Management of the Child’s Neuroblastoma in the Pediatric Oncology Department of Mustapha Pacha University Hospital
We present our experience of neuroblastoma through a 5-year retrospective study carried out in the pediatric oncology department of Mustapha Pacha University Hospital. A total of 57 cases of neuroblastoma were identified. The boy / girl sex ratio was 1/1. The age distribution was homogeneous between the two sexes. In this study 33 children were between 0 and 18 months old and 24 were over 18 months old. Thirty children were metastatic at diagnosis. The hepatic localizations were the most frequent with 13 cases followed by the osteomedullary localizations. The renal localization was represented by 5 cases, the other lymph node, mandibular, paravertebral, mediastinal localizations counted only one case each. The patients stage IV represented 33% of patients, stage III 12%, stages II 8% and stages I 4%, It was possible to operate immediately on 10 patients or 17.7% of cases. Chemotherapy was given to 47 / 57 patients or 82%. After chemotherapy, 27 patients (47.4%) were judged inoperable. Among operated patients, only 4 had complete resection (7% of them).
Introduction
Neuroblastoma originates from the neural crest which usually gives birth to the adrenal medulla and sympathetic glands [1, 2, 3]. It is a tumor of infants and young children and represents approximately 10% of malignant diseases of children and comes in 3rd place after malignant hemopathies and tumors of the central nervous system. The abdominal localizations are the most frequent [1]. It is a tumor which presents a large progressive heterogeneity with certain forms progressing towards a spontaneous regression and others resistant to intensive therapeutics. Advances in pathology, immunohistochemistry and molecular biology in particular have made it possible to individualize different groups and to adapt therapy as best as possible [2].
Objectives
Describe our experience, evaluate and analyze our results in order to improve them.
Material and Methods
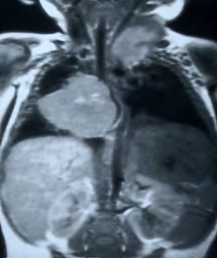
We present to you our experience of neuroblastoma through a 5-year retrospective study carried out in the pediatric oncology department. The recording of patients was done ona file previously established by ourselves including all the patient’s demographic characteristics and data relating to his illness after consultation of his medical file. The data analysis was done using Microsoft Excel software, Epi-info. We have described the demographic data: age, sex, clinical data, pathology, and management. The diagnostic assessment was made by imaging the radiography without preparation; a chest radiograph an abdominal echography first examination which shows a mass extrarenal retroperitoneal computed tomography and or magnetic resonance imaging, biological examinations assay of urinary metabolites of catecholamines HVA ), VMA , and Dopamine. The assessment of disease extension included a MIBG scan : with MIBG, a bone scintigraphy with non-fixing technetium with MIBG and Myelograms and bone biopsy puncture in search of spinal metastases (Figure 1 A, B and C). Treatment includes chemotherapy, surgery and or radiation therapy.

The indications were brought as a function of the age of the initial localization of the tumor of the extension stage and of biological prognostic factors and in particular N-Myc.and after multidisciplinary consultation in the committee The toxicity of chemotherapy was evaluated by the WHO grading or Lansky score which includes the score, the grading of Hematological, digestive, hepatic, renal and neurological toxicity The response to treatment was evaluated according to the recommendations of the SIOP.
Figure 1 : A: Thoracic neuroblastoma; B: Left adrenal neuroblastoma; C:MIBG scintigraphy shows with spinal cord compression in MRI multiple bone metastases
Results
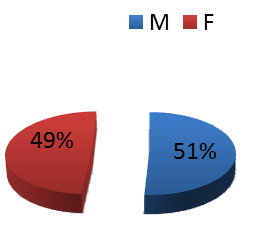
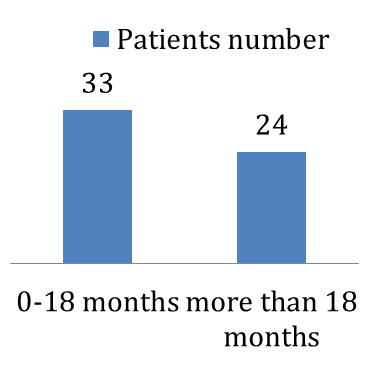
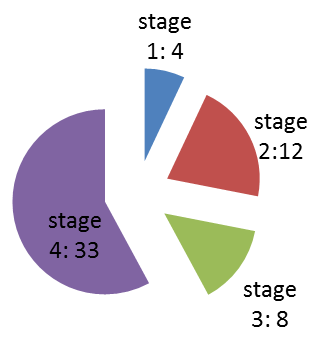
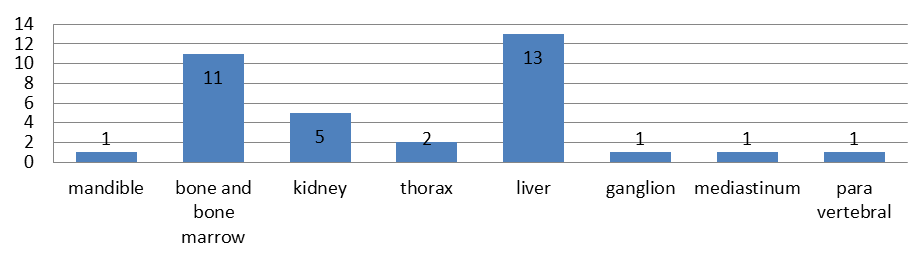
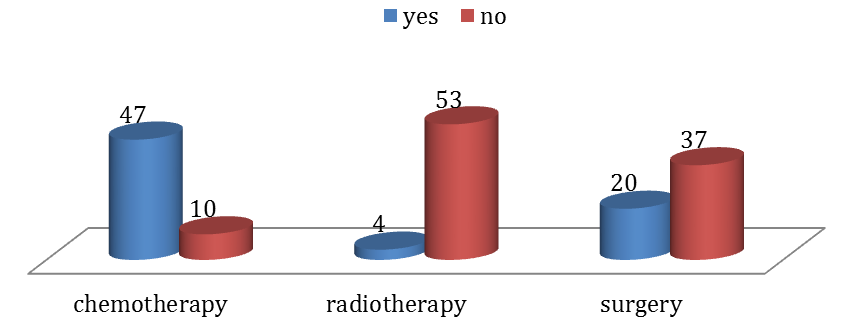
A total of 57 cases of neuroblastoma were identified. The boy / girl sex ratio was 1/1(Figure 2). The age distribution was homogeneous between the two sexes .In this study 33 children were between 0 and 18 months old and 24 were over 18 months old (Figure 3). Thirty children were metastatic at diagnosis. The hepatic localizations were the most frequent with 13 cases followed by the osteomedullary localizations. The renal localization was represented by 5 cases, the other lymph node, mandibular, paravertebral, mediastinal localizations counted only one case each (Figure 5). The patients stage IV represented 33% of patients; stage III 12%, stages II 8% and stages I 4% (Figure 4). It was possible to operate immediately on 10 patients or 17.7% of cases. Chemotherapy was given to 47 / 57 patients or 82%. The treatment consisted of the administration of 4 alternating cycles of CADO / VP16 + Carboplatin or cisplatinum cures according to the LMB protocol of the SIOP, in hospital (05 days minimum) and systemically and in possible association with rHu G-CSF. ). After chemotherapy, 27 patients (47.4%) were judged inoperable. Among the patients operated, only 4 patients had complete resection (7% of them) (Figure 6).
Evolution
The follow-up of our patients was 66 months. The overall monitoring for all stages of the disease was 68.57% at 12 months and it stabilized at 52.16% until 66 months (Figure 7).
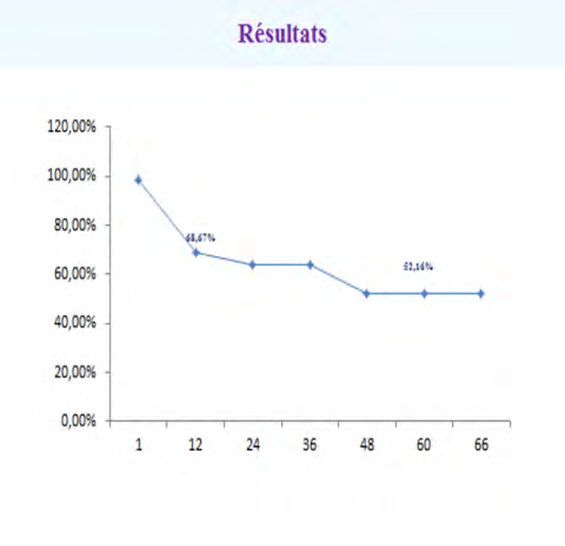
Figure 7 : Follow-up of patients for 66 months.
For metastatic patients we had very early deaths up to 3 months of evolution then a regular decrease to represent only 32.13% of the patients (Figure 8).
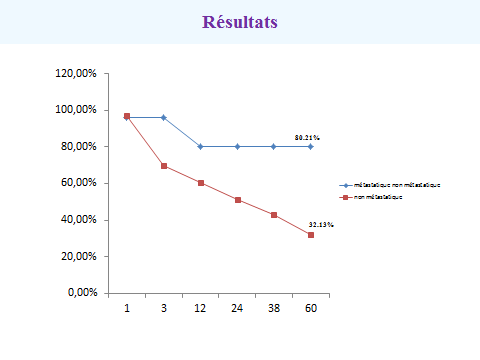
Figure 8 : Patient survival curve.
Discussion
The results of our study are disappointing. The management of these tumors is multidisciplinary to improve our results we must act at all stages of treatment [3, 4]. For medical treatment, it is necessary to shorten the diagnostic and treatment times [5]. It is necessary to have genetic and molecular biology examinations to have an accurate prognosis [4] and [6]. Chemotherapy does not manage to make operable the locally advanced stages. It is currently accepted in all protocols that chemotherapy in the attack phase obtains CR or BRP only in 45 to 60% after surgery, hence the need to treat the residual disease [5].
Intensification with HD chemotherapy followed of a stem cell self-transplant obtains a survival benefit which we cannot achieve in our department; we cannot do high-dose chemotherapy without a protected unit.
Conclusion
Neuroblastoma is a very polymorphic tumor. Despite significant diagnostic and therapeutic advances, there remains a serious tumor in some forms, warranting further research. The clinical stage and age at diagnosis are major prognostic factors, but they are the result of a genotype. Genotyping gives an excellent reflection of the prognosis in its absence, it is necessary to rely on the usual criteria (Stage, Age, Histopronostic if St <IV). Despite the progress made in the evaluation of the extension and the knowledge of clinical and biological prognostic factors the therapeutic results are still insufficient the survival currently of this type of tumors does not exceed 45% 5-year survival. A lot of research is underway to find new solutions: intraoperative radiotherapy, metabolic radiotherapy, specific antibodies, agents inducing cell differentiation, immunotherapy, anti-angiogenic agents
References
-
Cohn SL, Pearson AD, London WB, Monclair T, Ambros PF, et al. (2008) The International Neuroblastoma Risk Group (INRG) Classification System: An INRG Task Force Report. J Clin Oncol 27(2): 289-297.
-
Peuchmaur M, d’Amore ES, Joshi VV, Hata J, Roald B, et al. (2003) Revision of the international neuroblastome pathology classification: confirmation of favorable and unfavorable prognostic subsets in ganglio neuroblastoma, nodula Cancer 98(10): 2274-2281.
-
Perez CA, Matthay KK, Atkinson JB, Seeger RC, Shimada H, et al. (2000) Biologic variables in the outcome of stages I and II neuroblastoma treated with surgery as primary therapy : A Children’s Cancer Group study. J ClinOncol 18(1): 18-26.
-
Rubie H, Hartmann O, Michon J, Frappaz D, Coze C, et al. (1997) N-myc gene amplification is a major prognostic factor in localized neuroblastoma : Results of the French NBL 90 Study. J ClinOncol 15: 1171-1182.
-
Matthay KK, Villablanca JG, Seeger RC, Stram DO, Harris RE, et al. (1999) Treatment of high-risk neuroblastoma with intensive chemotherapy, radiotherapy, autologous bone marrow transplantation and 13-cisretinoic acid. N Engl J Med 341(6): 1165-1173.
-
Park R, Eggert A, Caron H (2008) Neuroblastoma: Biology, prognosis and treatment. Pediatr. Clin N Am 55(1): 97-120.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury