The Evolution of the Comprehensive Health Span Evaluation for Special Operations Forces
If necessity is the mother of all inventions, then the battlefield has always been a stern teacher of medicine. Today’s operators and first responders carry a tourniquet in their kit because they have learned that controlling blood supply is a lifesaving technique.
Commentary
If necessity is the mother of all inventions, then the battlefield has always been a stern teacher of medicine. Today’s operators and first responders carry a tourniquet in their kit because they have learned that controlling blood supply is a lifesaving technique. However, back in 1537, it took a determined French surgeon named Ambroise Pare at the Siege of Turin to institute the practice of using tourniquets to frantically save the lives of his soldiers who were bleeding to death [1]. Similarly, it took the ingenuity of LT Carter Harmen to use his Sikorsky YR-4B to pull off the first helicopter-assisted medical evacuation when his comrades were pinned down in the jungles of Burma during WWII [2]. His innovation was quickly refined for future conflicts where the tragic lessons learned of ineffective communication in chaotic conditions produced today’s 9-line to streamline the medical evacuation system [3]. Innovation has always followed necessity in war. Psychological health has had a similar wartime to mainstream trajectory. The primary architect of U.S. WWI military psychiatry, Dr. Thomas Salmon, received a crash course in hard lessons learned from our British psychiatry allies after he realized how unprepared the U.S. was for managing combat stress. He quickly drafted the principles Commentary of frontline psychiatry, which like the lessons of physical medicine, emphasized immediate treatment to promote quicker recovery and mitigate long-term psychiatric disability [4]. During the Korean War the U.S. added mobile mental health teams to augment the multi-tiered battlefield psychiatry model of WWI, further decreasing time to intervention while extending care through consultation with non-mental health medical providers [5]. This same general model of embedded care, close to the fight, was relied upon and refined throughout both Iraq and Afghanistan. After WWI, Dr. Salmon leveraged insights gained from the European theatre to speak out against using the traditional mental health hospitals of the time to treat veterans. He understood that stigma keeps service members from seeking treatment, that camaraderie is a therapeutic force multiplier for veterans, and that outpatient, community- based treatment can be a strategic solution to reducing access to care [6]. Unfortunately, it took another World War to break away from treating veterans in psychiatric asylums and to apply Dr. Salmon’s ideas. Led by General Omar Bradley in 1945, the birth of the Veterans Administration (VA) saw 4,000 physicians hired to fill an aggressive hospital building campaign, designed to ensure the delivery of culturally competent healthcare [7]. Here, a veteran could get seen by his Primary Care Provider (PCP) and be referred to a specialist within the same organization. The concept was solid in theory, but as time proved, this hub-and-spoke methodology was vulnerable to communication breakdowns and siloed care due to the protracted periods of time between specialists. This specialist referral-based model of care persisted in both the military and VA until halfway through the War on Terror when, on June 24, 2010, the National
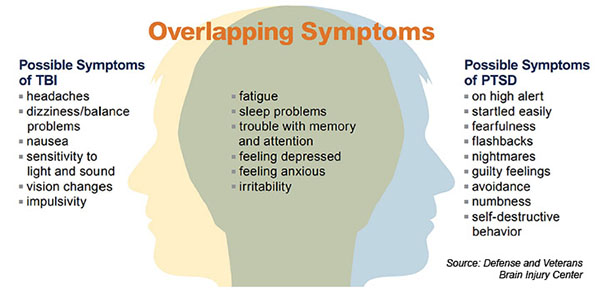
Intrepid Center of Excellence (NICoE) opened its doors as a directorate of Walter Reed National Military Medical Center and introduced a new interdisciplinary model of care [8]. Now, active-duty personnel were seen iteratively by a multidisciplinary staff over a designated amount of time that replaced specialist silos with cross-functional teams for a more efficient, comprehensive evaluation. Like the dire conditions in Burma that led LT Harmon to attempt something that hadn’t been done before, the creation of NICoE in 2010 by military medicine was a necessity. The War on Terror not only reintroduced Americans to combat- related PTSD (Post Traumatic Stress Disorder) en masse but overlaid it with Traumatic Brain Injuries (TBI) at an astonishing rate commensurate with the proliferation of improvised explosives. By 2008, data showed that one in five military personnel was diagnosed with PTSD [9], with rates of TBI varying between 9% and 28% [10]. “When PTSD and TBI coexist, it’s often difficult to sort out what’s going on. Changes in cognition such as memory and concentration, depression, anxiety, insomnia, and fatigue are common with both diagnoses. One basically feeds and reinforces the other, so it’s a complicated mix” (Figure 1) [11].
In 2024, we stand at a pivotal moment within operator brain health evaluation reminiscent of the transformative shifts experienced in 2010 when the integrated, multidisciplinary TBI evaluation was introduced to military medicine by NICoE. As we continue to distance ourselves from the relentless operational tempo of the Global War on Terror, a new clinical care landscape emerges, one that confronts the military and medical communities with a heightened awareness and a wealth of hard-earned insights from two decades of sustained conflict. The challenge now lies in integrating these lessons into our established evaluative procedures. To do so will require a candid reassessment of our current approach to evaluating operator brain health.
A central question to be asked is, should TBI remain the entry point for such an in-demand integrated, multidisciplinary evaluation for today’s operator? As it stands today, if an operator does not meet an organization’s TBI threshold, then he is generally left to the traditional PCP hub and spoke medical model of care that is often incompatible with their operational tempo. One potential consequence of this referral-based model of care is that operators only receive limited symptomatic relief for such neurological complaints as tinnitus, sleep apnea, and headaches [12], or comorbid behavioral health conditions such as anxiety and substance abuse [13]. Another consequence is delayed care or no care for this group of mission focused individuals who are already prone to minimization of symptoms. This is an especially noteworthy point when you consider that Belding, et al. [14] concluded that blast exposure elevated risks for more than 20 different diagnoses and that repeated exposure was associated with worse outcomes. An open dialogue on the state of operator brain health evaluation acknowledges that operators are inherently at high risk for acute and chronic blast and impact injury, that the heterogeneity of the mechanism of injury makes measuring it difficult (as does being recorded in one’s medical record), and that there is a subtle but not so obvious complex interplay between conditions that can be under-evaluated without an integrated, multidisciplinary evaluation. Adhering to a rigid TBI inclusion criterion potentially creates diagnostic blind spots especially when we account for the operator being at high risk for sub-concussive exposures (i.e. repetitive artillery or rockets, repetitive hull to wave impacts) that have known post-concussive sequela.
Unfortunately, relaxing inclusion criteria and broadening access to the type of comprehensive multidisciplinary evaluation being discussed is not practical within either the VA or military medicine. This integrated care model demands significant resources, limiting the number of patients that can be accommodated at any given time (typically 4-8 patients per cohort). This constraint exacerbates the already lengthy wait times for such care. Therefore, forging strategic partnerships with the nation’s leading academic medical centers is imperative for progress. With their diverse medical ecosystems, these centers are well-equipped to share the load and collaboratively address the escalating demand for evidence-based care and pioneering research. As the saying goes, a rising tide lifts all ships.
As science has evolved so has our understanding of the complex interrelated influences affecting our operators, making comprehensive integrated evidence-based assessment and treatment critical to their longevity. Since the PACT Act (Promise to Address Comprehensive Toxins) was commissioned in November 2022 there have been over 963,650 approved claims [15]. In response to the volume of substantiated claims, the VA Undersecretary for Health, Dr. S. Elnahal, stated: “This is really a confirmation of what advocates have been saying for years, that the denominator of veterans exposed to harmful substances is quite large” [16]. What is striking about the VA’s PACT Act performance dashboard is that of the over 5 million veterans who have completed a VA toxic exposure screening to date, less than 9% of these veterans have endorsed more than one toxic exposure. That is a stark contrast to special operations forces personnel who have not just a breadth of occupationally related environmental exposures (i.e. burn pits, lead, depleted uranium, asbestos, aviation fuel/fumes, etc.) but a depth of them through extensive training and multiple deployments. The biological consequences of these “complex mixtures” [17] was recognized by Special Operations Command in a March 5, 2024 written statement where routine cancer screenings were encouraged while advocating for “an in- depth study to characterize cancer risk and diagnosis within the active duty and retired Special Operations Forces (SOF) population” [18].
The paradigm shift occurring within SOF brain health evaluation has replaced TBI at the forefront of the diagnostic gateway with an exposure-based model. TBI isn’t simply a condition underdiagnosed within SOF [19]; it is one among many multifactorial ‘exposures,’ including environmental toxins and chronic stress that must be considered within a complex interrelated systems approach. Brain injuries can trigger underlying dysfunctions that extend well beyond the brain, affecting the endocrine system, sleep architecture, and other life-altering issues [19]. When we recognize that our operators have experienced multiple exposures beyond and related to TBI, it becomes clear that life-altering issues can extend to cancer, cardiovascular conditions, autoimmune disorders, and neurodegenerative diseases that threaten an operator’s long-term well-being. This underscores the crucial need for broader access to integrated, multidisciplinary evaluations to properly assess and educate our operators on their Health Span. Health Span is the years of life free from chronic disease. To avoid biological age outpacing the chronological age of our operators, as was shown to be the case with professional football players [20], we need an integrated evaluation that addresses the multitude of exposures that threaten their wellbeing and longevity. Forewarned is forearmed when it comes to the health of a population rich in exposures.
Contemporary SOF brain health evaluation presents a significant challenge that necessitates strategic military- civilian partnerships with the nation’s leading academic medical centers to meet the demand. An exemplary illustration of this approach is Home Base, a charitable organization anchored in a world class medical setting in Boston, Massachusetts, boasting a diverse ecosystem comprising Massachusetts General Brigham, Massachusetts Eye & Ear, Spaulding Rehabilitation Hospital, and the Harvard Medical system. In 2018, Home Base collaborated with Naval Special Warfare to swiftly develop a culturally competent 5-day integrated, multidisciplinary evaluation, which went online in less than six months and has since conducted over 500 comprehensive assessments of joint SOF operators. In response to concerns about environmental toxin exposure, Home Base partnered with the MGB Early Cancer Detection Clinic to integrate this capability into its existing 5-day SOF comprehensive Health Span evaluation within just seven months. Presently, Home Base continues to collaborate with world-renowned subject matter experts within its ecosystem to further enhance “exposure” evaluative capabilities to meet the evolving needs of contemporary operators. This serves as a compelling example of the possibilities that emerge when we thoughtfully consider what responsible load-sharing entails [21].
Contemporary SOF brain health evaluation presents a significant challenge that necessitates a paradigm shift away from TBI as the diagnostic gateway for an integrated, multidisciplinary evaluation, as well as Strategic military- civilian partnerships with the nation’s leading academic medical centers to meet the demand and preserve the Health Span of our operators.
References
-
Samuel L (2017) 6 medical innovations that moved from the battlefield to mainstream medicine. STAT: Reporting From the Frontiers of Health and Medicine.
-
National Museum of the United States Army (2024). MEDEVAC.
-
Bledsoe E (2023) What does nine line mean in military terms - explained.
-
Hans P, Stephanie O (2007) WAR & Military Mental Health. American Journal of Public Health 97(12): 2132- 2142.
-
Helmus TC, Glenn RW (2005) Steeling the Mind: Combat Stress Reactions and Their Implications for Urban Warfare. In: 1st (Edn.), RAND Corporation, pp: 174.
-
Cox C (2009) Invisible Wounds: The American Legion, Shell-Shocked Veterans, and American Society, 1919– 1924, in Traumatic Pasts: History, Psychiatry, and Trauma in the Modern Age, 1870–1930. In: Mark SM, et al. (Eds.), Cambridge University Press, New York.
-
Pickren WE, Schneider SF (2005) Psychology and the National Institute of Mental Health: A historical analysis of science, practice, and policy. American Psychological Association.
-
Health.mil (2023) About the NICoE.
-
RAND (2008) One in five Iraq and Afghanistan veterans suffer from PTSD or Major Depression.
-
Reger MA, Brenner LA, Pont AD (2025) Traumatic Brain Injury and Veteran Mortality after the War in Afghanistan. JAMA Netw Open 5(2): e2148158.
-
Lash M (2013) TBI and PTSD: Navigating the perfect storm. Brainline: All About Brain Injury and PTSD.
-
Martindale SL, Belding JN, Crawford CD, Rowland JA (2023) Validation of Military Occupational Specialty as a proxy for blast exposure using the Salisbury Blast Interview. Journal of Neurotrauma 40(21-22): 2321- 2329.
-
Belding JN, Englert RM, Bonkowski J, Thomsen CJ (2021) Occupational risk of low-level blast exposure and TBI-related medical diagnoses: A population- based epidemiological investigation (2005-2015). International Journal of Environmental Research and Public Health, 18(24): 12925.
-
Belding JN, Kolaja CA, Rull RP, Trone DW (2023) Single and repeated high-level blast, low-level blast, and new-onset self-reported health conditions in the U.S. Millennium Cohort Study: An exploratory investigation. Frontiers in Neurology 14: 1110717.
-
Department of Veterans Affairs (2024) PACT act performance dashboard, 21.
-
Shane IIIL (2023) Concern about military toxic exposure injuries remains high among vets. Air Force Times.
-
Jain P, Vineis P, Liquet B, Jelle V, Barbara B, et al. (2018) A multivariate approach to investigate the combined biological effects of multiple exposures. J Epidemiol Community Health 72(7): 564-571.
-
Skovlund J (2024) SOCOM calls for special ops veterans to report cancer screenings. Task & Purpose.
-
Hunter Seven Foundation (2024). Military Exposures.
-
Grashow R, Shaffer PTV, Dairi I, Lee H, Marengi D, et al. (2022) Healthspan and chronic disease burden among young adult and middle-aged male former American- style professional football players. British Journal of Sports Medicine 57(3): 166-171.
-
Haun JN, Nakase RR, Melillo C, Kean J, Benzinger RC, et al. (2023) Traumatic Brain Injury Intensive Evaluation and Treatment Program: Protocol for a Partnered Evaluation Initiative Mixed Methods Study. JMIR Res Protoc 12: e44776.
- Systematic Review and Meta-analysis Investigating the Prevalence of Depression, Anxiety, Loneliness and Help seeking among International Students
- Family Experiences and their Interpretations as a Source of Adaptive Behaviour in Young Adults: A Qualitative Model of Adaptive Behaviour
- The Development of Responsibility in Teenage Mothers: A Qualitative Model
- Post-Truth Reality: Worldwide Infodemia and Mental Health Concerns during and Post COVID-19 Pandemic Scenarios
- Psycho-Emotional Rehabilitating Means of Overcoming Extreme and Stressful Impact
- The Paradox of Humbleness, Arrogance and the Concept of Fluid Individuality