Implementation of Setting-Wide Positive Behaviour Support in Adult Disability Settings: A Research Synthesis
Background: Positive behaviour support (PBS) is mandated under the Health Act 2007 as a recommended intervention for vulnerable adults experiencing distress in residential settings. There is limited investigation in effective implementation systems for this model of support. This paper provides a synthesis of the research exploring the use of a systemic model of PBS with adult populations. Methods: A systematic review of the literature was undertaken using COVIDENCE. The resulting studies were critically appraised using the quality assessment tool for reviewing studies with diverse designs (QATSDD) and were coded and analysed using an adapted version of the standard data extraction template on the Covidence platform. Results: Nine studies met the inclusion criteria and were published between 2003 and 2021 and are reported in respect to descriptive features, methodological rigour, treatment components, outcomes observed and recommendations for future research. Conclusions: There is a growing body of literature evidencing the efficacy of systemic applications of PBS in promoting quality of life outcomes and reducing problem behaviours and restrictive practices. However, few studies to date have focused on adult populations. The most frequently reported treatment component across the included studies was workforce development programmes. Recommendations for future research include scaling up of the interventions so that SWPBS might be applied regionally or nationally, with a view to embedding this culture into disability practice and building capacity across the state.
Introduction
behavioural sciences and integrated with knowledge from biomedical and systems-change strategies, focused on improving quality of life (QOL) and resolving problem behaviours. The PBS movement surfaced in the early 1980’s as the awareness of the human rights violations experienced by people living in institutional settings came to light, and the deinstitutionalisation movement gained momentum [2]. In parallel, significant developments in the field of behaviour modification were occurring, as numerous researchers worked to develop frameworks to guide the ethical use of techniques based on the principle of punishment, developed through research in institutions, for application in educational or community settings [3, 4, 5]. Renzaglia, et al. [6] highlighted the predicament confronting community and school-based practitioners of applying aversive practices involving the application of negative consequences with vulnerable individuals in their work settings [2]. This provided the motivation to identify socially acceptable, evidence and rights-based approaches for supporting people with complex needs and distressed behaviours, which often associated with the restrictive environments they lived in [2, 7, 8, 9]. However, not all contributors to the literature agreed that the use of aversive procedures needed review, leading to a defining conceptual rupture in the applied scientific community [2, 10].
Much of the early research on understanding the causes of aberrant behaviours originated in the educational and behavioural psychology disciplines [11, 12, 13]. This resulted in the significant development of fundamental technologies of PBS, functional analysis of behaviour [14] and functional assessment approaches [15, 16]. Researchers now had the means to explore more socially acceptable ways of modifying behaviour in the emerging culture of human rights and person centred values [2, 17].
By the late 1980’s, PBS emerged as a distinct discipline with a widespread base of practitioners, supporters and communities [18], leading to the publication of a professional periodical, the Journal of Positive Behavior Interventions, in 1999 and the establishment of an international association for PBS in 2003 [2]. Carr, et al. [19] published a seminal article describing the development of PBS and its foundations in the science of applied behaviour analysis (ABA), the normalisation movement and person-centred principles which it represented. The authors identified nine critical features of the model that have now become the blueprint for subsequent practice. These incorporate comprehensive lifestyle change and quality of life, stakeholder participation, systems change, multi-component interventions and numerous theoretical positions [19].
Various syntheses, meta analyses and textbooks describing the application of the model have been published [20, 21, 22, 23, 24, 25, 26, 27]. Generalisation in the application of PBS beyond disability practice is also evidenced with studies in forensic and mental health settings [28, 29]. With the growth in adoption of the model and available literature, advances have emerged in the implementation of PBS over the last two decades. A need for implementation models at larger units of analyses (e.g., classrooms, schools, day-service settings) to support wider populations while incorporating individualized supports also emerged [19]. Exploration of ecological constructs, large scale health psychology research and implementation science influenced the development of a distinct model of implementation within PBS [30].
Multi-Tiered Models of PBS
Trends in the literature leaned towards a focus on school- wide and system-wide models of intervention Turnbull, et al. [31] where components of PBS are stratified across three distinct tiers [18, 32]. Sugai, et al. [33] describe school or setting-wide PBS (SWPBS) as “a systems approach for establishing the social culture and individualised behavior supports needed for a school to be a safe and effective learning environment for all students” (p. 309). The authors summarise the defining characteristics of the approach as: a) Having a foundation in ABA and behavioural paradigms. b) Continuum of interventions focused on prevention and organised across three tiers of support. c) Focus on directly teaching adaptive and social behaviours to the whole population of the setting. d) Use of evidence-based practices within the multi- component treatment design. e) Adoption of a systems perspective by establishing local capacity and proficiency, organisational assurances, large implementation readiness, fidelity, and evaluation; and f) Data driven decision making.
Syntheses of the literature on school wide models of PBS provide a strong evidence base for the positive impact of this model of support [27, 34, 35]. However, there appears to be little consideration of the future supports for participants when they progress from educational or childcare settings, as there is a scarcity of literature to date examining the implementation of SWPBS outside of educational facilities, or with adult populations [21, 36]. Simonsen, et al. [37] suggest several strategies to extend evidenced systemic practices into alterative settings, however few researchers have examined this. With the progression of de-institutionalisation across the globe, there is a need to gain a greater understanding of the implementation of systemic models of support in community-based settings for adult populations.
To our knowledge, there has been no attempt to synthesise the extant literature examining the implementation of SWPBS in adult settings. Previous syntheses concerning SWPBS have focused on educational settings [34, 35]. While there are several syntheses examining PBS that include adult populations, these focus on staff training [23, 24] and staff perceptions of the paradigm [22], and not on setting wide applications. The aim of this systematic review is to evaluate the literature concerning the implementation of SWPBS with adult populations with regards to: a. Descriptive features, b. Methodological rigour, c. Treatment components, d. Outcomes observed and, e. Recommendations for future research.
Methods
Search Procedures
A broad search strategy was adopted due to the paucity of research in the use of a systemic model of PBS with an adult population. Relevant articles were identified by conducting comprehensive searches of Academic Search Complete, CINAHL, Embase, ERIC, Medline, PsychoInfo Articles, Social Sciences and Web of Science in May 2021. Searches were completed by inputting system* OR setting* OR train* OR implement* OR tier* OR “multi-tiered system of support” OR adopt* OR organi?ation* AND “positive behavio?r*” OR behavio* N3 (challenging OR intervention*). In addition to the database searches, the reference lists of all eligible studies were reviewed for relevant articles to increase the scope of the search. Identified articles were uploaded to Covidence (www.covidence.org) for screening and data extraction.
Inclusion and Exclusion Criteria
Studies were included that described outcomes of a systemic PBS intervention with adults. Criteria for inclusion in the review were:
(a) an adult participant group (18 years or above); (b) the use of a setting-wide, whole organisation or multi- tiered model of positive behaviour support intervention; (c) original research published in an English language peer- reviewed journal and, (d) Publication year of 2000 to 2021. If the authors described the intervention or treatment as PBS this was accepted References to multiple tiers of support, systemic interventions, or descriptions of interventions that corresponded with the components of systemic PBS were accepted as indicators of a systemic PBS model. Articles were excluded if they did not describe an intervention with outcomes (e.g., conceptual studies) of if the term “positive behaviour support” was not used within the article. Diversity in research design was an important feature of the synthesis, and is a well- established approach in health service research [38, 39]. The inclusion of qualitative, quantitative and multi-methods research serves to enhance and deepen understanding of multi-tiered complex interventions [39, 40].
Included and Excluded Studies
Five of the included studies referred to a systemic model of PBS in the title [41, 42, 43, 44, 45]. In the remaining four included articles, two described this in the abstract [46, 47] and two referred to systemic approaches in the methods [48, 49].
There was considerable variation in how the systemic nature of the intervention was described. For example, Fuchs, et al. [48] stated that “Systemic approaches would view “behaviour that challenges” in the context of a person’s life and their relationships” (p.135), whereas Higgins [47] described “PBS interventions at multiple levels of the organisation” (p.42). Riding [49] did not use any of these terms in the description of the intervention. Rather this article was included as the components of the intervention tallied with identified elements of a systemic model of PBS. Some studies described features of systemic PBS, but as a future consideration rather than a treatment component so were excluded from the review [50, 51]. MacDonald, et al. [52] used a tiered or “cascade approach to implementing PBS” (p. 2), but the article focuses specifically on the introduction of staff training programme with a goal of developing PBS plans (PBSP) so was ultimately excluded. Finally, Denne, et al. [53] highlighted the importance of embedding PBS across multiple systems, but this article was an exploratory narrative so excluded.
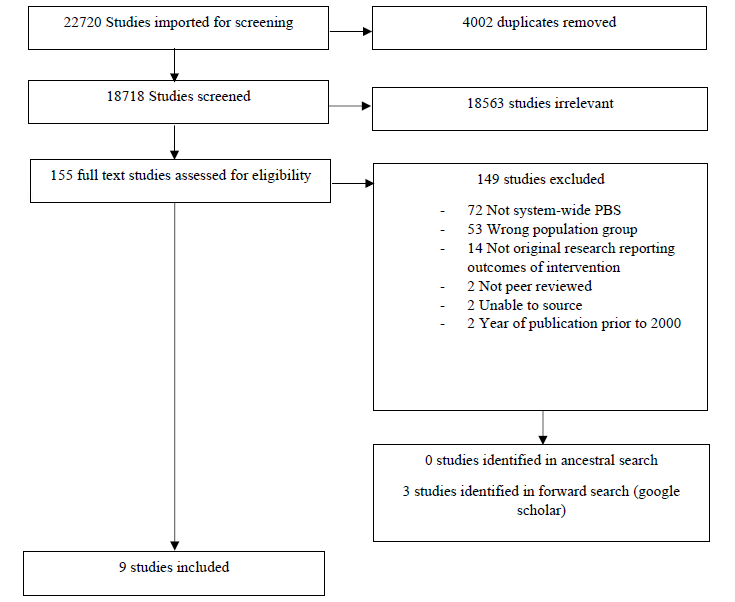
A total of 22720 articles were identified during the initial online database search. When duplicates were removed a total of 18563 articles remained. The abstracts of the studies were screened using the full eligibility criteria by means of the online platform Covidence [54]. A total of 155 articles were identified for full text review, with an additional 3 studies identified through reference searches and forward searches using google scholar. Two reviewers completed the full text review, and 6 studies were identified for inclusion in the synthesis (see Figure 1 for PRISMA diagram of the search procedure).
Article Coding
A data extraction template was developed based on the standardised format in Covidence [54] and adapted to include information potentially relevant to the goals of the review with a view to reducing post hoc selection biases [55]. The Quality Assessment Tool for Studies with Diverse Designs (QATSDD) was employed to critically appraise the quality of the included studies [56, 57]. This is a 16-item instrument specifically developed to evaluate the quality of research that is included in multiple methodological syntheses. The tool focuses on the congruency, clarity and structure of the reported research procedures over 16 evaluative indicators that are measured on a 4-point Likert scale. Fenton, et al. [56]. Each paper is given an overall quality score. Quality scores of all included studies are then totalled and calculated as a percentage of the maximum possible score. The instrument shows good reliability and validity in the critical appraisal of a multiplicity of studies and has been used in more than 80 systematic reviews to date [39].
Interrater Reliability
Identified articles were examined for inclusion against the stated inclusion criteria by the first author. Initially, inter- rater reliability was assessed during the full text screening of identified studies. Approximately 16% (n= 25) of the studies were reviewed by a second rater to determine IRR for inclusion. These studies were arbitrated to be included, excluded or uncertain by the second rater. Initial IRR was calculated as 68%. Any uncertainties or disagreements were deliberated by the reviewers, based on the stated inclusion and exclusion criteria, until a consensus was reached. Subsequently, IRR for inclusion of studies was calculated as 100%. Data in all included studies were extracted and assessed by the first author and an independent second rater. An agreement between authors was scored for instances of exact agreement on quantitative items (e.g., number of participants) or total agreement for conceptual items that involved some interpretation from the coder (e.g., how treatment components were selected). Agreement for data extraction was calculated as 98% and agreement for quality assessment as calculated as 96%. All instances of disagreement were discussed by the coders and a final code was reached by consensus.
Results
A total of nine studies met the inclusion criteria and were published between 2003 and 2021. Table 1 summarises the general information, participant and study characteristics, and intervention outcomes of the identified studies.
| Study | N | Design | Measures/Data Collection Tools | Interventions | Outcomes | Limitations |
|---|---|---|---|---|---|---|
| Allen D, Kaye N, Horwood S, Gray, D. & Mines S. | Not specified | Case Report | Periodic Service Review; Behaviour Monitoring Forms | Optimum physical environments, active support, management development programme, service development projects, staff emotional support | Reduction in overall use of physical interventions across settings | No reliability checks, population not static, no data on collateral changes, non-experimental, no data on staff, no statistical analysis |
| Evans R, Evans L & Rodgers T | 114 staff 178 adults with ID | Case Report | Supervisor observation, supervisory check sheets, routine incident reports, social validity survey | Brief positive interactions/meaningful interactions, supervisory checks of implementation fidelity, feedback to DSP’s, training for DSP and supervisors, programme embedded in organisational manuals and policies, regular update emails, agenda item at regular staff meetings, reinforcement for staff (pizza party) and supervisors (slushie) | Increases observed in implementation fidelity across settings for both DSP and supervisors. Decreases in challenging behaviour. Self reports indicated greater confidence, relationships with individuals supported and acceptance of the programme – however also resource intensive (time) | Some staff struggled to reach fidelity targets, retrospective analysis – no experimental controls, no reliability checks for incident reports, no statistical analysis of outcomes to determine significance |
| Freeman R, Smith C, Zarcone J, Kimbrough P, Tieghi-Benet M, Wickham D, Reese M & | 11 staff | Case Report | Pre-post training fidelity measures for PBSP’s and PCP’s completed, PBSP/ PCP ‘s in place prior to professional involvement, measures of problem behaviour, adaptive behaviour and quality of life, The Self Assessment of Contextual Fit Survey, The Person- Centred Planning Process Satisfaction Survey | Facilitator training in PBS/PCP comprising of online instruction, field based activities, portfolio development and resource toolbox over a 1 year period, online resources and instruction, expert support for organisation-- wide and state-wide PBS planning processes | Increase in PBSP and PCP fidelity scores completed by professionals in training, 11 facilitators completed training. Organisation-wide and state- wide planning model including residential setting support and family support described in report | Data was still in the process of being collected at the time of publication so incomplete, no statistical analysis of outcomes though the planned analysis is described |
| Fuchs K & Ravoux P | 14 adults with ID | Naturalistic pre- post intervention evaluation and a qualitative study | Quarterly reports, Health of the Nation Outcome Scales for people with Learning Disabilities, Behaviour Problems Inventory, Guernsey Community Participation and Leisure Assessment | PBS, systemic approaches, speech and language therapy, specialist nursing assessments interventions and health facilitation, advanced practitioner support for allocated social workers, person/family centred partnership approach, training and formulation workshops, care coordination risk management and care planning via systemic network meetings, sustainable capable environments in locality | Clinical outcomes include improvement in overall wellbeing, behaviours, health outcomes and adaptive function. Sizable reductions in financial costs were observed. Qualitative feedback indicated that clinical leadership, coordination of MDT input, responsiveness and family/person centred partnership approaches were most valued by the individuals supported. Further outcomes included successful transitions and prevention of service breakdown, development of capable environments in the community, individualised PBSP’s and provider/ family support | Small sample size, interventions not individually assessed |
| Higgins L | 20 adults with ID | Case Report | Periodic Service Review, Incident Reporting and Investigation System, Behaviour Support Plan Quality Evaluation tool, Maslow Assessment of Needs Scale, Positive Environment Checklist, MTS, staff turnover and retention data, qualitative feedback | Practice leadership by PBS implementation team, individual PBSP’s, enrichment of the physical and social environment, interactive meaningful engagement training, weekly “bite- size” staff training in PBS concepts and principles | Consistent improvements for target interventions in key service improvement areas observed. 20 PBSP developed of superior quality. Use of restrictive practices reduced by 99% and reduction in incidents of problem behaviour. Increases in staff retention and reductions in staff turnover indicated | Study lacks experimental control, independent observation, inter- rater reliability and treatment fidelity data. Intervention was resource intensive with heavy reliance on one practice leader in particular |
| McGill P, Vanono L, Clover W, Smyth E, Cooper V, Hopkins L, Barratt N, Joyce C, Henderson K, Sekasi S, Davis S & Deveau R | 81 adults with ID | Pragmatic cluster randomised controlled trial | Aberrant Behaviour Checklist, Engagement in Meaningful Activity Checklist – Revised, Active Support Measure, edited Individual Schedule, Short Adaptive Behaviour Scale, Social Validity Survey, Periodic Service Review | Audit of practice quality across settings to determine outcome standards across 8 domains of social care practice, agreement of standards with staff teams, monthly progress review meetings, performance feedback to managers, specific coaching support and training for DSP/ Managers, utilisation of existing and external local professional resources, progress chasing and fading of support towards the conclusion of the intervention | An average of 80% of outcome standards set were achieved. Challenging behaviour reduced significantly in all the experimental group settings. Significant increase in quality of social care was observed. While quality of life improved more in experimental settings there wasn’t a significant difference between groups on this measure. The intervention was recieved positively by staff, families and professionals engaged with experimental settings. | Results may be confounded by additional attention received in experimental settings, no data on supports for control group during intervention, impact of staff turnover, cost of intervention not measured, risk of bias due to experimenter involvement in intervention and analysis, some measures of unknown reliability/ validity |
| McKenzie K, Martin R, Metcalfe D, Murray G, McNall A & Noone S | 42 Staff | Qualitative – thematic analysis | Semi-structured interviews | Training programme including face to face teaching, e-learning and supervision targeting system-wide as well as individual change with two qualification levels: a) Postgraduate certificate or advanced diploma in leading PBS (level 6/7 award); b) Certificate in facilitating PBS in teams or Award of competence in PBS for support workers (level 4 awards) Community of practice to support development of staff and shared understanding of core PBS principles | Two themes and six subthemes were identified by the researchers. Participants highlighted the importance of understanding the principles and values of PBS to the successful adoption of the model. Participants expressed a confidence in the approach due to its evidence base. The systemic multi- component nature of PBS were also determined to be crucial, and participants highlighted successes at both multiple organisational levels and for people with ID and their families. | Study reflected staff opinions and not the adults with ID who have experienced the intervention, participants were a self-selecting group and their opinions may differ from other staff who declined to participate, staff interviewed by different researchers, no fidelity checks for subjective experiences, risk of bias as researchers were knowledgeable of the model |
| Reid D, Rotholz D, Parsons M, Morris L, Braswell B, Green C & Schell R | 398 Staff | Repeated measures within and between groups | Observational checklists, training evaluation forms, focus group feedback | Competency based PBS supervisory training programme with 26 modules combining classroom based and on the job training approaches. Each module targeted a specific knowledge base and/or performance skill | In the initial phase, all participants achieved 100% mastery in both observation and staff training skills. In the state- wide implementation phase, 85% of participants successfully completed the training. Feedback indicated that 95% of participants reported the training to be extremely/ very useful and 99.6% would recommend to colleagues. Feedback on impact of training on practice indicated improved quality of care for supported individuals and enhanced supervision with DSP. | No formal evaluation of the outcomes experienced by individuals with ID were included |
| Riding T | Not stated | Case report | Central incident register, programme of audits for PBSP, family and carer involvement and post-incident debrief | “Safewards” an integrated model of conflict and containment PBS training resources, PBS e-learning module for entire staff team | All forms of restraint use reduced by 42% from baseline. Planned use of prone restraint eliminated. , Quality of PSBP’s described as “exceptional” and positive culture change acknowledged by external quality assessors. | No experimental control demonstrated or reliability/validity checks. Also no data on implementation fidelity. |
Table 1: Details of Included Studies.
Participants
Participants were characterized as either individuals with ID or staff working with individuals with ID. Three studies described their participant group as staff members [42, 44, 45] and three studies identified individuals with ID as their target population [43, 47, 48]. One study identified both staff and adults with ID as the population group [46], and two did not specify whether the participants were staff or individuals with ID [41, 49]. For some of the studies the primary population was described as adults with ID, however staff related data were also included in the results [42, 43, 47]. Based on the reported demographic information, 293 adults with ID and 565 staff participated in systemic PBS interventions across all nine included studies. All individuals supported who participated in the studies were adults with ID and/or autism and presented with behaviours of concern. Staff participants included DSP, managers and supervisors, and clinical personnel. The age range for adults with ID was reported as 18 to 82, and the age range for DSP and supervisors was reported as 18 to 70.
Outcome Measures for Adults with ID
Dependent variables and selected outcome measures for participants with ID across the included studies are summarised in Table 2. While six of the studies reported data on problem behaviour [41,43,46-49l, only two studies employed an identified quality of life measure [47, 48].
| Dependent Variable | Measures | Studies |
|---|---|---|
| Behaviours of concern | Routine incident reports | Evans, et al. [46]; Higgins [47]; Riding [49] |
| Behaviour Monitoring Forms | Allen, et al. [41] | |
| Behaviour Problems Inventory (BPI) Rojahn, et al. [58] | Fuchs, et al. [48] | |
| Aberrant Behaviour Checklist (ABC) Aman , et al. [59] | McGill, et al. [43] | |
| Physical, Social and Emotional Wellbeing | HoNOS-LD | Fuchs, et al. [48] |
| Adaptive Behaviour | Short Adaptive Behaviour Scale (SABS) | McGill, et al. [43] |
| Quality of support | Engagement in Meaningful Activity Checklist (EMAC-R) (Mansell J, et al. [60] | McGill, et al. [43] |
| Active Support Measure (ASM) (Mansell J, et al. [61] | ||
| Quality of life | Guernsey Community and Participation Leisure Assessment (GCLPA) Baker [62] | Fuchs, et al. [48] |
| The Maslow Assessment of Needs Scale (Mans-LD) Skirrow, et al. [63] | Higgins [47] |
Table 2: Dependent Variables and Outcome Measures for Participants with ID.
Outcome Measures for Staff and/or Setting
A summary of the dependent variables and outcome measures used for staff participants is shown in Table 3. Several of the articles used existing organisational data collection methods [45, 46, 47] for staff related data, and cited operational efficiency as the rationale for this decision. However, as these tools are of unknown reliability and validity, the results of these reports need to be interpreted with care.
| Dependent Variables | Measures | Studies |
|---|---|---|
| Quality and fidelity | Observational checklists | Evans, et al. [46]; Reid, et al. [45] |
| PBSP fidelity check Horner, et al. [64] PCP fidelity checks | Freeman, et al. [42] McGill, et al. [43]; Higgins [47] | |
| Periodic Service Review LaVigna, et al [65] | Higgins [47] | |
| Behaviour Support Plan Quality Evaluation Tool Browning Wright, et al. [66] Positive Environment Checklist Albin, et al. [67] | Higgins [47] | |
| PBSP Audits | Riding [49] | |
| Social Validity | Social validity survey | Evans, et al. [46]; McGill, et al. [43] |
| Consumer satisfaction | The Person-Centred Planning Process Satisfaction Survey Abery, et al. [68] | Freeman, et al. [42] |
| Contextual fit | The Self-Assessment of Contextual Fit Survey R. Horner, et al. [69] | Freeman, et al. [42] |
| Staff perspectives and feedback | Semi-structured interviews | McKenzie, et al. [44]; Higgins [47] |
| Training evaluation forms | Reid, et al. [45] | |
| Focus groups | Reid, et al. [45] | |
| Post incident debriefs | Riding [49] | |
| Staff turnover and retention | Routine organisational data | Higgins [47] |
Table 3: Dependent Variables and Outcome Measures for Staff Participants.
Design
Six of the included articles were categorized as case reports of an intervention and did not provide empirical analyses [41, 42, 46, 47, 49]. Within the cohort of empirical studies, only one used a control group in a pragmatic cluster randomized control trial [43], one study adopted a repeated measures within and between subjects design [45] and one selected a naturalistic pre-post intervention evaluation [48]. One of the studies was a qualitative design using thematic analysis McKenzie, et al. [44] and one study included qualitative feedback in their reported findings [48].
Setting and Study Location
Six of the studies were conducted in the UK [41, 43, 44, 47, 48, 49] and three in the United States [42, 45, 46]. With respect to the settings, four of the articles involve specialist clinical in-patient settings for adults with ID and/or autism and challenging behaviours [41, 46, 47, 49], three include community based residential settings [43, 45, 46] and three involved disability service providers where it is not specified if they are day services, residential or both [42, 44, 48]. Three studies involved one service setting [41, 47, 49], four of the studies concerned multiple settings [43, 44, 46, 48] and two of the included articles reported on state-wide implementation of the model [42, 49]. Study authors were affiliated with the host organisations in five of the included studies Allen, et al. [41, 42, 45, 46, 48, 49], and were affiliated with the academic institution part funding the research.
Development of Interventions
Four of the included studies reported conducting various audits of service provision, environment, and staff performance with the aim of identifying key areas of practice development within the systemic PBS construct [43, 44, 47, 49]. The remaining studies based these elements on evidence-based practice in the literature, government guidance reports and expertise within the discipline [41, 42, 45, 46, 48, 49]. Two of the studies incorporated the views of the individuals with ID and their families into the development of the intervention [44, 48].
Treatment Components
The training components identified in the included articles are summarized in Table 4 based on the multi-tiered framework of systemic PBS. Data driven reviews occurred across a variety of areas, including job performance and supervision [41, 43, 45, 46, 47, 49] implementation fidelity checks [41, 42, 43, 46, 47] and quality of supports provided Freeman, et al. [42, 43, 45, 47, 49]. All included studies incorporated a form of workforce development program in their intervention framework. The structure and content of development programmes varied from specific brief workshops in PBS concepts and social care practice [41, 43, 47] to comprehensive longitudinal training in positive behaviour support and person centred planning [42, 44, 45]. Several of the training programmes involved work-based activities to encourage participants to bring knowledge and skills developed into day-to-day practice [42, 43, 44, 4647]. Three studies integrated e-learning into the administration of the staff training programme [42, 44, 49]. Three of the articles specifically detail environmental enhancement strategies [41, 47, 48] including development of both physical and social environments for the individuals supported.
| Tier 1 Supports | Tier 3 Supports |
|---|---|
| Data driven reviews and feedback Allen, et al. [41]; Evans, et al. [46]; Fuchs, et al. [48]; Higgins [47]; McGill, et al. [43]; Riding [49] | Individualised PBSP Allen, et al. [41,42,47,48] |
| Workforce development Allen, et al. [41-49] | Multi-disciplinary Reviews Allen, et al. [41,43,48] |
| Quality of Life enhancement through person centred planning, active supports and/or meaningful engagement [41,42,43,46,47,448] | Family involvement [48,49] |
| Safe reactive approaches [41,48,49] | |
| Environmental enhancement [41,47,48] |
Table 4: Summary of SWPBS Treatment Components.
Outcomes
Two articles reported improvements in quality of life for the individuals supported Fuchs, et al. [43, 48], however the improvements in the latter were not statistically significant. Four of the studies reported reductions in distressed behaviours [43, 46, 47, 48], and three studies reported decreases in use of restrictive practices such as physical restraint [41, 47, 49]. Improvement in quality of supports were reported in respect to the quality of PBSP’s and PCP’s [42, 47, 49]; community transitions and environments [48]; quality of staff interactions and engagement [43, 45] and staff mastery of PBS competencies [45]. Increases in implementation fidelity were reported in three of the studies Evans, et al. [43, 46, 47]. Several of the included articles reported on staff experiences and feedback. Staff reported feeling more confident in their practice [46], an appreciation for the principles and values of systemic PBS [44], and highlighted clinical leadership, multi-disciplinary team (MDT) coordination, systemic implementation and a person/family centered approach as crucial factors for successful outcomes [44, 48]. However, staff also expressed that the intervention was resource intensive with respect to time [46]. Two studies reported improvements in staff retention [44, 47] and one study reported significant cost savings following implementation of the model [48].
Quality Assessment of Included Studies
Individual, overall quality scores and summary percentages are detailed in Table 5. Results of the quality appraisal of included studies using the QATSDD [57] indicates that the articles were of moderate eminence (52%) ranging from a low score of 23% [41] to a high score of 73% [43].
| Study | QATSDD Total Score | Percentage Score |
|---|---|---|
| Allen, et al. [41] | Nov-48 | 23% |
| Evans, et al. [46] | 24/48 | 50% |
| Freeman, et al. [42] | 25/48 | 52% |
| Fuchs, et al. [48] | 26/48 | 54% |
| Higgins [47] | 27/48 | 56% |
| McGill, et al. [43] | 35/48 | 73% |
| McKenzie, et al. [44] | 33/48 | 69% |
| Reid, et al. [45] | 30/48 | 63% |
| Riding [49] | 15/48 | 31% |
| Total Score for included studies | 52% |
Table 5: Critical Appraisal Summary Scores of Included Studies Using the QATSDD [57].
Discussion
There is a growing body of literature from 2000 evidencing the efficacy of systemic applications of PBS in promoting quality of life outcomes and reducing problem behaviours. However, few studies to date have focused on the inclusion of adult populations. The aim of this synthesis was to identify the extant published research on the systemic application of PBS and to examine how findings from this research base may impact on future practice. The current synthesis highlighted that the implementation of this model with an adult population may currently be considered incipient. The current review evaluated 9 studies examining the impact of SWPBS with participants over the age of 18 years. The quality of these studies was assessed using the QATSDD [57] and were coded and analyzed using an adapted version [55] of the standard data extraction template on the Covidence platform [54]. Included articles employed diverse designs, with the majority utilising case reports, followed by group designs and qualitative methodologies, or a combination of these. All the reported interventions included multiple components that fit with the defined values and principles of SWPBS, with the majority including some form of workforce development programme in their intervention. All articles reported successful outcomes across a range of areas including improved quality of life, levels of engagement from DSP, skills in DSP and supervisors, reduction in restrictive practices and social validity or treatment acceptability of intervention componants. However, few of the articles employed robust statistical analyses to examine the significance of these results, and as many of the included studies did not implement experimental designs, reliability and validity of the studies is inconclusive at best. Quality assessment of the included articles implied limitations in the congruence, clarity, and Organisation of the reports. The identified articles will be discussed in terms of a. Limitations to the research, b. Study settings, c. Rationale for selecting the model, d. Treatment components in respect to the defining characteristics of SWPBS, e. Observed outcomes and f. Areas for future research.
Several limitations are described in the included studies. With respect to procedure, five studies involved case reports whereby no experimental control can be inferred [41, 42, 46, 47, 49]. Additionally, four of the studies did not include reliability or validity checks [41,46,47,49l, while McGill, et al. [43] noted that some of the measures employed were of unknown reliability and validity. Allen, et al. [41] commented that no data on collateral changes for participants, such as adjustments to medication, were collected and thus an influence of these effects on the observed outcomes cannot be ruled out. Similarly, McGill, et al. [43] did not collect data on any interventions received by the control groups over the duration of the study, and results need to be interpreted with caution. However, the studies that did employ experimental designs observed what may be considered encouraging outcomes [43, 45, 48], echoing the findings of the case reports without experimental controls. This exemplifies a core principle of PBS, flexibility in scientific practices, whereby PBS recognizes the need for flexibility to accommodate the study of practical efficacy and causal processes. Several authors cited difficulties with staff resources in relation to turnover and attrition [43, 48] and availability [46, 47] although only the latter study collected specific data in relation to this. These findings reflect the ongoing problem of maintaining consistent staff support in disability organisations [70, 71]. Notably, Higgins [47] observed increased staff retention following implementation of SWPBS, suggesting that implementation of the model can potentially assuage these concerns. Allen, et al. [41] had similar difficulties with variation in the adults with ID population. However, as this was due to several discharges from acute services, and with new residents subsequently being referred in, this may be interpreted as an indicator of the efficacy of the model in improving problem behaviours and wellbeing. Finally, five of the articles did not report on outcomes for the adults with ID involved in the intervention [42, 44, 45, 46] which juxtaposes the person-centered principles and value based on the SWPBS model.
All of the included studies were based in an adult disability services, with four involving clinical inpatient locations [41, 46, 47, 49], two in community based residential settings [43, 45] and three in disability organisations where it is not specified if they were day/residential services, or both. With the progression of the inclusion movement and a rights- based agenda in disability service provision, progressively more adults with intellectual disabilities are moving to community based residential settings. It is surprising that so few studies are available examining the implementation of this model in the community. This may be considered most pertinent to Ireland, where PBS is mandated under the Health Act 2007, however none of the studies were conducted with an Irish population.
While there was some variation in how treatment components were selected (e.g., based on literature or needs analysis in the setting), there are a lot of similarities in the selected treatment components across the nine studies (see Table 4). For example, all the studies included a workforce development plan, incorporating various forms of front- line staff training [43, 44, 46, 47, 48, 49] and/or management or supervisor training [41, 43, 45, 46]. Furthermore, this component was an important theme in the successful adoption of SWPBS in the qualitative study by McKenzie, et al. [44]. This systemic approach to skills development is not identified as a specific treatment component for people with ID in the included studies. The inclusion of active supports Allen, et al. [41, 43] and person-centred planning [42, 47, 72] is reflective of a lifespan perspective and focus on comprehensive lifestyle change and quality of life; two core doctrines of the PBS model. This might be considered as an important adaption to the school-wide model, as taking a strong scholastic perspective may not be appropriate for adult populations. Several of the authors included some form of regular team meeting to support data driven feedback and progress review [43, 46, 48], which are identified as core components of a SWPBS approach [33]. Finally, some of the studies incorporated the SWPBS model into organizational policies and practice documentation Allen, et al. [41, 46, 47] and qualitative feedback indicated that this was perceived by staff as an important element in intervention [44].
However, not all authors adopted this approach, which may limit maintenance of the intervention after the research period comes to an end. Future studies should consider the development of intervention manuals that can be incorporated into organizational guidance documentation to maintain implementation fidelity and treatment outcomes [43].
Important outcomes were observed across the included studies in terms of person-centered and rights- based practice in disability service provision. Notably, three of the studies reported considerable decrease in the use of physical restraint [41, 47, 49], with the deliberate and planned use of prone restraint being eliminated in the latter. In the wake of multiple controversies such as the Winterbourne [73] and Áras Attracta scandals [74] where widespread abusive practices were unearthed, it is crucial that support staff are skilled in evidenced proactive rights-based practices. None of the included articles completed component analyses to explore which of the treatment components were most effective in producing the observed outcomes. One author Riding [49] stated that “in practice, it matters little and was most likely a combination of all three” (p. 182). However, qualitative feedback indicated that:
- A core foundation in the principles and values of PBS
- Good leadership that cascades from experts to facilitators to wider DSP throughout Organisation,
- Realising outcomes through evaluation and feedback and
- Embedding SWPBS within the culture of the organisation through policies and practice documents were recognised by treatment agents as essential [44, 48]. Social validity surveys found high levels of acceptance and satisfaction with the model, but some staff recognised that it was resource intensive [41, 43, 46]. This supports the need for embedding SWPBS in organisational policy documentation so services can commission funding appropriately for future service planning and delivery.
Several of the authors highlight the need for future research to adopt more rigorous empirical approaches in examining implementation and impact of SWPBS with adult populations. Results of the quality appraisal using the QATSDD [57] in the present study further supports this contention. The randomised controlled trial (RCT) is arguably the most scientifically rigorous method of hypothesis testing currently available, and accordingly is considered the gold standard design for evaluating intervention efficacy [75]. While McGill, et al. [43] adopted this design, they and other authors highlight the need for future replication studies to provide greater validity and generalisability to the present findings. There are currently no professional third level training programmes in Ireland in PBS, and there are a very limited number of practitioners with expertise in PBS in the state [76]. The cascade model cited by McKenzie, et al. [44] has been shown to be promising in other studies [52], therefore further research into the manualising of the model for disability settings is needed. This could allow efficient use of the available PBS expertise to work with building SWPBS capacities across multiple settings. It is also important to consider further research into scaling up of the interventions so that SWPBS might be applied regionally or nationally, with a view to embedding the culture into disability practices and building capacity across the state [42, 48]. Finally, further research needs to incorporate measure of individuals with ID and staff outcomes, particularly in relation to workforce development programmes, to ensure a more comprehensive evaluation of the impact of the model [77].
• Compliance with Ethical Standards Not applicable as this is a literature review and not original research involving human participants and/or animals.
• Acknowledgements The authors with to acknowledge the supported adults and staff of St. Patricks Centre (Kilkenny) ltd. for their participation in this study.
• Statements and Declarations We confirm that this work is original and has not been published elsewhere, nor is it currently under consideration for publication elsewhere. Deirdre Kearney is a former employee of St. Patricks Centre (Kilkenny) Ltd. This research was funded by the Irish Research Council Employment Based Postgraduate Programme (project ID R15310) in partnership with St. Patricks Centre (Kilkenny) ltd. and Trinity College Dublin. ORCID: https://orcid.org/0000-0001-5445-5607
References
-
Dunlap G, Carr E (2007) Positive Behavior Support and Developmental Disabilities: A Summary and Analysis of Research. In: Odom SL, Horner RH, et al. (Eds.), Handbook of Developmental Disabilities pp: 469-482.
-
Dunlap G, Sailor W, Horner RH, Sugai G (2009) Overview and History of Positive Behavior Support. Handbook of Positive Behavior Support pp: 3-16.
-
Horner RD, Barton ES (1980) Operant Techniques in the Analysis and Modification of Self-Injurious Behavior: A Review. Behavior Research of Severe Developmental Disabilities 1(1): 61-91.
-
Repp AC, Deitz SM (1974) Reducing Aggressive And Self‐Injurious Behavior Of Institutionalized Retarded Children Through Reinforcement of other Behaviors. Journal of Applied Behavior Analysis 7(2): 313-325.
-
Snell ME (1978) Systematic Instruction of the Moderately and Severely Handicapped. In: Snell ME (Ed.), 2nd (Edn.), C.E. Merrill Publishing Company, USA, pp: 543.
-
Renzaglia A, Bates P (1983) Socially appropriate behavior. In Systematic instruction of the moderately and severely handicapped. In: Renzaglia A, Bates P (Eds.), 2nd (Edn), Columbus, Merrill, OH, USA, pp: 314-356.
-
Beadle-Brown J, Mansell J, Kozma A (2007) Deinstitutionalization in intellectual disabilities. Current Opinion in Psychiatry 20(5): 437-442.
-
Hext G, Clark LL, Xyrichis A (2018) Reducing Restrictive Practice in Adult Services: Not Only an Issue for Mental Health Professionals. British Journal of Nursing 27(9): 479-485.
-
Lemay RA (2009) Deinstitutionalization of People with Developmental Disabilities: A Review of the Literature. Canadian Journal of Community Mental Health 28(1): 181-194.
-
Johnston J, Foxx RM, Jacobson JW, Green G, Mulick JA (2006) Positive Behavior Support and Applied Behavior Analysis. The Behavior Analyst 29(1): 51-74.
-
Carr EG (1977) The Motivation of Self-Injurious Behavior: A Review of some Hypotheses. Psychological Bulletin 84(4): 800-816.
-
Donnellan AM, Mirenda PL, Mesaros RA, Fassbender LL (1984) Analyzing the Communicative Functions of Aberrant Behavior. Journal of the Association for Persons with Severe Handicaps 9(3): 201-212.
-
Iwata BA, Dorsey MF, Slifer KJ, Bauman KE, Richman GS (1994) Toward A Functional Analysis of Self‐Injury. Journal of Applied Behavior Analysis 27(2): 197-209.
-
Iwata BA, Dorsey MF, Slifer KJ, Bauman KE, Richman GS (1982) Toward A Functional Analysis of Self-Injury. Analysis and Intervention in Developmental Disabilities 2(1): 3-20.
-
Dunlap G, Kern Dunlap L, Clarke S, Robbins FR (1991) Functional Assessment, Curricular Revision, and Severe Behavior Problems. Journal of Applied Behavior Analysis 24(2): 387-397.
-
Horner RH, Dunlap G, Koegel RL, Carr EG, Sailor W, et al. (1990) Toward A Technology of “Nonaversive” Behavioral Support. Journal of the Association for Persons with Severe Handicaps 15(3): 125-132.
-
Repp AC, Singh NN (1990) Perspectives on the use of Nonaversive and Aversive Interventions for Persons with Developmental Disabilities. In: Repp AC, Singh NN (Eds.), Sycamore Publishing Company.
-
Sugai G, Horner R (2002) The Evolution of Discipline Practices: School-Wide Positive Behavior Supports. Child & Family Behavior Therapy 24(1-2): 23-50.
-
Carr EG, Dunlap G, Horner RH, Koegel RL, Turnbull AP, et al. (2002) Positive Behavior Support: Evolution of an Applied Science. Journal of Positive Behavior Interventions 4(1): 4- 16.
-
Gao X (2020) Meta-Analysis of Family-Centered Positive Behaviour Support with Families of Children with Developmental Disabilities and Problem Behaviour. University of British Columbia, USA.
-
Hayward BA, Poed S, McKay‐Brown L, McVilly KR (2021) Introducing Positive Behaviour Support (PBS) into Disability Services for Successful Adoption: A Synthesised Systematic Review. British Journal of Learning Disabilities 49(2): 145-161.
-
Karger G, Davies B, Hare DJ (2018) The Perception of Positive Behavioural Support: A Systematic Review. International Journal of Positive Behavioural Support 8(2): 16-32.
-
MacDonald A, McGill P (2013) Outcomes of Staff Training in Positive Behaviour Support: A Systematic Review. Journal of Developmental and Physical Disabilities 25(1): 17-33.
-
Mahon D, Walsh E, Holloway J, Lydon H (2021) A Systematic Review of Training Methods to Increase Staff’s Knowledge and Implementation of Positive Behaviour Support in Residential and Day Settings for Individuals with Intellectual and Developmental Disabilities. Journal of Intellectual Disabilities 26(3): 732-757.
-
Marquis JG, Horner RH, Carr EG, Turnbull AP, Thompson M, et al. (2000) A Meta-Analysis of Positive Behavior Support. In: Contemporary Special Education Research pp: 149-190
-
Mowat JG (2012) Positive Behaviour Support in Secondary Schools: A Practical Guide. European Journal of Teacher Education 35(3): 378-381.
-
Solomon BG, Klein SA, Hintze JM, Cressey JM, Peller SL (2012) A Meta‐Analysis of School‐ wide Positive Behavior Support: An Exploratory Study Using Single‐ Case Synthesis. Psychology in the Schools 49(2): 105- 121.
-
Wardale S, Davis F, Dalton C (2014) Positive Behavioural Support Training in A Secure Forensic Setting: The Impact on Staff Knowledge and Positive Behavioural Support Plan Quality. International Journal of Positive Behavioural Support 4(2): 9-13.
-
Duchnowski AJ, Kutash K (2009) Integrating PBS, Mental Health Services, and Family-Driven Care. In: Handbook of Positive Behavior Support pp: 203-231.
-
Simonsen B, Sugai G (2019) School-Wide Positive Behavioral Interventions and Supports: A Systems- Level Application of Behavioral Principles. In: Little SG, Akin-Little A (Eds.), Behavioral interventions in schools: Evidence-based positive strategies. American Psychological Association pp: 35-60.
-
Turnbull A, Edmonson H, Griggs P, Wickham D, Sailor W, et al. (2002) A blueprint for school wide positive behavior support: Implementation of three components. Exceptional Children 68(3): 377-402.
-
Horner RH, Sugai G, Anderson CM (2010) Examining the Evidence Base for School-Wide Positive Behavior Support. Focus on Exceptional Children 42(8).
-
Sugai G, Horner RH (2009) Defining and Describing School wide Positive Behavior Support. In: Handbook of Positive Behavior Support, pp: 307-326.
-
Lee A, Gage NA (2020) Updating and Expanding Systematic Reviews and Meta‐Analyses on the Effects of School‐Wide Positive Behavior Interventions and Supports. Psychology in the Schools 57(5): 783-804.
-
Noltemeyer A, Palmer K, James AG, Wiechman S (2019) School-Wide Positive Behavioral Interventions and Supports (SWPBIS): A Synthesis of Existing Research. International Journal of School & Educational Psychology 7(4): 253-262.
-
Rotholz DA, Ford ME (2003) Statewide System Change in Positive Behavior Support. Mental Retardation 41(5): 354-364.
-
Simonsen B, Jeffrey Pearsall J, Sugai G, McCurdy B (2011) Alternative Setting-Wide Positive Behavior Support. Behavioral Disorders 36(4): 213-224.
-
Dixon-Woods M, Bonas S, Booth A, Jones DR, Miller T, et al. (2006) How can Systematic Reviews Incorporate Qualitative Research A Critical Perspective. Qualitative research 6(1): 27-44.
-
Harrison R, Jones B, Gardener P, Lawton R (2021) Quality Assessment with Diverse Studies (Quads): An Appraisal tool for Methodological and Reporting Quality in Systematic Reviews of Mixed-or Multi- Method Studies. BMC Health Services Research 21(1): 144.
-
Collins KM, Onwuegbuzie AJ, Sutton IL (2006) A Model Incorporating the Rationale And Purpose for Conducting Mixed-Methods Research in Special Education and Beyond. Learning Disabilities: A Contemporary Journal 4(1): 67-100.
-
Allen D, Kaye N, Horwood S, Gray D, Mines S (2012) The Impact of A Whole-Organisation Approach to Positive Behavioural Support on the Use of Physical Interventions. International Journal of Positive Behavioural Support 2(1): 26-30.
-
Freeman R, Smith C, Zarcone J, Kimbrough P, et al. (2005) Building a Statewide Plan for Embedding Positive Behavior Support in Human Service Organizations. Journal of Positive Behavior Interventions 7(2): 109- 119.
-
McGill P, Vanono L, Clover W, Smyth E, Cooper V, et al. (2018) Reducing Challenging Behaviour of Adults with Intellectual Disabilities in Supported Accommodation: A Cluster Randomized Controlled Trial of Setting-Wide Positive Behaviour Support. Research in Developmental Disabilities 81: 143-154.
-
McKenzie K, Martin R, Metcalfe D, Murray G, McNall A, et al. (2020) Look, All our Hard Work Is Paying Off”: A Qualitative Evaluation of A System‐Wide, Workforce Development Model to Promote Positive Behavioural Support. Journal of Applied Research in Intellectual Disabilities 33(6): 1512- 1522.
-
Reid DH, Rotholz DA, Parsons MB, Morris L, Braswell BA, et al. (2003) Training Human Service Supervisors in Aspects of PBS: Evaluation of A Statewide, Performance- Based Program. Journal of Positive Behavior Interventions 5(1): 35-46.
-
Evans R, Evans L, Rodgers T (2020) How to Sustain PBS Without Magic in Forensic Psychiatric Facilities & Community Sellings. Journal of Organizational Psychology 20(3): 18-29.
-
Higgins L (2021) Secure Unit: Positive Behavioural Support and Restraint Reduction in A Unit for Offenders with an Intellectual Disability and/or Autism: Practice Paper. International Journal of Positive Behavioural Support 11(1): 42-54.
-
Fuchs K, Ravoux P (2019) Transforming Care: Developing A Community Enhanced Intervention Service. Advances in Mental Health and Intellectual Disabilities.
-
Riding T (2016) Exorcising Restraint: Reducing the Use of Restrictive Interventions in a Secure Learning Disability Service. Journal of Intellectual Disabilities and Offending Behaviour 7(4).
-
Davies B, Mallows L, Hoare T (2016) “Supporting me through Emotional Times, All Different Kinds of Behaviour.” Forensic Mental Health Service Users Understanding of Positive Behavioural Support. The Journal of Forensic Psychiatry & Psychology 27(4): 530- 550.
-
Karger G, Davies B, Jenkins R, Samuel V (2018) Staff Perceptions of Positive Behavioural Support in A Secure Forensic Adult Mental Health Setting. Journal of Forensic Practice 20(1).
-
MacDonald A, McGill P, Murphy G (2018) An Evaluation of Staff Training in Positive Behavioural Support. Journal of Applied Research in Intellectual Disabilities 31(6): 1046-1061.
-
Denne L, Jones E, Lowe K, Brown FJ, Hughes JC (2015) Putting Positive Behavioural Support into Practice: The Challenges of Workforce Training and Development. International Journal of Positive Behavioural Support 5(2): 43-54.
-
(2021) Covidence Systemic Review Software. Innovation VH.
-
Cooper H (2015) Research Synthesis and Meta-Analysis: A Step-by-Step Approach. In: Cooper H (Ed.), 5th (Edn.), Sage Publications 2: 384.
-
Fenton L, Lauckner H, Gilbert R (2015) The QATSDD Critical Appraisal Tool: Comments and Critiques. Journal of Evaluation in Clinical Practice 21(6): 1125-1128.
-
Sirriyeh R, Lawton R, Gardner P, Armitage G (2012) Reviewing Studies with Diverse Designs: the Development and Evaluation of a new tool. Journal of Evaluation in Clinical Practice 18(4): 746-752.
-
Rojahn J, Matson JL, Lott D, Esbensen AJ, Smalls Y(2001) The Behavior Problems Inventory: An Instrument For the Assessment Of Self-Injury, Stereotyped Behavior, and Aggression/Destruction in Individuals with Developmental Disabilities. J Autism Dev Disord 31(6): 577-588.
-
Aman MG, Singh NN (1986) Aberrant behavior checklist. Slosson, East Aurora, NY, USA.
-
Mansell J, Elliott T, Beadle-Brown J, Ashman B, Macdonald S (2002) Engagement in meaningful activity and “active support” of people with intellectual disabilities in residential care. Research in Developmental Disabilities 23(5): 342-352.
-
Mansell J, Elliott T (1996) Active Support Measure. Canterbury, Tizard Centre.
-
Baker PA (2000) Measurement of community participation and use of leisure by service users with intellectual disabilities: The Guernsey Community Participation and Leisure Assessment (GCPLA). Journal of Applied Research in Intellectual Disabilities 13(3): 169-185.
-
Skirrow P, Perry E (2009) The Maslow Assessment of Needs Scales. Liverpool: Mersey Care NHS Trist.
-
Horner RH, Sugai G, Todd AW, Lewis-Palmer T (2000) Elements of Behavior Support Plans: A Technical Brief. Exceptionality 8(3): 205-215.
-
LaVigna G, Willis T, Shaull J, Abedi M, Sweitzer M (1994) The Periodic Service Review. Baltimore: Paul H Brookes.
-
Browning Wright D, Mayer GR, Saren D (2006) The Behaviour Intervention Plan Quality Evaluation Scoring Guide II.
-
Albin R, O’Neil R (1994) Proactive Behaviour Support: Structuring and Assessing Environments. Specialised Training Project. University of Oregon.
-
Abery B, McBride M, Rotholz D (1999) The Person- Centered Planning Process Satisfaction Survey (PCP- SS). Minneapolis: University of Minnesota, Institute on Community Integration.
-
Horner R, Albin R, Borgmeier C, Salantine S (2003) Moving from Functional Assessment to the Design of Behavior Support. Paper presented at the Symposium presented at the Association for Behavior Analysis Annual Convention, San Franisco, CA, USA.
-
Hatton C, Emerson E, Rivers M, Mason H, Swarbrick R, et al. (2001) Factors associated with intended staff turnover and job search behaviour in services for people with intellectual disability. Journal of Intellectual Disability Research 45(3): 258-270.
-
McCarron M, Lombard-Vance R, Murphy E, May P, Webb N, et al. (2019) Effect Of Deinstitutionalisation on Quality of Life for Adults with Intellectual Disabilities: A Systematic Review. BMJ open 9(4): e025735.
-
Allen D, McGill P, Hastings RP, Toogood S, Baker P, et al. (2013) Implementing Positive Behavioural Support: Changing Social and Organisational Contexts. International Journal of Positive Behavioural Support 3(2): 32-41.
-
Flynn M (2012) Winterbourne View Hospital. A Serious Case Review. Gloucestershire, UK: South Gloucestershire Council.
-
McCoy K, Carroll D, Judge A, McCormack B (2016) What Matters Most: Report of the Áras Attracta Swinford Review Group. Ireland: Áras Attracta Swinford Review Group.
-
Akobeng AK (2005) Understanding Randomised Controlled Trials. Archives of Disease in Childhood 90(8): 840-844.
-
Martin G (2015) 20 Years of Positive Behaviour Support- Implementing PBS in a Large Scale Service Setting, and the Role of the Clinical Nurse Specialist.
-
McKenzie K, McNall A, Noone S, Branch A, Murray G, et al. (2021) The Use of an Implementation Science Theoretical Framework to Inform the Development of A Region Wide Positive Behavioural Support Workforce Development approach. Journal of Applied Research in Intellectual Disabilities 34(3): 675-683.
- Systematic Review and Meta-analysis Investigating the Prevalence of Depression, Anxiety, Loneliness and Help seeking among International Students
- Family Experiences and their Interpretations as a Source of Adaptive Behaviour in Young Adults: A Qualitative Model of Adaptive Behaviour
- The Development of Responsibility in Teenage Mothers: A Qualitative Model
- Post-Truth Reality: Worldwide Infodemia and Mental Health Concerns during and Post COVID-19 Pandemic Scenarios
- Psycho-Emotional Rehabilitating Means of Overcoming Extreme and Stressful Impact
- The Paradox of Humbleness, Arrogance and the Concept of Fluid Individuality