the progressive degenerative diseases produce a state of emotional uncertainty making existential planning different, it can produce feelings of inadequacy, lack of self-esteem, helplessness, loneliness or marginalization and loss of autonomy, leading to psychological and emotional isolation. As far as emotional aspects are concerned, in order to highlight the importance of quality of life, many studies showed the relationship between low vision and prevalence of depressive disorders. The National Eye Institute developed a questionnaire, the Visual Function Questionnaire NEI VFQ-25, to evaluate the subjective perception of the quality of life and has been proposed not only to ascertain the impact of low vision on a person’s quality of life, but also to evaluate the real effectiveness of the rehabilitation process. The primary intervention for people with progressive and irreversible vision impairment is the visual rehabilitation. Objective: The purpose of this study is to evaluate patients’ quality of life, measured by the NEI VFQ-25, before and after the multidisciplinary visual rehabilitation. Method: Low-vision assessment included: psychological assessment, administered the Visual Function Questionnaire (VFQ), developed by The National Eye Institute (NEI), complete ophthalmological examination, low vision device training and at last the prescription of low-vision devices. Results: A statistically significant improvement was found in some areas of self-reported perception (VFQ25), on General vision, near activities and Peripheral vision, and in reading speed. Data for control group remained unchanged. Conclusion: Multidisciplinary low-vision intervention, that includes emotional support, could enhance the quality of life of subjects with central vision loss.
Introduction
Quality of life (QoL) is a concept that includes physical health, psychological state, level of independence, social relationships, personal beliefs and the relationships between these factors and the salient features of the environment. As argued by several authors [1, 2], QoL includes both objective and subjective indicators, ranging from the living conditions to evaluations of the personal life situation. According to Aaronson’s findings [3], a proper evaluation of quality of life should consider: a physical and functional axis (symptoms and treatment of the disease),concerning both clinical parameters and organs and systems’ functionality; a psychological axis (cognitive function, emotional status, well- being, life satisfaction and happiness), including emotional and cognitive skills; a social axis (self-care, mobility, activity level and daily living activities), dealing with inter-personal experiences and expertise in social relations. In medicine, the measurement of QoL is a way to assess the impact of diseases on the patient’s physical and psychosocial features. QoL can indeed be used as an index of the potential influence of impairment on individuals.
Low vision is one of the leading causes of disability induced by chronic eye diseases [4]. In industrialized countries, the most important cause of visual impairment, having an impact on both patients’ psychological status and quality of life, is macular degeneration. Macular diseases (MD) are characterized by the progressive loss of central vision representing a severe limitation of patients’ visual function. Age-related macular degeneration (AMD) is the most common form of senile maculopathy. Moreover, other forms, such as Stargardt’s disease, affect young subjects on a genetic basis. The distinctive symptom of macular disease is the initial perception of altered and distorted images followed by a gradual and progressive reduction of central vision, which interfere with the ability to perform daily activities such as reading, recognizing faces, watching TV, etc. [5]. These difficulties may result in loss of independence, limiting social interaction up to a significant narrowing of social interests, with consequent impact on the perception of QoL.
Therefore, low vision can affect QoL because the progressive degenerative diseases produce a state of emotional uncertainty making existential planning different, it can produce feelings of inadequacy, lack of self-esteem, helplessness, loneliness or marginalization and loss of autonomy, leading to psychological and emotional isolation. As far as emotional aspects are concerned, in order to highlight the importance of quality of life, many studies showed the relationship between low vision and prevalence of depressive disorders [6, 7, 8, 9, 10]. The National Eye Institute developed a questionnaire, the Visual Function Questionnaire NEI VFQ-25, to evaluate the subjective perception of the quality of life and has been proposed not only to assess the impact of low vision on a person’s quality of life, but also to evaluate the real effectiveness of the rehabilitation process that end with the prescription of aids [11].
Low vision rehabilitation, in fact, is the primary intervention for people with progressive and irreversible vision impairment [12]. Its goal is to improve engagement in activities of daily living by helping people with reduced visual functions to optimize the use of their remaining sight through the provision of appropriate refractive correction, as well as providing training in the use of vision assistive equipment (VAE) and compensatory strategies [13]. The most compromised task in patients with low vision is reading since of the reduction of visual acuity and the presence of an absolute scotoma, making it difficult for the patient to recognize printed characters. Approximately 86% of the patients who were referred to low vision rehabilitation Centre were found to have problems with reading task [14]. Many different low vision rehabilitation protocols are currently available. In particular, at National Centre of Services and Research for the Prevention of Blindness and Rehabilitation of the Visually Impaired, a WHO Collaborating Centre, low vision rehabilitation is based on a multidisciplinary approach that includes a complete functional disability assessment and psychological assement. The purpose of this study is to evaluate patients’ quality of life, measured by the NEI VFQ-25, before and after the multidisciplinary visual rehabilitation.
Methods
Participants
Eighty-four health records of patients with MD from the attendees of our center were retrospectively reviewed. Subjects (44 females, 40 males; median age of 67.5 years, range: 18-94) with different macular diseases such as age related macular degeneration, myopic maculopathy and Stargardt’s disease were analyzed for the study. During one year of activity, a total of 125 patients with a diagnosis of MD were referred to our center. Of these patients, 5 had a worsening of visual acuity, 2 did not give their informed consent, 6 did not come back to our low vision center for general health issues, 4 did not buy the prescribed low vision devices and 24 refused to attend psychological counseling, and were excluded from the analysis. Another twenty patients (10 females and 10 males) between those who refused to attend psychological counseling formed the control group (Figure 1). Patients’ charts were analyzed based on the diagnosis of MD with the following clinical criteria: a Best Corrected Visual Acuity (BCVA) between 1 logMAR and 0.5 LogMAR, unchanged until 6 months follow-up; a completed vision rehabilitation program and bilateral central vision impairment. All patients spoke Italian as their first language. Subjects’ clinical charts were excluded if they reported other concomitant eye or neurophthalmologic diseases, cognitive impairment, ocular surgery in the previous three months. The approval for this study was obtained from the Ethical Committee/Institutional Review Board of the Catholic University of Rome. Informed Consent was obtained by all participants and the study is conformed to the Declaration of Helsinki.
Low Vision Rehabilitation Procedure
In our Centre, low-vision assessment as standard procedure included: psychological assessment, administered the Visual Function Questionnaire (VFQ), developed by The National Eye Institute (NEI), complete ophthalmological examination, low vision device training and at last the prescription of low-vision devices. The psychologist is a key figure in the multidisciplinary rehabilitation team, both for supporting patients during their low vision rehabilitation pathway, and assessing any progression of self-reported vision functionality in activities of daily living [15, 16]. It should be taken into account that people with visual impairments can develop depressive symptoms that if not receive any form of treatment can hinder not only potential access to the rehabilitation path but also and especially its effectiveness [17]. The psychologist provided a specialized assessment in order to define better patients’ difficulties and needs. During the psychological counseling, the operator discussed the intervention approaches to address the activities of daily living and performances at home for visually impaired. The demand’s analysis is aimed in order to set a customizable rehabilitation pathway and to overcome the patients’ expressed difficulties, for example reading.
He supported patients in focusing on personal goals in order to facilitate independence in activities of daily life and through the clinical interview, evaluated the presence or absence of depressive symptoms in accordance to DSM-V (little interest or pleasure in doing things; feeling down, depressed, or hopeless; trouble falling or staying asleep, or sleeping too much, etc.). The NEI-VFQ-25 was used as measure of vision-related functioning outcome and it was developed to assess vision functioning outcomes among a range of ocular conditions. In order to evaluate patients’ QoL before low vision intervention and at 6 months follow up, the Italian version of the NEI-VFQ25 was submitted [18].
This questionnaire was set to assess the impact of low vision on the quality of life of the patient, as well as to evaluate the actual effectiveness of the rehabilitation process ending with the prescription of assistive device. The NEI-VFQ25 version can be considered a very sensitive instrument to detect changes in the perception of quality of life before and after visual rehabilitation programs [19, 20].
The NEI-VFQ25 includes 12 vision related subscales: general vision, near vision, distance vision, driving, peripheral vision, color vision, ocular pain, general health, vision specific role difficulties, vision-specific dependency, vision specific social function, and vision-specific mental health. Each subscale is ranged between 0, representing the lowest visual functioning and 100, representing the best possible one. An overall composite score is calculated as the mean of the subscale scores except for the general health score. Moreover, the questionnaire is composed by an appendix of 13 optional items. Once the psychological counseling was completed, he transmitted relevant information to the ophthalmologist to facilitate the creation of a better empathetic relationship between doctor and patient.
The ophthalmologist evaluated the BCVA by the Early Treatment of Diabetic Treatment Study charts at 4 m (Precision Vision, Bloomington, IL) in LogMAR. Moreover, the ophthalmologist determined the near visual acuity by means of Italian MN Read charts adding +4 spherical dioptres. After patients had completed the evaluation process, the team met to design a customized rehabilitative pathway for each patient, based on psychosocial characteristics (adaptation to vision loss, family and social support, trait of personality) and clinical and functional visual assessment. Devices training session consisted of 1 weekly session provided by an orthoptist to teach patients how to correctly use magnifying devices and to suggest strategies to perform daily living tasks independently. In particular, to restore reading ability, visual rehabilitation training sessions focused on identifying the most suitable device for reading, managing the device, and teaching page navigation strategies. Each session went on for about one hour and on average three sessions was required. Moreover, if needed, training sessions were associated to psychological support.
Reading speed was calculated with the most appropriate low vision devices in words read correctly in one minute (WPM) on an Italian newspaper. Therefore, appropriate low- vision devices were prescribed at the end of the low vision rehabilitation pathway. Consecutive visits at low vision center took place 6 months after the prescription of low vision aids. During follow-up (6 months) psychological counselling, VFQ- 25 questionnaire, Ophthalmological assessment and reading speed were determined.
Measures
The data extracted from the low-vision clinical charts for this retrospective review, from baseline to 6 months follow up period, included: psychological counselling, NEI VFQ- 25 Questionnaire, BCVA, magnified-assisted evaluation of reading rate.
Statistical Analysis
Patients’ clinical outcomes, including VFQ-25, were analyzed using a paired t test in order to evaluate changes in between the baseline and the follow-up assessment. Data were managed and stored by only one operator. Patients’ data were collected and divided in several group according to gender, age, degree level and presence or not of depressive symptoms. A Spearman’s correlation analysis was performed in order to verify the association features between VFQ- 25 and social patients’ characteristics. A p value was set at <0,05 as an indicator of statistical significance. The driving subscale was not analyzed (missing) because none of our patients’ was able to drive.
Results
Vision Related Quality of Life at 6 Months Follow-Up
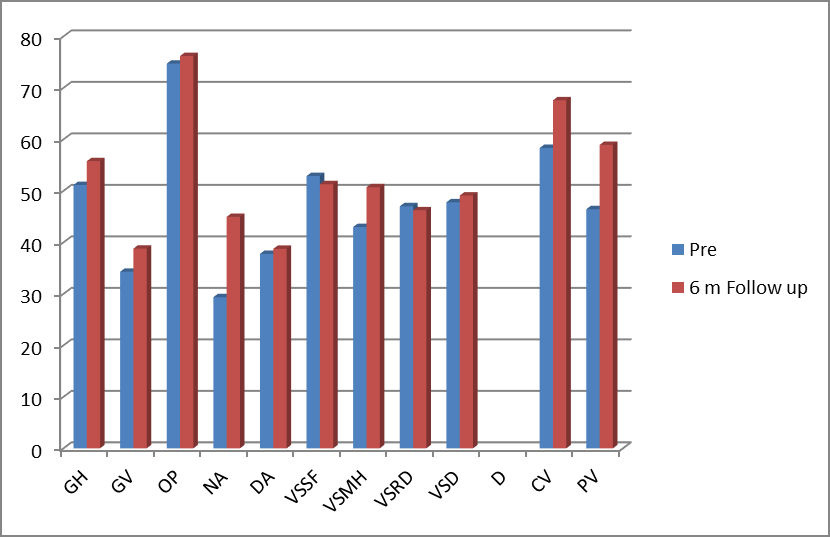
After 6 months follow-up, BCVA remained unchanged: 0,72 (± 0,73) in the right eye and 0,89 (±0,8) in the left eye. As shown in Figure 1, for each VFQ-25 Item we identified the result before the visual rehabilitation pathway and after 6 months from the provision of low vision aids. The questionnaire revealed significant differences in 3 of 12 subscales groups: General vision (GV) (F=4,49; p=0,03), Near activities (NA) (F=15,6; p<0,001), Peripheral vision (PV) (F=12,5; p=0,004). Mean reading speed for the whole sample improved at 53,29 (±37,57) wpm 6 months after the low vision devices provision (p=0,004). In addition, patients were divided according to gender; the male group showed a statistically significant improvement on self-perception of NA (F=13,45; p=0,0003) and PV (F=15,91; p=0,007). On the other hand, the female group demonstrated a statistically significant improvement on NA only (F=17,96; p=0,005) (Table 3). As regarding reading performances at 6 months follow-up, the female group had higher reading speed when compared to the male group. Reading speed was significantly enhanced for women at 6 months follow up (p=0,02).
Moreover, patients were divided into several groups according to their age:
- Group 1 Patients’ age between 18 and 49 years (N=16; 19%)
- Group 2 Patients’ age between 50 and 75 years (N=30; 36%)
- Group 3 Patients’ age more than 75 years. (N=38; 45%) and to the presence of depressive symptoms
- Group 1 Presence of depressive symptoms due to eye disease: (N=48; 57%)
- Group 2 No presence of depressive symptoms due to eye disease: (N=36; 43%).
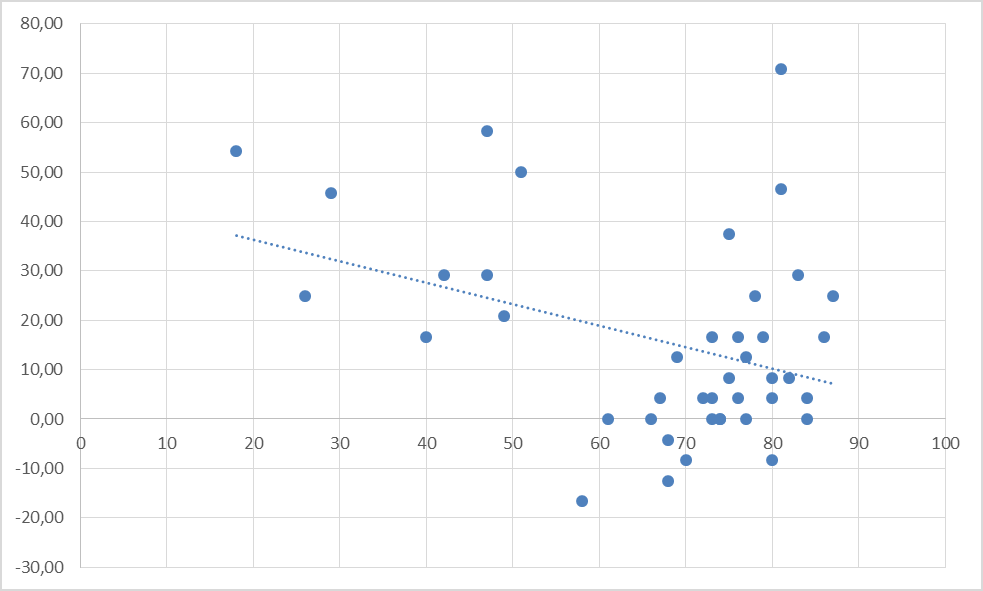
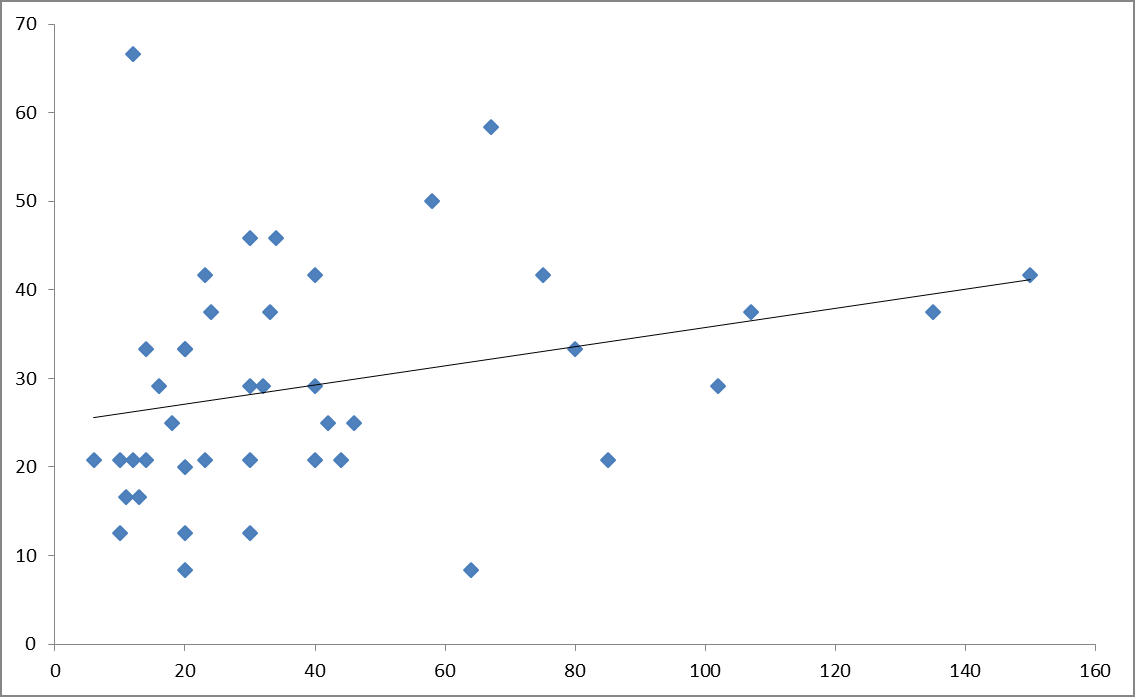
A statistically significant relationship was found between patients’ age and self-reported measures of near activities (Figure 2). As for the presence of depressive symptoms, slightly more than half of the patients suffered from depressive symptoms (57%). The number of patients with depressive symptoms remained roughly constant during the whole process of rehabilitation. Moreover, a positive correlation was found between self-perception on Near Activities item of NEI-VFQ25 and reading speed with low vision device at 6 months follow-up (r=0,28; F=3,44, p<0,01) (Figure 3).
| VFQ-25 | Pre VR | 6 M Follow-up | F | p | Pre VR | 6 M Follow-up | F | p |
|---|---|---|---|---|---|---|---|---|
| Male | Female | |||||||
| Mean, SD | Mean, SD | Mean, SD | Mean, SD | |||||
| General health (GH) | 53,3±14,91 | 58,75±16,25 | 5,45 | 0,13 | 48,75±14,97 | 52,5±22,2 | 3,75 | 0,38 |
| General vision (GV) | 34,32±10,61 | 38,52±25,82 | 4,2 | 0,13 | 34,25±11,62 | 39,06±16,42 | 4,81 | 0,13 |
| Ocular Pain (OP) | 81,82±21,03 | 81,82±22,05 | 0 | 1 | 66,88±26,06 | 70±27,02 | 3,13 | 0,63 |
| Near activities (NA) | 32,2±13,98 | 45,64±18,21 | 13,45 | 0,0003 | 26,21±11,5 | 44,17±25,49 | 17,96 | 0,005 |
| Distance activities (DA) | 43,3±18,54 | 43,94±22,6 | 0,64 | 0,88 | 31,67±19,56 | 33,02±26,25 | 1,35 | 0,8 |
| Vision-specific social functioning (VSSF) | 58,14±21,38 | 58,14±24,21 | 0 | 1 | 47,08±30,38 | 43,75±26,2 | -3,33 | 0,67 |
| Vision-specific mental health (VSMH) | 43,18±27,8 | 51,36±30,09 | 8,18 | 0,1 | 42,75±25 | 50±33,99 | 7,25 | 0,38 |
| Vision-specific role difficulties (VSRD) | 51,42±24,99 | 50,75±20,54 | -0,67 | 0,91 | 42,19±19,86 | 41,25±29,34 | -0,94 | 0,89 |
| Vision-specific dependency (VSD) | 53,98±34,64 | 53,98±33,44 | 0 | 1 | 40,94±24,87 | 43,73±26,97 | 2,79 | 0,69 |
| Driving (D) | Missing | Missing | - | - | Missing | Missing | - | - |
| Color vision (CV) | 52,27±39,27 | 66,54±38,84 | 14,27 | 0,13 | 65±31,83 | 68,75±33,32 | 3,75 | 0,66 |
| Peripheral vision (PV) | 47,73±30,77 | 63,64±31,55 | 15,91 | 0,007 | 45±34 | 53,75±27,24 | 8,75 | 0,18 |
Table 3: Changes in vision related quality of life pre visual rehabilitation and at 6 months after low vision aids provision in m
Control Group
The mean age of the twenty patients included in the control group was 78,5 (±8,2) years. There were no improvements in any of the measures (i.e., VFQ-25 items, reading performance, and fixation stability). The means and SDs for outcomes measures are shown in Table 4. Reading ability is the most frequent and important rehabilitation request and goal.
| Baseline | Follow up | p | |
|---|---|---|---|
| Mean (DS) | Mean (DS) | ||
| GH | 53,1 (± 20,2 | 53,8 (± 18,4) | >0,05 |
| GV | 32,7 (±10,5) | 32,5 (±9,8) | >0,05 |
| OP | 64,5 (±20,7) | 67,8 (± 21,6) | >0,05 |
| NA | 35,1 (± 21,9) | 32,6 (±19,1) | >0,05 |
| DA | 21,2 (±23,7) | 31,9 (±18,4) | >0,05 |
| Vssf | 43,7 (±21) | 45 (±19) | >0,05 |
| Vsmh | 39,5 (± 20,7) | 40,1 (± 22) | >0,05 |
| Vsrd | 46,6 (±18,5) | 49,6 (±19,8) | >0,05 |
| Vsd | 47,1 (± 29,8) | 44,8 (±29,1) | >0,05 |
| D | 0 | 0 | >0,05 |
| CV | 63,1 (± 33,7) | 58,3 (±37,3) | >0,05 |
| PV | 17,5 (± 25,7) | 21,4 (±26,1) | >0,05 |
Table 4: VFQ-25 scales pre visual rehabilitation and after 6 months from the provision of low vision device in control group.
Discussion
This study shows that our rehabilitation method could have effect for improving patients’ QoL. In particular, visually impaired subjects due to MD perceived a significant improvement in Near Activities such as reading. The main improvement was observed in “Near Activities”, which was indeed indicated by the patients as their main issue and request (Table 1, about 95% of patients put reading at the first place). In addition, the improvement was found to be significant even when dividing the population by gender, showing how the rehabilitation procedure overcomes the cultural differences underlying gender differences. Given that, in VFQ25, results related to reading speed are included the NA variable (Near Activities). We performed a specific test (speed of reading) to make sure that reading was indeed one of the aspects of the patient’s profile that had improved after rehabilitation. As shown in Figure 4, a positive correlation was found between NA and words read per minute, whereas a negative correlation was found between age and effectiveness considered as a whole (Figure 3). This result is yet another indication in favor of the fact that our procedure of rehabilitation, centering on the demands of the patient, is able to decrease the systemic effects having a negative impact on the rehabilitation itself. In our study, the holistic approach was found to play a major role in influencing the obtained result. Moreover, for control group who refused to attend psychological counseling and support, no enhancement of PROMs was detected.
As shown in several previous studies [21, 22], the difficulties reported in most daily activities by maculopathy patients depend on factors such as depression, compensative strategies used, cognition and personality. In particular, one study argued that personality traits such as neuroticism, defined as the tendency to experience more negative and distressing emotions as a result of adverse events in comparison to others in the same conditions, influences the perception of their own functional vision. The above mentioned findings, along with others studies [23, 24], show that the presence of an anxiety-depressive disorder, developing as a result of the ocular pathology, is an obstacle to rehabilitation and negatively affects the perception of QoL, i.e. the score of VFQ25 questionnaire. In our study, the use of our rehabilitation procedure is followed by a different outcome, since VFQ25 scores are not affected by the presence of emotional disorders, which remain present during the entire follow-up period [25].
Through the clinical interview, the psychologist assesses personality traits, emotionally supports the patient, providing help to restructure its self-concept, to overcome an eventual crisis (a real grief process), to reshape expectations and interests as well as relationships in order to achieve the highest level of independence and adaptation. The psychologist indeed helps the visually impaired to become aware of its condition; to recognize and use the individual and familiar resources in order to cope with its disease and deal with the possible evolution of the disease; to develop new skills and psychological relationships; to manage stress reactions; to reinforce self-image, making it acceptable to the patient through positive reinforcement, and to accept aids. Thus, this peculiar approach can have a positive impact on increasing the accuracy of rating scales of functional vision and suggesting new rehabilitative interventions to improve the patients’ functional vision and QoL.
Conclusion
The holistic approach allows caring for a person with visual impairment as a whole, especially supporting a better perception of the quality of life. Indeed, we observed that the perception of improvement, as compared to the activity, is not associated to an actual increase in reading speed. Although the concept of emotional support as an integral part of visual rehabilitation is now supported by many studies [26, 27], the number of studies actually evaluating the effectiveness of this support is still limited [28]. Therefore, as suggested the literature, fundamental research and effective valid assessment tools are needed in order to improve medical care, providing also clinicians with the effectiveness of psychological and medical outcomes related to problems associated with visual impairment. Some limitations of the study should be considered. First of all, in view of the small number of patients included in the study, we suggest researchers to conduct additional trials on this topic. Research for identifying better rehabilitative approaches and enhancing QoL for visually impaired subjects are needed.
References
-
Wagner M, Rietz C, Kaspar R, Janhsen A, Geithner L, et al. (2017) Quality of life of the very old: Survey on quality of life and subjective well-being of the very old in North Rhine-Westphalia (NRW80+). Journal of Gerontology and Geriatrics 51(2): 193-199.
-
Jacelon CS (2007) Older adults’ participation in research. Nurse Res 14(4): 64-73.
-
Aaronson NK (1988) Quality of life: what is it? How should it be measured?. Oncology 2(5): 69-76.
-
(2019) World report on vision. World Health Organization.
-
Dell’Osbel (1996) Introduction. The condition of the blind: medical-epidemic and social welfare aspects. In: Calati D (Eds.), Seeing with the mind. Knowledge, affectivity, adaptation in the blind. Franco Angeli Milan.
-
Van der Aa HP, Hoeben M, Rainey L, Rens GH, Vreeken HL, et al. (2015) Why visually impaired older adults often do not receive mental health services: the patient’s perspective. Qual Life Res 24(4): 969-978.
-
Cimarolli VR, Casten RJ, Rovner BW, Heyl V, Sorensen S, et al. (2016) Anxiety and depression in patients with advanced macular degeneration: current perspectives. Clin Ophthalmol 10: 55-63.
-
Moschos, M, Nitoda E, Lavaris A (2016) Estimation of depression prevalence in patients with Stargardt disease using PHQ-9 and Zung scores. Eur J Ophthalmol 26(3): 268-272.
-
Choi HG, Lee MJ, Lee SM (2018). Visual impairment and risk of depression: A longitudinal follow-up study using a national sample cohort. Sci Rep 8(1): 2083.
-
Sheikh S, Dahiya S, Ansari AH, Kumar MM (2019) The association of quality of life between anxiety and depression in patients with chronic rheumatic heart disease. Mediterranean Journal of Clinical Psychology 7(2): 1-12.
-
Mangione CM, Lee PP, Gutierrez PR, Spritzer K, Berry S, et al. (2001) Development of the 25-item National Eye Institute Visual Function Questionnaire. Arch Ophthalmol 119(7): 1050-1058.
-
Markowitz SN (2006) Principles of modern low vision rehabilitation. Can J Ophthalmol 41(3): 289-312.
-
Binns AM, Bunce C, Dickinson C, Harper R, Edwards RT, et al. (2012) How effective is low vision service provision? A systematic review. Surv Ophthalmol 57(1): 34-65.
-
Grant P, Seiple W, Szlyk JP (2011) Effect of depression on actual and perceived effects of reading rehabilitation for people with central vision loss. J Rehabil Res Dev 48(9): 1101-1108.
-
Renieri G, Pitz S, Pfeiffer N, Beutel ME, Zwerenz R (2013) Changes in quality of life in visually impaired patients after low-vision rehabilitation. Int J Rehabil Res 36(1): 48-55.
-
Cimarolli VR, Boerner K, Ing MB, Reinhardt JP, Horowitz A (2012) Challenges faced by older adults with vision loss: a qualitative study with implications for rehabilitation. Clin Rehabil 26(8): 748-757.
-
Heesterbeek TJ, Van der Aa HPA, Van Rens GHMB, Twisk JWR, Nispen RMA (2017) The incidence and predictors of depressive and anxiety symptoms in older adults with vision impairment: a longitudinal prospective cohort study. Ophthalmic Physiol Opt 37(4): 385-398.
-
Rossi GCM, Milano G, Tinelli C (2003) The Italian Version of the 25-Item National Eye Institute Visual Function Questionnaire: Translation, Validation, and Reliability. J Glaucom 12(3): 213-220.
-
Horowitz A, Reinardt JP, Kennedy GJ (2005) Major and subthreshold depression among older adults seeking vision rehabilitation service. Am J Geriatr Psychiatry 13(3): 180-187.
-
Clemons TE, Rankin MW, Mcbee WL (2006) Cognitive impairment in the Age-Related Eye Disease Study: AREDS report no. 16. Arch Ophtalmol 124(4): 537-543.
-
Whitson HE, Witaker D, Sanders LL, Potter GG, Cousins SW, et al. (2012).Memory deficit associated with worse functional trajectories in older adults in low-vision rehabilitation for macular disease. J Am Geriatr Soc 60(11): 2087-2092.
-
Rovner BW, Casten RJ, Hegel MT, Massof RW, Leiby BE, et al. (2014) Personality and Functional Vision in Older Adults with Age-Related Macular Degeneration. Journal of Visual Impairment & Blindness 108(3): 187-199.
-
Brody BL, Gamst AC, Williams RA, Smith AR, Lau PW, et al. (2001) Depression, visual acuity, comorbidity, and disability associated with age-related macular degeneration. Ophthalmology 108(10): 1893-1900.
-
Rovner BW, Casten RJ, Massof W, Leiby BE, Tasman WS (2011) Psychological and Cognitive Determinants of Vision Function in Age-Related Macular Degeneration. Arch Ophthalmol 129(7): 885-890.
-
Kupfer C (2000) The National Eye Institute’s low vision education program: improving quality of life. Ophthalmology 107(2): 229-230.
-
Barr W, Hodge S, Leeven M, Bowen L, Knox P (2012) Emotional support and counselling for people with visual impairment: Quantitative findings from a mixed methods pilot study. Counselling & Psychotherapy Research 12(4): 294-302.
-
Hodge SB, Bowen W, Leeven L, Knox P (2013) Exploring the role of emotional support and counselling service for people with visual impairments. British Journal of Visual Impairment 31(1): 5-19.
-
Neyman SR, Gosney MA, Victor CR (2010) Psychosocial impact of visual impairment in working-age adults. Br J Ophtalmol 94(11): 1427-1431.
- Systematic Review and Meta-analysis Investigating the Prevalence of Depression, Anxiety, Loneliness and Help seeking among International Students
- Family Experiences and their Interpretations as a Source of Adaptive Behaviour in Young Adults: A Qualitative Model of Adaptive Behaviour
- The Development of Responsibility in Teenage Mothers: A Qualitative Model
- Post-Truth Reality: Worldwide Infodemia and Mental Health Concerns during and Post COVID-19 Pandemic Scenarios
- Psycho-Emotional Rehabilitating Means of Overcoming Extreme and Stressful Impact
- The Paradox of Humbleness, Arrogance and the Concept of Fluid Individuality