The Effectiveness of transcranial Direct Current Stimulation (tDCS) for Improving the Naming of a Patient with Apraxia: A Single Case Study
Aim: Studies have shown that transcranial Direct Current Stimulation (tDCS) can modulate cortical activity and performance of both healthy and brain-damaged people. In the present study, we investigated the effect of tDCS on the recovery of naming in one patient with apraxia of speech. Methods: After establishing a baseline in 3 weeks, the participant received regular speech therapy for 3 weeks alongside with tDCS. The participant received anodic stimulation over the left inferior frontal gyrus (Broca’s area) while he performed the repetition task. Results: The results showed that the participant improved in the naming task after language treatment combined with tDCS in the treatment phase in comparison to the baseline phase, and this difference was clinically significant (RCI=2.652). Discussion: This study showed that associating the language therapy with noninvasive brain stimulation (e.g. tDCS) can have a positive effect on rehabilitation outcomes in patients with acquired apraxia of speech.
Introduction
Apraxia of speech is an acquired speech motor disorder in which a patient cannot translate well-formed phonological frames into formerly learned kinematic information [1]. Focal brain damage like a stroke in the left hemisphere can cause a disorder in speech movements like apraxia of speech. The signs of the disorder are distortions of vowels and consonants that can be like sound substitutions in the absence of reduced strength or tone of muscles and articulators controlling phonation [2, 3].
Depending on the severity of the disorder, apraxia of speech may present with a variety of signs. In the less severe form, patients with apraxia can produce single syllables, words, or maybe short phrases. In most severe cases, a patient with apraxia may be unable to produce even a single word, syllable, or speech sound [4]. One common symptom is that patients with apraxia make groping oral movement to find a correct articulatory position and articulatory difficulties increase with the increase in word length. Patients with apraxia may also show a problem in the use of correct speech prosody [5]. Also, the speech rate is reduced, and speech errors increase when the complexity of utterances is more [2].
There is no agreement that which area in the brain is responsible for apraxia of speech, but a consensus is that brain injury in the left hemisphere (dominant for language), in the inferior frontal gyrus [6, 7] the left anterior insula [8] and/or in the subcortical structures, particularly in the basal ganglia [9, 10] may led to apraxia of speech.
Several treatment procedures have been proposed to treat the apraxia of speech, and no single approach has been proven to be more effective than others. Most of the studies focus on articulation disorders, and the first treatment protocol in this regard were proposed by Rosenbek, Hansen, et al. [11] which emphasize the relearning of articulation and sequencing of articulatory gestures to change the speech of patients from limited, automatic- reactive speech to more appropriate and purposeful speech. Recently, the researcher started to use technology to help the treatment process in apraxia of speech. One of these treatments is noninvasive brain stimulation (e.g. transcranial Direct Current Stimulation (tDCS)), but the efficacy of this treatment is not proven yet and further studies are needed [3].
As stated above, noninvasive brain stimulation (e.g. tDCS) are new techniques for remediating motor and language impairment. Transcranial direct current stimulation (tDCS) makes use of a weak polarizing direct current to deliver to the cortex through two electrodes placed on the scalp. In the previous studies by tDCS, the anode is usually placed to increase the cortical excitability over the region of interest and the cathode is placed to decrease the contralateral region [12]. The previous investigation showed that anodic stimulation may increase motor learning, visuo-motor performance, working memory, and verbal fluency in normal subjects. Recent studies of chronic neurological patients showed increased cortical excitability effects on the improvement of motor [13, 14], neurological and psychiatric symptoms [15, 16, 17].
Recently, new treatment techniques have highlighted the role of brain stimulation techniques, like transcranial direct current stimulation (tDCS), as complementary strategies to increase the efficiency of language treatment. Several studies have exhibited that that the word retrieval ability of aphasic patients showed greater improvement when the language therapy was combined with repeated tDCS stimulation [18, 19, 20, 21]. Until now few studies investigated the effect of tDCS on language recovery in patient with acquired apraxia of speech, and this preliminary studies showed positive effect of treatment with tDCS on promoting language abilities [22, 23, 24].
In this study, we aimed at investigating a patient with non-fluent aphasia, whether the application of anodic tDCS over the left inferior frontal gyrus (referred to as Broca’s area) alongside with language training for apraxia can promote his articulatory problems in naming test. As we mentioned before, based on the study by Hillis et al. [6], the left inferior frontal gyrus is impaired in apraxia of speech, and we chose this region because of its crucial role in speech articulation. Also, previous researches with apraxia have shown positive results when anodic tDCS were placed over Broca’s area [23, 24]
Methods
Subject
The participant was a 60 years old right-handed male who suffered left hemispheric stroke which occurred 5 years before the baseline assessment. He was a native Farsi speaker and had severe non-fluent aphasia with severe apraxia of speech. The collected data of this study conformed to the Code of Ethics of the World Medical Association (Declaration of Helsinki) printed in the British Medical Journal (18 July 1964).
Procedure
The Farsi naming test [25] was used to assess the naming of the patient. This test includes 50 images from 3 different familiar categories consists of 12 animals, 11 natural phenomena, and 27 man-made phenomena. Three baseline sessions were established for 3 weeks before treatment. In the treatment phase, the naming assessment was performed on the second session of the week and therefore, 6 assessments were performed during baseline and treatment.
Treatment
Treatment was performed twice per week for 3 weeks, and therefore, 6 treatment sessions were established. Each session includes the application of tDCS along with speech and language therapy for 20 minutes. The clinician and the subject seated face-to-face so that the patient could watch the articulatory movements of the clinician as a pattern. For the treatment of apraxia of speech, the clinician was orally presenting the whole stimuli and asking the patient to repeat it. Each stimulus was just presented one time to the patient. tDCS was applied using a portable device, with a pair of surface-soaked sponge electrodes (5 cm × 7 cm). An anodal electrode placed -the stimulating electrode- over the left inferior frontal gyrus (IFG, BA 44/45, a position defined according to the extended International 10-20 System). The cathode electrode was positioned over the contralateral supraorbital region [26]. During each session, anodic tDCS (current of 2 mA) was applied for 20 min.
Results
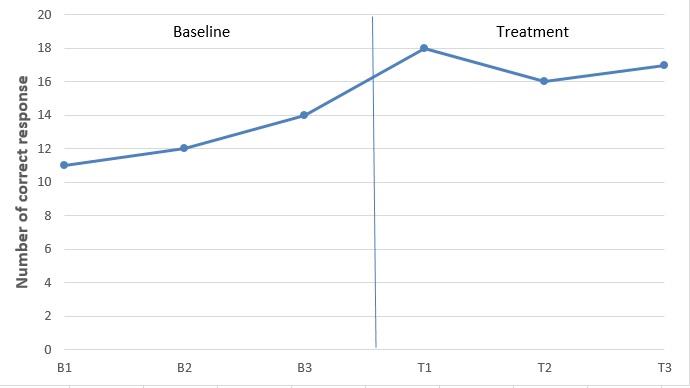
The number of correct responses to the naming assessment is shown in Figure 1. As shown in the graph, the number of correct responses are increased in baseline 2 (B2) and 3 (B3) comparing to baseline 1 (B1), but there is a visual improvement in the number of correct responses in the intervention phase in comparison to the baseline phase.
𝑅𝐶𝐼= Xpost −Xpre
Sdiff
In this study Xpre= 12.33, Xpost= 17 and Sdiff = 1.76 and the RCI =2.652. Jacobson and Truax (1992) stated that the change is considered reliable if the change index (RCI) is larger than 1.96. Therefore, we can assume that the naming ability of the patient in this is clinically improved after treatment.
This study aimed to investigate whether the application of anodic tDCS over the left inferior frontal gyrus (referred to as Broca’s area) alongside with language training can promote the articulatory problems in naming test in a non-fluent aphasia patient with apraxia of speech. The results showed that the participant made progress in naming abilities when the language treatment was combined with tDCS and this improvement was clinically significant.
These findings replicate previous studies of treating apraxia of speech with language therapy concomitant with tDCS [22, 23, 24]. Also our findings are in line with previous researches that showed associating specific language therapy with anodic uni-hemispheric tDCS stimulation over the perilesional language areas can promote the results of the treatment [19, 20, 21].
The mechanisms underlying the positive effects of tDCS on language recovery are unknown. Some authors proposed that anodic stimulation elicits a prolonged increment in cortical excitability, probably due to depolarization of the neuronal membrane and changes in the synaptic connections of the N-methyl-D-aspartate (NMDA) receptors involved in long-term potentiation [28, 29]. Maybe this was the case for our subject, and anodic stimulation over Broca's area increased the activity of not injured areas associated with Broca's area, and these areas compensate for speech articulation difficulties, but this claim needs more evidence especially with neuroimaging studies like fMRI.
Researches showed that unimpaired brain tissue can be modulated by various factors like behavioral training and neuromodulator therapies like noninvasive tDCS of the brain [13]. Concerning the similar mechanism of action of these approaches, which is, both make similar changes in the neural excitability of the impaired area, it could be reasonable to use this strategy together for better outcomes. The result of this study can be a support for this hypothesis as speech therapy alongside with tDCS increased the naming accuracy of an aphasic patient with apraxia of speech.
The improvement of the subject in this study in naming task after stimulating left inferior frontal area alongside with word repetition treatment could be because of patient improvement in motor planning for speech production, and this may be a confirmation for the results of previous studies that damage to left Broca's area is responsible for motor functions of speech [6, 7].
Together, this study only carried out on a single aphasic patient, therefore it precludes any conclusive claims regard efficacy of treatment with tDCS on improvement of acquired apraxia of speech, but it supports the claim that associating the language therapy of aphasia with tDCS can have a positive effect on rehabilitation outcome, and maybe in future more studies can be done to investigate the effect of tDCS on treatment of apraxia of speech in aphasic patients.
Conflict of Interest
The authors declare no conflict of interest.
Acknowledgment
Authors want to thank Tehran University of Medical Sciences for supporting this study. Also they appreciate Prof. Michael Nitsche for his guidance and support during this study.
References
-
McNeil MR, Ballard KJ, Duffy JR, Wambaugh J (2017) Apraxia of speech theory, assessment, differential diagnosis, and treatment: Past, present, and future. Speech motor control in normal and disordered speech: Future developments in theory and methodology, pp: 195-221.
-
Duffy JR (2013) Motor Speech disorders-E-Book: Substrates, differential diagnosis, and management: Elsevier Health Sciences.
-
McNeil M (2000) Apraxia of speech: A treatable disorder of motor planning and programming. Aphasia and Language. Theory to Practice, pp: 221- 266.
-
Ziegler W (2008) Apraxia of speech. Handbook of clinical neurology 88: 269-285.
-
McNeil MR, Robin DA, Schmidt RA (1997) Apraxia of speech: Definition, differentiation, and treatment. Clinical management of sensorimotor speech disorders 1: 311-344.
-
Hillis AE, Work M, Barker PB, Jacobs MA, Breese EL, et al. (2004) Re‐examining the brain regions crucial for orchestrating speech articulation. Brain 127(7): 1479-1487.
-
Richardson JD, Fillmore P, Rorden C, LaPointe LL, Fridriksson J (2012) Re-establishing Broca’s initial findings. Brain and language 123(2): 125-130.
-
Dronkers NF (1996) A new brain region for coordinating speech articulation. Nature 384(6605): 159-161.
-
Peach RK, Tonkovich JD (2004) Phonemic characteristics of apraxia of speech resulting from subcortical hemorrhage. Journal of Communication Disorders 37(1): 77-90.
-
Square P (1994) Nature and treatment of neuromotor speech disorders in aphasia. Language intervention strategies in adult aphasia, pp: 467-499.
-
Rosenbek J, Hansen R, Baughman CH, Lemme M (1974) Treatment of developmental apraxia of speech: A case study. Language, Speech, and Hearing Services in Schools, pp: 13-22.
-
Lindenberg R, Renga V, Zhu L, Nair D, Schlaug G (2010) Bihemispheric brain stimulation facilitates motor recovery in chronic stroke patients. Neurology 75(24): 2176-2184.
-
Bolognini N, Pascual-Leone A, Fregni F (2009) Using non-invasive brain stimulation to augment motor training-induced plasticity. Journal of neuroengineering and rehabilitation 6(1): 8.
-
Hummel F, Celnik P, Giraux P, Floel A, Wu WH, et al. (2005) Effects of non-invasive cortical stimulation on skilled motor function in chronic stroke. Brain 128(3): 490-499.
-
Boggio PS, Rigonatti SP, Ribeiro RB, Myczkowski ML, Nitsche MA, et al. (2008) A randomized, double-blind clinical trial on the efficacy of cortical direct current stimulation for the treatment of major depression. International Journal of Neuropsychopharmacology 11(2): 249-254.
-
Ferrucci R, Mameli F, Guidi I, Mrakic-Sposta S, Vergari M, et al. (2008) Transcranial direct current stimulation improves recognition memory in Alzheimer disease. Neurology 71(7): 493-498.
-
Mrakic-Sposta S, Marceglia S, Mameli F, Dilena R, Tadini L, et al. (2008) Transcranial direct current stimulation in two patients with Tourette syndrome. Mov Disord 23(15): 2259-2261.
-
Baker JM, Rorden C, Fridriksson J (2010) Using transcranial direct-current stimulation to treat stroke patients with aphasia. Stroke 41(6): 1229-1236.
-
Fiori V, Coccia M, Marinelli CV, Vecchi V, Bonifazi S, et al. (2011) Transcranial direct current stimulation improves word retrieval in healthy and nonfluent aphasic subjects. Journal of cognitive neuroscience 23(9): 2309-2323.
-
Fridriksson J, Richardson JD, Baker JM, Rorden C (2011) Transcranial direct current stimulation improves naming reaction time in fluent aphasia: a double-blind, sham-controlled study. Stroke 42(3): 819-821.
-
Monti A, Ferrucci R, Fumagalli M, Mameli F, Cogiamanian F, et al. (2013) Transcranial direct current stimulation (tDCS) and language. J Neurol Neurosurg Psychiatry 84(8): 832-842.
-
Marangolo P, Fiori V, Cipollari S, Campana S, Razzano C, et al. (2013) Bihemispheric stimulation over left and right inferior frontal region enhances recovery from apraxia of speech in chronic aphasia. European Journal of Neuroscience 38(9): 3370-3377.
-
Marangolo P, Fiori V, Di Paola M, Cipollari S, Razzano C, et al. (2013). Differential involvement of the left frontal and temporal regions in verb naming: a tDCS treatment study. Restorative Neurology and Neuroscience 31(1): 63-72.
-
Marangolo P, Marinelli CV, Bonifazi S, Fiori V, Ceravolo MG, et al. (2011) Electrical stimulation over the left inferior frontal gyrus (IFG) determines long- term effects in the recovery of speech apraxia in three chronic aphasics. Behavioural brain research 225(2): 498-504.
-
Nilipour R (2002) Farsi Naming Test. University of Walfare and Rehabilitation Sciences publisher, Tehran.
-
Nitsche MA, Doemkes S, Karaköse T, Antal A, Liebetanz D, et al. (2007) Shaping the effects of transcranial direct current stimulation of the human motor cortex. Journal of neurophysiology 97(4): 3109-3117.
-
Jacobson NS, Truax P (1992) Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. J Consult Clin Psychol 59(1): 12-19.
-
Nitsche MA, Paulus W (2000) Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. The Journal of physiology 527(3): 633-639.
-
Nitsche MA, Paulus W (2001) Sustained excitability elevations induced by transcranial DC motor cortex stimulation in humans. Neurology 57(10): 1899- 1901.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury