Drug Abuse & Cognitive Functioning
Extensive research has been conducted on cognitive impairments in substance use disorders, particularly with the advancements in cognitive and computational neuroscience as well as neuroimaging techniques over the past two decades. It has been noticed that, impaired cognition functioning is the common factor in person with substance abuse most precisely in case of attention, memory, recalling, decision making etc. Addiction has been showing basic impairment in brain and brain related processes through improper regulation and decreasing motivation and development of apathy. This special issue addresses cognitive impairment as a trans-diagnostic domain, highlighting the potential benefits of advancing the understanding and treatment of cognitive dysfunction in substance use disorders for various psychiatric conditions. In line with this overarching objective, we provide a summary of current findings in the fore mentioned cognitive domains of substance use disorders. Additionally, we propose an expansion of the scope to encompass precognition and social cognition, which are often overlooked but hold significant relevance to substance use disorders. While these two areas have received comparatively less attention, they are essential aspects of substance use disorders both phenomenologically and in other respects. The review concludes by suggesting avenues for further research and potential therapeutic interventions targeting both the well-established cognitive domains and this more comprehensive understanding of cognitive impairments associated with substance use disorders.
Introduction
Cognitive changes and impairments observed in substance use disorders play a significant role in the substantial public health burden associated with these disorders [1]. The spectrum of drug and alcohol use among individuals ranges from non-pathological to diagnosable mental health disorders according to the Diagnostic and Statistical Manual of Mental Disorders (DSM) [2, 3]. In this discussion, we focus on cognitive alterations that are already indicative of a disorder related to drug use. This type of drug use can be defined as a “pathological pattern of behaviors” characterized by compulsive and persistent drug use, impaired control, continuation despite negative consequences, craving, tolerance, and withdrawal [4, 5]. The cognitive domains typically involved in addiction include attention, response inhibition, decision-making, and working memory.
A recent frame work called the Research Domain Criteria (RDoC), initiated by the National Institutes of Health, provides a systemic conceptual approach to neuroscience. RDoC considers mental processes and disorders in terms of disruptions along the continuum from normal to pathological, encompassing various psychological processes and behavioral functions [6]. This approach is gaining recognition and is increasingly used in research. RDoC is applied across the normal-pathology continuum for the specific domain or construct under investigation, allowing a departure from categorical diagnoses [7].
The application of the RDoC framework to substance use disorders has gained attention [8]. Three domains relevant to addiction have been identified: executive function, incentive salience, and negative emotionality [9]. These domains correspond to different stages in the addiction cycle and contribute concurrently to addiction and relapse vulnerability. They can be measured across various substance use disorders. In this review, we focus on the executive (cognitive) domain and provide an overview of impairments that could serve as intermediate phenotypes for interventions targeting behavior, pharmacology, or neuro stimulation (Figure 1) [10].
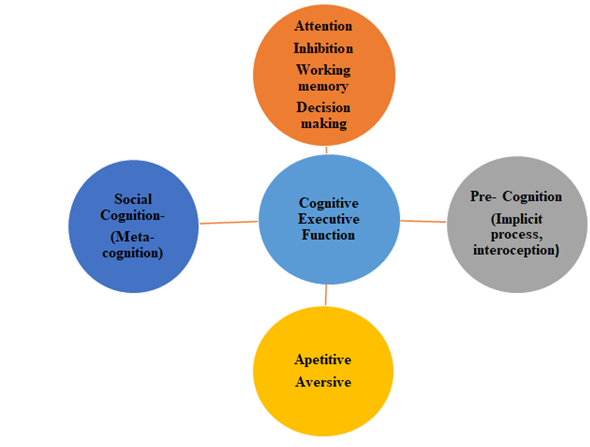
Figure1: Figure depicting research domain criteria of addiction.
This overview suggests an expansion of the established cognitive domains in substance use disorders to include two additional domains:
- Precognition, which encompasses processes occurring outside or before conscious cognition, and
- Social cognition, which includes metacognition/insight and theory of mind (ToM). These extended domains may be crucial components of the addiction phenotype in humans and could potentially hold the key to understanding the challenging treatment and functional impairments associated with substance use disorders.
There are several models that indicate cognitive impairment that arises both ways due to addiction or as drug abuse. One such model, proposed by Goldstein and Volkow, focuses on disrupted cortical top-down processes resulting from dysfunction in the prefrontal cortex (PFC). This dysfunction leads to impaired response inhibition and altered salience attribution, reducing the ability to modify behavior related to drugs and drug cues [11]. Other models, including Monterosso J, et al. [12] concept of impulsive choice as a hyperbolic function, describe impulsive behaviors as a breakdown of cognitive self-control mechanisms. Bickel WK, et al. [13] further expanded on this model and applied it specifically to addiction, demonstrating that individuals with addiction exhibit greater discounting of delayed rewards compared to healthy controls [14]. Sofuoglu M, et al. [15] proposed a dual-process model, highlighting the interplay between “top-down” and “bottom-up” processes in controlling behavior [14]. They argue that heightened implicit and automatic neurobiological processes increase the risk of drug use and relapse, while impaired executive top-down processes in individuals with addiction are responsible for regulating these downstream automatic processes.
Attention
In addition, there is a notable bias towards directing attention to drugs and drug-related cues [15, 16, 17]. This
attentional bias is often implicit and occurs automatically [18]. Some researchers propose that drug-related cues acquire positive incentive properties through classical conditioning, while others suggest that negative emotions enhance the salience of drug-related cues [19]. Both processes contribute to the facilitation of drug-seeking behaviors. Once established, attentional bias drives drug seeking by shifting the salience towards drug-related cues and directing behavioral resources towards the goal of drug consumption [20, 21].
Several tasks are employed to measure attentional bias. The Stroop interference task, for instance, requires individuals to name the font color of words, and interference arises when the word content differs from the font or carries emotional significance (such as drug-related words), leading to slower reaction times [22]. Generally, individuals using nicotine, cocaine, heroin, cannabis, and alcohol exhibit slower reaction times when confronted with words associated with their respective substance use disorders [23, 24, 25, 26]. Visual attention tasks also reveal quicker reaction times towards drug-related stimuli, indicating an attention-driven approach [27]. Tasks employing a “joystick” procedure have been utilized to measure approach or avoidance responses to explicit or implicit drug-related cues [28, 29].
Researchers have started using these tasks to modify attentional biases, aiming to reduce drug use [30]. Attentional bias modification training has shown some success in reducing bias towards alcohol cues but has had limited success with cocaine cues [31, 32]. The field is actively investigating the most effective methods to modify attentional bias towards substance-related cues and how to translate these modifications into clinical outcomes [33, 34].
The modest results achieved so far highlight the entrenched nature of attentional bias towards drug-related cues and underscore their potential significance as a target for treatment [35, 36, 37].
Response Inhibition
Loss of control over drug use is a defining characteristic of addiction4. Inhibitory control refers to the ability to suppress or counter responses, including behaviors, thoughts, or motivational states. Impairments in inhibitory control are believed to underlie the difficulty in resisting the powerful allure of drugs, thus increasing the risk of relapse [38, 39, 40, 41]. Poor inhibitory control is also associated with various behavioral patterns commonly observed in substance use disorders, such as increased impulsivity, sensation seeking, risk-taking, and poor decision-making [42].
Neuropsychological and neuroimaging studies have identified the prefrontal cortex (PFC) as the key region involved in inhibitory control. The PFC exerts top-down regulation over downstream motivational systems associated with drugs and natural rewards [43].
Variability in the ability to inhibit impulses and delay gratification is evident across individuals, even before any drug exposure. However, chronic exposure to certain drug classes, particularly stimulants, can undermine this “braking ability” of the brain [44, 45, 46]. Common tasks used to assess inhibitory control involve instructed attempts to inhibit a propotent motor response. For example, the “go/no-go” task requires rapid button presses to “go” stimuli while withholding the response to infrequent “no-go” stimuli [47]. Poor performance in these tasks is correlated with higher-order failures of inhibition and is associated with drug relapse. Some tasks incorporate valences stimuli to capture real-world inhibition challenges, where inhibition of approach to positive stimuli is required. Laboratory models that involve inhibiting craving to drug- related cues closely resemble the challenges faced by individuals in recovery [48].
Neuroimaging studies have shown reduced recruitment of top-down inhibitory regions in drug users compared to controls during simple laboratory tasks of inhibition, particularly in stimulant users [49]. Notably, cocaine patients who achieve extended abstinence demonstrate enhanced recruitment of cognitive control regions, suggesting potential recovery of inhibitory ability with abstinence or that individuals with strong inhibitory ability are more likely to achieve abstinence. Longitudinal studies are needed to further explore these possibilities [50, 51, 52].
Efforts to improve inhibitory function through medication targeting frontal circuitry or direct neural stimulation are still in early stages but offer promising prospects for targeted interventions [53]. Enhancing inhibitory control holds clinical significance as an intermediate phenotype for targeted interventions in addiction [54, 55, 56].
Working Memory
Working memory, as defined by Baddeley, is a system responsible for the temporary maintenance and manipulation of information crucial for complex cognitive tasks like comprehension, learning, and reasoning [57]. It consists of three subsystems: the phonological loop, which handles verbal and acoustic information; the visuospatial sketchpad, which deals with visual information; and the central executive, a capacity-limited control system that allocates and actively manipulates resources [58].
Various tasks have been used to measure working memory, such as n-back tasks, visuospatial tasks, digit and word recall, and verbal memory [59]. Studies have revealed cognitive deficits in individuals with substance use disorders using these tasks [60]. Working memory impairments may be associated with the chronic toxic effects of drug use, and lower executive cognitive ability has been linked to an increased susceptibility to problematic drug use [61]. Therefore, targeting working memory could be a therapeutic approach in substance use disorders and potentially improve functional outcomes. Strengthening the central executive subsystem of working memory through retraining may also benefit other cognitive functions [62, 63].
Addiction researchers have started focusing on working memory as a means to enhance cognitive control [64]. Some studies have used working memory training programs, involving tasks like verbal memory and recall of numbers and words, to improve working memory in individuals with stimulant use disorders [65]. While improvements in delay- discounting were observed, working memory enhancements were not consistent. In individuals with alcohol use disorders, working memory training has been associated with reduced alcohol use and improved working memory performance [66].
Another rationale for targeting working memory in addiction is its connection to dopaminergic mechanisms, which play a central role in addiction [67]. Working memory capacity relies on dopaminergic mechanisms, and working memory training has been shown to influence dopamine systems. When behavioral interventions alone are insufficient, pharmacological approaches that optimize dopaminergic function could serve as facilitation tools [68]. Accumulated evidence suggests that psychoactive drugs can compensate for working memory impairments, thus supporting functional restoration and the goals of reducing drug use and achieving abstinence [69].
Decision Making Process
The characteristic of addiction often involves seemingly poor decision-making, where individuals continue to use drugs and alcohol despite experiencing negative consequences. Several theories attempt to explain why these “poor” choices persist [70]. The “somatic markers” theory proposed by Verdejo-Garcia suggests that individuals with addiction have reduced awareness of emotional warning signals from the body, leading to risky decision-making and a focus on immediate rewards rather than future consequences [71]. Bickel WK, et al. [13] emphasize cognitive impairment, which results in prioritizing immediate rewards over larger, delayed rewards [72].
These poor decisions arise from an imbalance between top-down (deliberative) and bottom-up (automatic) processing [73]. While top-down processing allows for flexible and value-sensitive decisions, it is slow and cognitively demanding [74]. On the other hand, automatic actions, driven by habits and conditioned behaviors, are fast but inflexible and insensitive to devaluation [75]. Initially, drug and alcohol use involves more deliberate decision- making, but with continued use, these actions become more automatic and eventually compulsive. The incentive salience of drug-related cues further contributes to this transition [76].
Various tasks are used to measure decision-making processes [77]. Delay-discounting tasks assess an individual’s ability to delay immediate gratification for a higher-value reward in the future. Individuals with addiction tend to discount larger, delayed rewards more than healthy controls, and higher rates of discounting are associated with disadvantageous behaviors, including drug use [78]. The Iowa gambling task evaluates real-time decision-making, and people with addiction generally perform worse than controls. Some addicted individuals may lack implicit interoceptive guidance toward a more advantageous strategy [79].
Researchers have employed different methods to restore the balance between top-down and bottom-up processing [80]. Working memory training has shown potential in strengthening the central executive subsystem, reducing discounting, improving working memory, and decreasing substance use [81]. Meditation has emerged as a promising approach to enhance executive control and increase awareness of internal states, potentially improving interception. Contingency management approaches offer a way to promote deliberative decision-making and reduce automatic drug-choice behaviors [82].
Pre-Cognition
Processes that occur rapidly and implicitly, even outside of conscious awareness, play significant roles in executive cognitive domains such as attention, inhibition, working memory, and decision-making [83]. These precognitive processes, shaded in blue in Figure 1, can be influenced by appetitive or aversive motivational states and may shape drug-related feelings and behavior without explicit awareness. In the domain of attention, the response to drug cues is fast, involuntary, and implicit due to prior associative learning. Individuals with substance use disorders may automatically attend to drug-related cues even when task performance requires shifting attention away from them. Inhibition tasks also involve precognitive processes, where deliberate attempts to inhibit pre potent responses (whether motor- or drug-related) depend on their near-automatic nature [84]. Working memory, the ability to maintain and update information, often occurs implicitly without conscious focus, despite experimental tasks instructing intentional recall. Decision-making involves a competition between fast, implicit, precognitive responses (e.g., immediate reward approach and discounting of future rewards) and slower, deliberative responses that consider future consequences [85, 86]. Balancing these processes is a challenge addressed by dual-process models of decision-making [87].
The implications for addiction treatment are noteworthy, as conventional cognitive behavioral interventions primarily target explicit cognitions and may not effectively address implicit processes. High relapse rates in substance use disorders might partially result from difficulty addressing the precognitive domain [88]. Attempts to change attentional biases to drug cues through behavioral interventions have shown modest success, while working memory training studies are still in early stages [89]. Pharmacologic interventions, on the other hand, offer promise for targeting precognitive processes. For example, atomoxetine has reduced attentional bias to cocaine cues, although clinical trials did not demonstrate clear benefit [90]. Naltrexone has shown improvement in modulatory circuitry recruitment during now-later decision-making tasks [91]. Baclofen, a GABAB agonist, has blunted mesolimbic activation triggered by cocaine cues presented outside of conscious awareness. Screening candidate medications’ impact on precognition through paradigms involving brief “unseen” drug cues complements conventional self-reports of conscious motivational states [92].
Interoception, the sense of one’s internal state, plays a unique role in the precognitive domain. It is based on bodily sensations reflecting changes in internal state or autonomic visceral responses [93]. These sensations can become associated with previously neutral cues through learning, guiding the organism toward reward or away from danger. Interoception has been implicated in addiction models, where impaired interoception for negative stimuli and heightened interoception for positive arousal from drug cues contribute to relapse vulnerability [94].
The anterior insula, implicated in interoceptive processing and emotional awareness, is clinically significant in addiction, as attenuated responses in the insula during decision-making predict relapse [95]. Therapeutic approaches targeting explicit awareness of internal states aim to enhance cognitive control. Innovative treatments such as real-time neurofeedback or direct brain stimulation targeting the insula highlight the potential of interoceptive processes as meaningful therapeutic targets in substance use disorders [96].
Humans possess the capacity to introspect, enabling us to comprehend the connection between ourselves and others, monitor our thoughts, and exercise control over them. These metacognitive abilities play a crucial role in decision-making [97]. However, impaired metacognition can have adverse effects, such as overconfidence in poor decisions or a lack of confidence in better alternatives [98].
Despite being a prominent and critical characteristic of addiction, the extent of metacognitive impairment in substance use disorders remains poorly investigated. Many researchers have observed discrepancies between self- reported experiences and actual behavior, low compliance with treatment, frequent relapses, impaired psychosocial functioning, and a lack of awareness regarding the necessity of treatment [99]. In 2015, over 21 million individuals aged 12 and older required treatment for substance use disorders, but only around 10% received it. Among the remaining individuals (approximately 19 million), merely 5% recognized the need for treatment [100]. Goldstein and colleagues have associated this impairment with dysfunction in neural circuitry [101]. Metacognition mechanisms are believed to reside in frontal brain structures like the rostral anterior cingulate cortex [102, 103], and ventrolateral prefrontal cortex dysfunction may contribute significantly to insight impairment [104].
Metacognition
Metacognitive deficits can be considered as impairments of insight, which are commonly observed in addiction [105, 106]. In the substance use disorder field, lack of insight is sometimes conflated with “denial,” but they are distinct. Denial involves refusing or contradicting something that one is aware of, while lack of insight refers to an absence of awareness regarding something present within the individual [107]. Mental health researchers differentiate between clinical insights, which encompass awareness of illness, recognition of the need for treatment, and relabeling symptoms, and impaired general insight, which is associated with poorer treatment outcomes, an inability to perceive illness severity, impaired psychosocial functioning, higher relapse rates, and low self-esteem [108]. The inability of individuals with substance use disorders to assess the severity of their impairments or even be aware of their disorder may explain the lack of perceived need for treatment. It should be noted that even after recognizing the need for help and seeking treatment, patients may still struggle and experience relapses, suggesting that self-awareness alone may not be sufficient for recovery [109].
Addiction has been observed to involve deficits in self-awareness and behavioral control, similar to other neuropsychiatric disorders (e.g., mood, psychotic, and neurological disorders) [110, 111]. The insight deficit is evident in one of the key characteristics of substance use disorders defined in the DSM classification: continued drug use despite negative consequences. Self-awareness deficits and metacognitive impairments persist even in individuals who have achieved remission from drug use, as demonstrated by their poor correlation between self-reported confidence in performance and actual performance on visuo-perceptual accuracy tasks [112].
Conclusion
This review provides an overview of cognitive impairments observed in drug and alcohol use disorders, considering a continuum ranging from precognitive processes to higher-level social cognition, with cognitive executive domains in between (Figure 1). The majority of research in the cognitive executive domain has focused on characterizing patients compared to controls and identifying differences in specific domains such as attention, response inhibition, working memory, and decision-making systems. Evidence is emerging for the status of each of these domains as intermediate phenotypes and potential targets for intervention. However, the translation of intermediate phenotypes to clinical outcomes is still in its early stages. Promising novel treatments like neuro stimulation and pharmacologic rebalancing offer potential for the next phase of translational research, particularly concerning cognitive deficits in substance use disorders. We propose a cognitive continuum wherein the less-studied extremes, namely precognition and social cognition, exhibit unique features (e.g., impaired interoception, metacognitive deficits, and impaired insight into illness) that could serve as viable therapeutic targets, necessitating the development of new interventions.
It is important to acknowledge the challenges in cross- sectional research when establishing whether cognitive impairments proceeded, predisposed to, exacerbated, or solely resulted from drug use. Longitudinal studies conducted in developmental cohorts prior to drug exposure will help determine the relative contributions of individual variables (e.g., genetics, epigenetics, and adversity) compared to drug variables (e.g., drug type, dose, exposure, frequency) to the observed impairments. This information is crucial for selecting therapeutic targets and setting realistic expectations regarding therapeutic outcomes, such as restoring function or providing remedial biological support.
Furthermore, it is worth noting that the phenotypic features arising from both familiar and extended cognitive domains are not exclusive to addiction but are dimensional and trans diagnostic, relevant to other neuropsychiatric disorders and conditions (as emphasized in the Research Domain Criteria framework). Hence, therapeutic discoveries in the addiction field may have direct implications for other major psychiatric disorders that share the dimensions of these cognitive impairments. Research in these domains will also help empirically determine the unique contributions of intermediate phenotypes compared to overall psychopathology (e.g., factor “p”) in guiding treatments and predicting clinical outcomes [113, 114].
References
-
Gould TJ (2010) Addiction and cognition. Addict Sci Clin Pract 5(2): 4-14.
-
Saha TD, Chou SP, Grant BF (2006) Toward an alcohol use disorder continuum using item response theory: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Psychol Med 36(7): 931-941.
-
Patrono E, Gasbarri A, Tomaz C, Nishijo H (2016) Transitionality in addiction: a temporal continuum hypotheses involving the aberrant motivation, the hedonic dysregulation, and the aberrant learning. Med Hypotheses 93: 62-70.
-
American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders, 5th (Edn.), American Psychiatric Publishing.
-
Koob GF, Volkow ND (2010) Neurocircuitry of addiction. Neuropsychopharmacology 35(1): 217-238.
-
Insel T, Cuthbert B, Garvey M (2010) Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry 167(7): 748-751.
-
O’Donnell P, Ehlers MD (2015) Opportunities for new drug development in psychiatry: a glass half-full. JAMA Psychiatry 72(11): 1067-1068
-
Kwako LE, Momenan R, Litten RZ, Koob GF, Goldman D (2016) Addictions neuroclinical assessment: a neuroscience-based framework for addictive disorders. Biol Psychiatry 80(3): 179-189.
-
Koob GF (2009) Neurobiological substrates for the dark side of compulsivity in addiction. Neuropharmacology 56(1): 18-31.
-
Goldstein RZ, Volkow ND (2011) Dysfunction of the prefrontal cortex in addiction: neuroimaging findings and clinical implications. Nat Rev Neurosci 12(11): 652-
-
Goldstein RZ, Volkow ND, Wang GJ, Fowler JS, Rajaram S (2001) Addiction changes orbitofrontal gyrus function: involvement in response inhibition. Neuroreport 12(11): 2595-2599.
-
Monterosso J, Ainslie G (1999) Beyond discounting: possible experimental models of impulse control. Psychopharmacology 146(4): 339-347.
-
Bickel WK, Marsch LA (2001) Toward a behavioural economic understanding of drug dependence: delay discounting processes. Addiction 96(1): 73-86.
-
Madden GJ, Petry NM, Badger GJ, Bickel WK (1997) Impulsive and self control choices in opioid-dependent patients and non-drug-using control participants: drug and monetary rewards. Exp Clin Psychopharmacol 5(3): 256-262.
-
SofuogluM, DeVito EE, Waters AJ, Carroll KM (2016) Cognitive function as a trans-diagnostic treatment target in stimulant use disorders. J Dual DIagn 12(1): 90-106.
-
Field M, Mogg K, Bradley BP (2006) Attention to drug- related cues in drug abuse and addiction: component processes. In: R.W.Wiers & A. W. Stacy (Edns.), Handbook of Implicit Cognition and Addiction. Thousand Oaks CA Sage, pp: 151-163.
-
Roberts W, Fillmore MT (2015) Attentional bias to alcohol-related stimuli as an indicator of changes in motivation to drink. Psychol Addictive Behav 29(1): 63- 70.
-
Anderson BA (2016) What is abnormal about addiction- related attentional biases?. Drug Alcohol Depend 167: 8-14.
-
Wetherill RR, Childress AR, Jagannathan K (2014) Neuralmresponses to subliminally presented cannabis and other emotionally evocative cues in cannabis- dependent individuals. Psychopharmacology 231(7): 1397-1407.
-
Field M, Cox WM (2008) Attentional bias in addictive behaviors: a review of its development, causes, and consequences. Drug Alcohol Depend 97(1-2): 1-20.
-
Stewart J, de Wit H, Eikelboom R (1984) Role of unconditioned and conditioned drug effects in the self- administration of opiates and stimulants. Psychol Rev 1984 91(2): 251-268.
-
Robinson TE, Berridge KC (2001) Incentive-sensitization and addiction. Addiction 96(1): 103-114.
-
Baker TB, Piper ME, McCarthy DE, Majeskie M Fiore MC (2004) Addiction motivation reformulated: an affective processing model of negative reinforcement. Psychol Rev 111(1): 33-51.
-
Leeman RF, Robinson CD, Waters AJ, Sofuoglu M (2014) A critical review of the literature on attentional bias in cocaine use disorder and suggestions for future research. Exp Clin Psychopharmacol 22(6): 469-483.
-
Cox WM, Fadardi JS, Pothos EM (2006) The addiction- Stroop test: theoretical considerations and procedural recommendations. Psychol Bull 132(3): 443-476.
-
Froeliger B, Modlin L, Wang L, Kozink RV, McClernon FJ (2012) Nicotine withdrawal modulates frontal brain function during nan affective Stroop task. Psychopharmacology 220(4): 707-718.
-
Munafò M, Mogg K, Roberts S, Bradley BP, Murphy M (2003) Selective processing of smoking-related cues in current smokers, ex-smokers and never-smokers on the modified Stroop task. J Psychopharmacol 17(3): 310- 316.
-
Rzetelny A, Gilbert DG, Hammersley J, Radtke R, Rabinovich NE, et al. (2008) Nicotine decreases attentional bias to negative-affect related Stroop words among smokers. Nicotine Tob Res 10(6): 1029-1036.
-
Pike E, Stoops WW, Fillmore MT, Rush CR (2013) Drug- related stimuli impair inhibitory control in cocaine abusers. Drug Alcohol Depend 133(2): 768-771.
-
Waters AJ, Marhe R, Franken IH (2012) Attentional bias to drug cues is elevated before and during temptations to use heroin and cocaine. Psychopharmacology 219(3): 909-921.
-
Waters AJ, Sayette MA, Franken IH, Schwartz JE (2005) Generalizability of carry-over effects in the emotional Stroop task. Behav Res Ther 43(6): 715-732.
-
Fadardi JS, Ziaee SS (2010) A comparative study of drug- related attentional bias: evidence from Iran. Exp Clin Psychopharmacol 18(6): 539-545.
-
Franken IH, Kroon LY, Wiers RW, Jansen A (2000) Selective cognitive processing of drug cues in heroin dependence. J Psychopharmacol 14(4): 395-400.
-
Field M (2005) Cannabis dependence and attentional bias for cannabis related words. Behav Pharmacol 16(5- 6): 473-476.
-
Cousijn J, Watson P, Koenders L, Vingerhoets WAM, Goudriaan AE, et al. (2013) Cannabis dependence, cognitive control and attentional bias for cannabis words. Addict Behav 38(12): 2825-2832.
-
Snelleman M, Schoenmakers TM, van de Mheen D (2015) Attentional bias and approach/avoidance tendencies do not predict relapse or time to relapse in alcohol dependency. Alcohol Clin Exp Res 39(9): 1734-1739.
-
Mogg K, Bradley BP, Field M, De Houwer J (2003) Eye movements to smoking‐related pictures in smokers: relationship between attentional biases and implicit and explicit measures of stimulus valence. Addiction 98(6): 825-836.
-
Field M, Mogg K, Bradley BP (2004) Eye movements to smoking-related cues: effects of nicotine deprivation. Psychopharmacology 173(1-2): 116-123.
-
Field M, Mogg K, Bradley BP (2006) Attention to drug- related cues in drug abuse and addiction: component processes. In: R.W Wiers & A. W. Stacy (Edns.), Handbook of Implicit Cognition and Addiction. Thousand Oaks CA Sage, pp: 151-163.
-
Jones BT, Bruce G, Livingstone S, Reed E (2006) Alcohol- related attentional bias in problem drinkers with the flicker change blindness paradigm. Psychol Addict Behav 2006 20(2): 171-177.
-
Wiers RW, Eberl C, Rinck M, Becker ES, Lindenmeyer J (2011) Retraining automatic action tendencies changes alcoholic patients’ approach bias for alcohol and improves treatment outcome. Psychol Sci 22(4): 490- 497.
-
Field M, Duka T, Eastwood B, Child R, Santarcangelo M, et al. (2007) Experimental manipulation of attentional biases in heavy drinkers: do the effects generalize?. Psychopharmacology 192(4): 593-608.
-
Schoenmakers T, Wiers RW, Jones BT, Bruce G, Jansen ATM (2007) Attentional re-training decreases attentional bias in heavy drinkers without generalization. Addiction 102(3): 399-405.
-
Schoenmakers TM, de BruinM, Lux IFM, Goertz AG, Van Kerkhof DHAT, et al. (2010) Clinical effectiveness of attentional bias modification training in abstinent alcoholic patients. Drug Alcohol Depend 109(1-3): 30- 36.
-
Mayer AR, Wilcox CE, Dodd AB (2016) the efficacy of attention bias modification therapy in cocaine use disorders. Am J Drug Alcohol Abuse 42(4): 459-468.
-
Wiers RW, Gladwin TE, Hofmann W, Salemink E, Ridderinkhof KR (2013) Cognitive Bias modification and cognitive control training in addiction and related psychopathology: mechanisms, clinical perspectives, and ways forward. Clin Psychol Sci 1(2): 192-212.
-
Smith JL, Mattick RP, Jamadar SD, Iredale JM (2014) Deficits in behavioural inhibition in substance abuse and addiction: a metaanalysis. Drug Alcohol Depend 145: 1-33.
-
Luijten M, Field M, Franken IH (2014) Pharmacological interventions to modulate attentional bias in addiction. CNS Spectr 19(3): 239-246.
-
Bornovalova MA, Daughters SB, Hernandez GD, Richards JB, Lejuez CW (2005) Differences in impulsivity and risk-taking propensity between primary users of crack cocaine and primary users of heroin in a residential substance-use program. Exp Clin Psychopharmacol 2005 13(4): 311-318.
-
Bornovalova MA, Lejuez CW, Daughters SB, Zachary Rosenthal M, Lynch TR (2005) Impulsivity as a common process across borderline personality and substance use disorders. Clinical Psychol Rev 25(6): 790-812.
-
Verdejo-Garcia A, Rivas-Perez C, Vilar-Lopez R, Perez- Garcia M (2007) Strategic self-regulation, decision- making and emotion processing in poly-substance abusers in their first year of abstinence. Drug Alcohol Depend 86(2-3): 139-146.
-
Patkar AA, Murray HW, Mannelli P, Gottheil E, Weinstein SP, et al. (2004) Pre-treatment measures of impulsivity, aggression and sensation seeking are associated with treatment outcome for African-American cocaine- dependent patients. J Addict Dis 23(2): 109-122.
-
Lejuez CW, Aklin WM, Jones HA (2003) The Balloon Analogue Risk Task (BART) differentiates smokers and nonsmokers. Exp Clin Psychopharmacol 11(1): 26-33.
-
Lejuez CW, Aklin WM, Zvolensky MJ, Pedulla CM (2003) Evaluation of the Balloon Analogue Risk Task (BART) as a predictor of adolescent real-world risk-taking behaviours. J Adolesc 26(4): 475-479.
-
Bechara A, Dolan S, Denburg N, Hindes A, Anderson SW, et al. (2001) Decision-making deficits, linked to a dysfunctional ventromedial prefrontal cortex, revealed in alcohol and stimulant abusers. Neuropsychologia 2001 39(4): 376-389.
-
Garavan H, Hester R, Murphy K, Fassbender C, Kelly C (2006) Individual differences in the functional neuroanatomy of inhibitory control. Brain Res 1105(1): 130-142.
-
Childress AR, Mozley PD, McElgin W, Fitzgerald J, Reivich M, et al. (1999) Limbic activation during cue-induced cocaine craving. Am J Psychiatry 156(1): 11-18.
-
Kaufman JN, Ross TJ, Stein EA, Garavan H (2003) Cingulate hypoactivity in cocaine users during a GO-NOGO task as revealed by eventrelated functional magnetic resonance imaging. J Neurosci 23(21): 7839-7843.
-
Mischel W, Shoda Y, Rodriguez MI (1989) Delay of gratification in children. Science 244(4907): 933-938.
-
Goldstein RZ, Volkow ND (2002) Drug addiction and its underlying neurobiological basis: neuroimaging evidence for the involvement of the frontal cortex. Am J Psychiatry 159(10):1642-1652.
-
Bjork JM, Momenan R, Hommer DW (2009) Delay discounting correlates with proportional lateral frontal cortex volumes. Biol Psychiatry 65(8): 710-713.
-
Garavan H, Kaufman JN, Hester R (2008) acute effects of cocaine on the neurobiology of cognitive control. Philos Trans R Soc Lond B Biol Sci 363(1507): 3267-3276.
-
Horn NR, Dolan M, Elliott R, Deakin JF, Woodruff PW (2003) Response inhibition and impulsivity: an fMRI study. Neuropsychologia 41(14): 1959-1966.
-
Robbins TW (2007) Shifting and stopping: fronto- striatal substrates, neurochemical modulation and clinical implications. Philos Trans Soc Lond B Biol Sci 362(1481): 917-932.
-
Dalley JW, Robbins TW (2017) Fractionating impulsivity: neuropsychiatric implications. Nat Rev Neurosci 18(3): 158-171.
-
Moeller SJ, Paulus MP (2018) toward biomarkers of the addicted human brain: using neuroimaging to predict relapse and sustained abstinence in substance use disorder. Prog Neuro psycho pharmacol Biol Psychiatry 80(Pt B): 143-154.
-
Casey BJ, Somerville LH, Gotlib IH (2011) Behavioral and neural correlates of delay of gratification 40 years later. Proc Natl Acad Sci USA 108(36): 14998-15003.
-
Goldman M, Ehrman RN, Suh JJ (2015) Brief report: Spiders-No, Puppies-Go introducing a novel Go NoGo task tested in inner city adolescents at risk for poor impulse control. J Adolesc 2015 38: 45-48.
-
Lam SC, Wang Z, Li Y, (2013) Wavelet-transformed temporal cerebral blood flow signals during attempted inhibition of cueinduced cocaine craving distinguish prognostic phenotypes. Drug Alcohol Depend 128(1-2): 140-147.
-
Spechler PA, Chaarani B, Hudson KE, Potter A, Foxe JJ, et al. (2016) Response inhibition and addiction medicine: from use to abstinence. Prog Brain Res 223: 143-164.
-
Garavan H, Ross TJ, Stein EA (1999) Right hemispheric dominance of inhibitory control: an event-related functional MRI study. Proc Natl Acad Sci USA 96(14): 8301-8306.
-
Luo X, Zhang S, Hu S (2013) Error processing and gender-shared and -specific neural predictors of relapse in cocaine dependence. Brain 136(4): 1231-1244.
-
Connolly CG, Foxe JJ, Nierenberg J, Shpaner M, Garavan H (2012) The neurobiology of cognitive control in successful cocaine abstinence. Drug Alcohol Depend 121(1-2): 45-53.
-
Bell RP, Foxe JJ, Ross LA, Garavan H (2013) intact inhibitory control processes in abstinent drug abusers (I): a functional neuroimaging study in former cocaine addicts. Neuropharmacology 82: 143-150.
-
Jacobson L, Javitt DC, Lavidor M (2011) Activation of inhibition: diminishing impulsive behavior by direct current stimulation over the inferior frontal gyrus. J Cogn Neurosci 23(11): 3380-3387.
-
Dunlop K, Hanlon CA, Downar J (2017) Noninvasive brain stimulation treatments for addiction and major depression. Ann NY Acad Sci 1394(1): 31-54.
-
Baddeley A (1992) Working memory: the interface between memory and cognition. J Cogn Neurosci 4(3): 281-288.
-
Baddeley AD, Hitch G (1974) Working Memory. In: Bower GH, 1st (Edns.), Psychology of Learning and Motivation. Oxford UK, Academic Press 8: 47-89.
-
Baddeley A (2003) Working memory and language: an overview. J Commun Disord 36(3): 189-208.
-
Bechara A, Martin EM (2004) Impaired decision making related to working memory deficits in individuals with substance addictions. Neuropsychology 18(1): 152-162.
-
Tomasi D, Goldstein RZ, Telang F (2007) Widespread disruption inmbrain activation patterns to a working memory task during cocaine abstinence. Brain Res 1171: 83-92.
-
Bickel WK, Yi R, Landes RD, Hill PF, Baxter C (2011) Remember the future: working memory training decreases delay discounting among stimulant addicts. Biol Psychiatry 69(3): 260-265.
-
Patterson F, Jepson C, Loughead J (2010) Working memory deficits predict short-termsmoking resumption following brief abstinence. Drug Alcohol Depend 106(1): 61
-
Yan WS, Li YH, Xiao L, Zhu N, Bechara A, et al. (2014) Working memory and affective decision-making in addiction: a neurocognitive comparison between heroin addicts, pathological gamblers and healthy controls. Drug Alcohol Depend 134: 194-200.
-
Goldstein RZ, Leskovjan AC, Hoff AL (2004) Severity of neuropsychological impairment in cocaine and alcohol addiction: association with metabolism in the prefrontal cortex. Neuropsychologia 42(11): 1447-1458.
-
Hester R, Lubman DI, Yücel M (2010) the role of executive control in human drug addiction. Curr Top Behav Neurosci 3: 301-318.
-
Houben K, Wiers RW, Jansen A (2011) Getting a grip on drinking behavior: training working memory to reduce alcohol abuse. Psychol Sci 22(7): 968-975.
-
Volkow ND, Fowler JS, Wang GJ, Baler R, Telang F (2009) Imaging dopamine’s role in drug abuse and addiction. Neuropharmacology 56(suppl 1): 3-8.
-
Cohen JD, Braver TS, Brown JW (2002) Computational perspectives on dopamine function in prefrontal cortex. Curr Opin Neurobiol 12(2): 223-229.
-
McNab F, Varrone A, Farde L (2009) Changes in cortical dopamine D1 receptor binding associated with cognitive training. Science 323(5915): 800-802.
-
Backman L, Nyberg L, Soveri A (2011) Effects of working memory training on striatal dopamine release. Science 333(6043): 718.
-
Sofuoglu M, DeVito EE, Waters AJ, Carroll KM (2013) Cognitive enhancement as a treatment for drug addictions. Neuropharmacology 64(1): 452-463.
-
Rosell DR, Zaluda LC, McClure MM (2015) Effects of the D1 dopamine receptor agonist dihydrexidine (DAR- 0100A) on working memory in schizotypal personality disorder. Neuropsychopharmacology 40(2): 446-453.
-
Joyce JN, Millan MJ (2005) Dopamine D3 receptor antagonists as therapeutic agents. Drug Discov Today 10(13): 917-925.
-
Verdejo-García A, Bechara A (2009) A somatic marker theory of addiction. Neuropharmacology 56(suppl 1): 48-62.
-
Van der Meer M, Kurth-Nelson Z, Redish AD (2012) Information processing in decision-making systems. Neuroscientist 2012 18(4): 342-359.
-
Everitt BJ, Robbins TW (2013) From the ventral to the dorsal striatum: devolving views of their roles in drug addiction. Neurosci Biobehav Rev 37(9 Pt A): 1946- 1954.
-
Hauser TU, Allen M, NSPN Consortium, Rees G, Dolan RJ (2017) Metacognitive impairments extend the perceptual decision making weaknesses in compulsivity. Sci Rep 7(1): 6614.
-
Teper R, Inzlicht M (2013) Meditation, mindfulness and executive control: the importance of emotional acceptance and brain-based performance monitoring. Soc Cogn Affect Neurosci 8(1): 85-92.
-
Lipari RN, Park-Lee E, Van Horn S ( 2016) America’s Need for and Receipt of Substance Use Treatment in 2015. The CBHSQ Report Rockville, MD Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration.
-
Goldstein RZ, Craig AD, Bechara A (2009) The neuro circuitry of impaired insight in drug addiction. Trends Cogn Sci 13(9): 372-380.
-
Moeller SJ, Fleming SM, Gan G (2016) Metacognitive impairment in active cocaine use disorder is associated with individual differences in brain structure. Eur Neuropsychopharmacol 26(4): 653-662.
-
Moeller SJ, Konova AB, Parvaz MA (2014) Functional, structural, and emotional correlates of impaired insight in cocaine addiction. JAMA Psychiatry 71(1): 61-70.
-
Van der Meer L, de Vos AE, Stiekema AP (2013) Insight in schizophrenia: involvement of self-reflection networks?. Schizophr Bull 39(6): 1288-1295.
-
Balconi M, Finocchiaro R, Campanella S (2014) Reward sensitivity, decisional bias, and metacognitive deficits in cocaine drug addiction. J Addict Med 2014 8(6): 399-406.
-
Brevers D, Cleeremans A, Bechara A (2014) Impaired metacognitive capacities in individuals with problem gambling. J Gambl Stud 2014 30(1): 141-152.
-
Amador XF, Davis AS (2004) Insight and Psychosis: Awareness of Illness in Schizophrenia and Related Disorders. Oxford University Press.
-
Orfei MD, Robinson RG, Bria P, Caltagirone C, Spalletta G (2008) Unawareness of illness in neuropsychiatric disorders: phenomenological certainty versus etiopathogenic vagueness. Neuroscientist 14(2): 203-222.
-
Orfei MD, Piras F, Banaj N (2017) Unrealistic self- overconfidence in schizophrenia is associated with left presubiculum atrophy and impaired episodic memory. Cortex 86: 132-139.
-
Moeller SJ, Bederson L, Alia-Klein N, Goldstein RZ (2016) Neuroscience of inhibition for addiction medicine: from prediction of initiation to prediction of relapse. Prog Brain Res 223: 165-188.
-
Barbato M, Liu L, Penn DL (2013) Social cognition as a mediator between neurocognition and functional outcome in individuals at clinical high risk for psychosis. Schizophr Res 150(2-3): 542-546.
-
Francesconi M, Minichino A, Carrión RE (2016) Theory of Mind as mediator variable between neurocognition and functioning im young individuals in treatment with secondary services for nonpsychotic disorders. Psychiatry Res 246: 415-420.
-
Kwako LE, Bickel WK, Goldman D (2018) Addiction biomarkers: dimensional approaches to understanding addiction. Trends Mol Med 24(2): 121-128.
-
Caspi A, Houts RM, Belsky DW (2014) The p factor: one general psychopathology factor in the structure of psychiatric disorders?. Clin Psychol Sci 2(2): 119-137.
- Systematic Review and Meta-analysis Investigating the Prevalence of Depression, Anxiety, Loneliness and Help seeking among International Students
- Family Experiences and their Interpretations as a Source of Adaptive Behaviour in Young Adults: A Qualitative Model of Adaptive Behaviour
- The Development of Responsibility in Teenage Mothers: A Qualitative Model
- Post-Truth Reality: Worldwide Infodemia and Mental Health Concerns during and Post COVID-19 Pandemic Scenarios
- Psycho-Emotional Rehabilitating Means of Overcoming Extreme and Stressful Impact
- The Paradox of Humbleness, Arrogance and the Concept of Fluid Individuality