A Review on New Trends of Artificial Intelligence in Medicine
Computer science’s artificial intelligence division is able to analyse intricate medical data. They can be employed in various clinical contexts for diagnosis, treatment, and outcome prediction due to their capacity to exploit important relationships within a data set. The terms “artificial intelligence” and “neural networks (computer)” were used in searches on Medline and the internet. By cross-referencing important papers, further references were found. This study presents an overview of several artificial intelligence approaches and an evaluation of significant therapeutic applications. Nearly every area of medicine has investigated the effectiveness of artificial intelligence methods. While fuzzy expert systems, evolutionary computation, and hybrid intelligent systems are examples of artificial intelligence techniques, artificial neural networks were the most widely utilised analytical tool. Medicine is becoming increasingly interested in explainable artificial intelligence (AI). In a technical sense, is an age-old issue in artificial intelligence, and traditional AI methods aimed to be understandable and traceable. Their inability to handle the uncertainties of the actual world was a drawback, though. Applications grew more and more successful when probabilistic learning was introduced, but they also became more and more opaque. The introduction of traceability and transparency in statistical black-box machine learning techniques, especially deep learning (DL), is the focus of explainable AI. Artificial intelligence is a branch of computer science that can assess complex medical data. Their capacity to find and use meaningful links in a dataset can be used for outcome prediction, therapy, and diagnosis in a variety of therapeutic settings. Additional references were found by cross-referencing significant articles. This paper presents an overview of numerous artificial intelligence algorithms and reviews important therapeutic applications. Every field of medicine has looked into how well artificial intelligence tools work. Artificial neural networks were the most widely used analytical tool; other artificial intelligence techniques included fuzzy expert systems, evolutionary computation, and hybrid intelligent systems.
Abbreviations
AI: Artificial Intelligence; DL: Deep Learning; ML: Machine Learning; ANNs: Artificial Neural Networks; CAD: Computer Assisted Diagnosis; NIH: National Institutes of Health; ISPE: International Society for Pharmaceutical Engineering.
Introduction
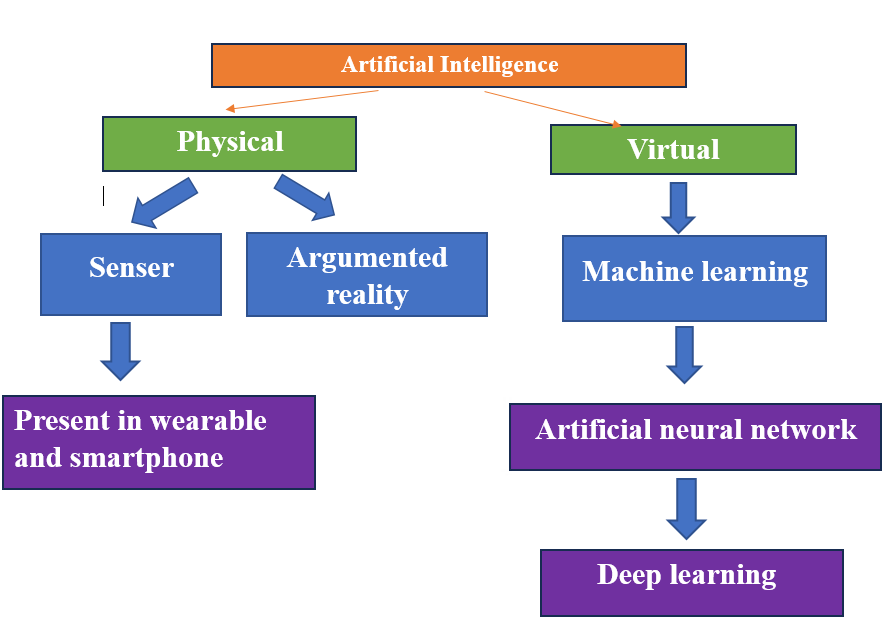
Turing (1950) was a pioneer of AI and contemporary computing. The “Turing test” was developed on the premise that intelligent computer behaviour is demonstrated by its capacity to accomplish cognitively demanding activities at a level comparable to that of a human. AI enjoyed a boom in popularity in the 1980s and 1990s. Various clinical contexts in the healthcare industry have employed artificial intelligence approaches, including hybrid intelligent systems, artificial neural networks, fuzzy expert systems, and Bayesian networks. Comparing healthcare applications to other industries, the healthcare sector received the largest portion of investments in AI research in 2016. Virtual and physical AI are the two categories of AI in medicine. Applications like electronic health record systems and neural network- based treatment decision guidance are examples of the virtual portion. The physical portion covers with aged care, intelligent prosthetics for the disabled, and robots helping with surgery. Establishing clinical correlations and insights through the creation of relationships and patterns from the available database of data are the cornerstone of evidence- based medicine. To find these patterns and correlations, we used to apply statistical techniques [1, 2].
Flowcharts and the database approach are two general methods that computers use to learn the art of patient diagnosis. With the flowchart-based method, a doctor asks a series of questions to get a probable diagnosis by integrating the symptoms they present with one another. This is a translation of the history-taking process. This necessitates loading a substantial amount of data onto machine-based cloud networks, given the variety of illness processes and symptoms seen in everyday medicine. This method has limited results since the machines cannot detect and collect cues that a doctor can only see during a patient encounter. The database technique, on the other hand, makes use of the deep learning or pattern recognition concept, which entails teaching a computer to recognise particular groups of symptoms or specific clinical or radiological pictures through repeated procedures. The 2012 debut of Google’s artificial brain project serves as an illustration of this strategy. Using information from 10 million YouTube videos, this system taught itself to identify cats. As it viewed more and more photos, its accuracy increased. It learned in three days and was able to predict a picture of a cat with 75% accuracy.
Perhaps the oldest branch of computer science, artificial intelligence (AI) covers a wide range of topics, including creating systems that can learn and think like people and simulating cognitive processes for the purpose of solving problems in the real world. As a result, to distinguish it from human intelligence, it is frequently referred to as machine intelligence. The field was centred on the nexus of computer science and cognitive science. Nowadays, AI is a very popular topic because of machine learning’s (ML) practical achievements. Explain ability and AI has always been closely related. McCarthy’s 1958 proposal of the Advice Taker, a “programme with common sense,” is one of the earliest examples of this. It was most likely the first time that the ability to reason with common sense was suggested as the secret of AI. With the goal of creating software that can automatically learn from past data to gain knowledge from experience and gradually improve its learning behaviour to make predictions based on fresh data, machine learning (ML) is a very useful area of artificial intelligence. Making sense of the world, comprehending context, and making decisions in the face of ambiguity are the three great problems. AI’s workhorse, machine learning (ML), is becoming increasingly widely used in business, engineering, and science. This is leading to a greater emphasis on evidence-based decision- making. Large data sets, inexpensive computing, and the creation of new statistical learning algorithms have all contributed to the tremendous advancements in machine learning. Deep learning is one technique that is very popular these days [1, 3, 4].
A family of machine learning models with a lengthy history, DL is based on deep convolutional neural networks. Because they are producing incredible outcomes even at human performance levels, DL is highly popular these days. The Thrum group’s latest work serves as an example of best practise; using a DL technique, they attained performance comparable to that of medical physicians, showing that these approaches can classify skin cancer with a level of competence on par with human dermatologists. The encouraging findings in the identification of diabetic retinopathy and related eye illnesses provide as another illustration. All of these are excellent illustrations of the advancement and utility of artificial intelligence; however, even the most well-known proponents of these techniques have recently noted how challenging it is to achieve usable intelligence because, in addition to learning from past data, extracting knowledge, generalising, and overcoming the curse of dimensionality, we also need to separate the underlying explanatory factors of the data in order to comprehend the context in an application domain where a doctor-in-the-loop is still necessary.
One of the biggest applications of AI, ML, and DL is medicine. We deal with probabilistic, unknown, incomplete, imbalanced, heterogeneous, noisy, unclean, erroneous, inaccurate, and missing data sets in arbitrarily high- dimensional domains when we assist medical decisions. Frequently, we just lack vast data sets. Future medical research aims to model patient complexity in order to customise treatments, medical decisions, and healthcare procedures for each unique patient. This presents difficulties, namely in the mapping, integration, and fusion of diverse distributed and heterogeneous data, as well as in the visual interpretation of these heterogeneous data. Explainable AI in the medical domain must therefore consider that a variety of data sources may contribute to an important outcome. The need for AI techniques in the medical field that not only work effectively but also are transparent, dependable, understandable, and comprehensible to human experts for instance, a natural language sentence in the field is expanding. To replicate and understand the learning and knowledge extraction process, as well as to reenact the machine decision-making process, methods and models are required. This is significant because comprehending the causal relationship between learned representations is essential for decision support [5, 6, 7].
Importance: To support the medical professional in diagnosing a patient, choosing a course of treatment, and projecting the patient’s result. They are intended to assist healthcare staff with tasks that require the manipulation of information and data as part of their daily responsibilities. Artificial neural networks (ANNs), fuzzy expert systems, hybrid intelligent systems, and evolutionary computation are a few examples of these systems. Synthetic neural networks ANN is the most widely used AI method in medicine, based on the amount of publications over the past two decades. Six Artificial neural networks (ANNs) are computer analytical tools modelled after the biological nervous system. Their structure consists of networks of highly interconnected computer processors known as “neurons,” which can process data and express knowledge in parallel. Their capacity to draw conclusions from past examples, analyse non-linear data, deal with imprecise information, and generalise, allowing the model to be used to independent data, has made them an extremely appealing analytical tool in the medical area. The first artificial neural network was created in 1943 by McCulloch and Pitts using straightforward binary threshold functions. The creation of the Perceptron as a useful model by psychologist Frank Rosenblatt in 1958 marked the next significant turning point. Several iterations of the fundamental Perceptron network have been suggested, with the multilayer feed forward Perceptron being the most widely used model. Each layer in these networks is fully connected to every other layer. Typically, there are three layers of neurons: an input layer, one or more middle or hidden layers, and an output layer. A numerical weight is assigned to each link that connects the neurons. Repetitive changes to these weights allow a neural network to “learn.” The capacity of artificial neural networks (ANNs) to learn from their experiences in a training environment is one of their key characteristics. Before “backpropagation” learning was established by PhD student Paul Werbos in 1974, the usage of multilayer feed forward Perceptron’s was limited due to the lack of an appropriate learning method. The Self-Organizing Feature Map, Hopfield networks, and Radial Basis Function are a few other well-liked network architectures. Artificial neural networks (ANNs) have already found several practical uses. Each layer in these networks is fully connected to every other layer. Typically, there are three layers of neurons: an input layer, one or more middle or hidden layers, and an output layer. A numerical weight is assigned to each link that connects the neurons. Repetitive changes to these weights allow a neural network to “learn.” The capacity of artificial neural networks (ANNs) to learn from their experiences in a training environment is one of their key characteristics. Before “back propagation” learning was established by PhD student Paul Werbos in 1974, the usage of multilayer feed forward Perceptrons was limited due to the lack of an appropriate learning method. The Self-Organizing Feature Map, Hopfield networks, and Radial Basis Function are a few other well-liked network architectures. Artificial neural networks (ANNs) have already found several practical uses [8, 9, 10].
Classification
Artificial Intelligence in Medicine
The Virtual Branch: There is two primary areas of AI application in medicine: virtual and physical. Machine learning, also known as deep learning, is a virtual component that is represented by mathematical algorithms that enhance learning by experience. Three categories of machine learning algorithms exist: (i) unsupervised algorithms, which rely on pattern recognition; (ii) supervised algorithms, which use prior instances to classify and predict; and (iii) reinforcement learning.
Artificial Intelligence in Medicine
The Physical Branch: Physical things, medical equipment, and more complex robots that assist in providing care (carebots) are all included in the second way that artificial intelligence is being used in medicine. The use of robots as assistants for instance, a robot companion for the elderly population experiencing cognitive decline or limited mobility may be the most promising strategy. The most advanced models of this technology are carebots made in Japan. Robots can operate alone or as a surgeon’s help in surgery. Use of Robots to Monitor Effectiveness of Treatment: Additionally, robots can be helpful in assessing how human performance has changed in contexts like rehabilitation. AI might also be used to monitor the directed distribution of medications to certain organs, tissues, or tumours. The recent development of nanorobots, for instance, to address delivery issues resulting from medicinal agent dispersion difficulties into a target region, is a promising development. This issue comes up [1, 3, 11].
AI is becoming more and more prevalent in the field of public health, and it will significantly alter every facet of primary care (Figure 1).
AI-powered computer programmes will assist primary care doctors in more accurately identifying patients who need special care and in developing protocols that are tailored to each patient. AI can be used by primary care doctors to take notes, evaluate patient conversations, and upload necessary data straight into electronic health record systems. Primary care doctors will be able to view patient data collected and analysed by these applications, together with information about the patients’ medical need.
According to a 2016 survey, doctors spend 27% of their workdays in direct clinical face-to-face interactions with patients and 49.2% of their workdays on desk work and electronic medical data. 52.9% of the time that doctors were in the examination room with patients, they were working on other tasks on the EHR. In summary, compared to doctors who did not utilise these services, doctors who utilised documentation support services like dictation help or medical scribe services spent more face-to-face time with patients. Additionally, more AI is being used in medicine to improve productivity, accuracy, and efficacy in addition to reducing manual labour and freeing up time for primary care physicians.
Clinical trials that search for and develop pharmacological compounds to treat a particular ailment take years and cost billions of dollars. In a recent instance, artificial intelligence (AI) was utilised to screen for drugs that were already on the market and might be used to combat the Ebola virus, which would have taken years to treat otherwise. We could accept the novel idea of “precision medicine” with the aid of AI .There have been trials where AI systems have properly classified worrisome skin lesions in more cases than dermatologists. This is due to the fact that AI systems are significantly more capable of learning from subsequent cases than a clinician could ever handle in a mortal lifetime, and they can be exposed to numerous examples in a matter of minutes. When professionals frequently disagree on a diagnosis, such pulmonary tuberculosis on a chest radiograph, AI- based decision-making techniques are applied. There are just as many people who are sceptical as supporters of this new era of AI-augmented practise. Numerous aspiring and practising physicians are concerned about the decline in employment prospects resulting from the growing use of technology. Though some human qualities, including critical thinking, interpersonal and communication skills, emotional intelligence, and creativity, cannot be taught to machines, they may be able to translate human behaviour analytically and logically [1, 12].
Advantages and Disadvantage of AI in Medicine
| Disadvantage | Advantages |
|---|---|
| Loss of job | Efficiency, accuracy, precision |
| Lack of human touch empty emotional intelligence | Decrease workload |
| Save money , better monitoring |
In 2016, the Digital Mammography DREAM Challenge was done where several networks of computers were connected, and the goal was to establish an AI-based algorithm by reviewing 640,000 digital mammograms. The best which was achieved was a specificity of 0.81, sensitivity of 0.80, area under receiver operator curve was 0.87, which is roughly approximated to bottom 10% radiologists. In conclusion, AI has potential, but it is unlikely that AI will replace doctors out rightly.AI would be an integral part of medicine in the future (Figure 2). Hence, it is important to train the new generation of medical trainees regarding the concepts and applicability of AI and how to function efficiently in a workspace alongside machines for better productivity along with cultivating soft skills like empathy in them.
Ultimately, it is critical that primary care physicians become knowledgeable about the latest developments in artificial intelligence as well as the uncharted medical ground that the field is exploring. A finely balanced, mutually beneficial combination of the human skills and judgement of skilled primary care physicians with the efficient application of automation and artificial intelligence (AI) should be the aim. This is crucial since it raises concerns that the potential benefits of AI in medicine could be hampered if it were to totally replace human .In the medical field, artificial intelligence is already being used extensively. Examples include online appointment scheduling, online check-ins at medical centres, digitization of medical records, calls to remind patients of follow-up appointments and immunisation dates for children and pregnant women, drug dosage algorithms, and warnings about potential side effects when prescribing multiple medications. The many uses of AI in medicine are summed up in the pie graphic [13, 14].
Applications of Artificial Intelligence in Health Care
The medical field that has been most accepting of new technology utilisation is radiology. Computers were first utilised in clinical imaging for administrative tasks including image acquisition and storage. With the development of picture archiving and communication systems, computers have now evolved into an essential part of the workplace. It is commonly recognised that computer-assisted diagnosis, or CAD, is used during screening mammography. According to recent research, CAD is not a very useful diagnostic tool in terms of positive predictive values, sensitivity, and specificity.
The University of Massachusetts developed the DX plain decision support system in 1986. It provides a list of likely differentials based on the symptom complex and is used as an instructional tool for medical students to fill in the information gaps not covered in traditional textbooks. The University of Washington created the Germwatcher system to identify and look into hospital acquired illnesses. Patients in the UK can use an internet application called Babylon to obtain test kits, check for symptoms, seek advice and speak with a doctor. In addition, the range of AI has grown to include medicinal applications.
Surgery has undergone a transformation thanks to Intuitive Surgical Da Vinci robotic surgical system, particularly in the fields of gynaecological and urological surgery. The system’s robotic arms can more accurately replicate a surgeon’s hand movements, and its 3D vision and magnification choices let the surgeon make tiny incisions. Since 2018, Buoy Health and the Boston Children’s Hospital have been working together on a web interface-based artificial intelligence (AI) system that gives parents advice regarding their sick child by responding to inquiries about medications and whether or not symptoms call for a trip to the doctor. The Cure App, developed by the National Institutes of Health (NIH), lowers non adherence rates by tracking patients’ medicine use through smartphone camera access [15, 16].
In addition to existing inventions, several advancements are being developed that will improve the quality of medical care provided by doctors. One of the best examples of this is IBM’s Watson Health, which will be able to recognise cancer and heart disease signs with ease. AI-assisted care (PAC) is a programme that Stanford University is developing. With the use of several sensors, PAC’s intelligent senior wellbeing support system and smart ICUs can detect any changes in the behaviour of old individuals living alone or ICU patients, respectively. Additionally, PAC is expanding its efforts to include conversational agents for healthcare and support for intelligent hand hygiene.
In order to achieve flawless hand hygiene for doctors and nursing personnel and lower hospital acquired infections, hand hygiene support uses depth sensors to refine computer vision technology. In order to help patients seek care sooner, healthcare conversational initiatives examine how mobile phone users ask inquiries about physical health, mental health, and interpersonal violence and how Siri, Google Now, S voice, and Cortana answer. A virtual nurse named Molly is being created to provide discharged patients follow-up treatment so that doctors can concentrate on more urgent cases [17, 18].
Applications of Artificial Intelligence in Medicine
Cardiology
Atrial Fibrillation: One of the first uses of AI in medicine was the early diagnosis of atrial fibrillation. In 2014, the FDA approved Alive Cor’s Kardia mobile application, which enables smartphone-based ECG monitoring and atrial fibrillation identification. According to the recently completed REHEARSE-AF study, mobile patients’ remote ECG monitoring with Kardia has a higher detection rate of atrial fibrillation than standard treatment. Additionally, Apple received FDA certification for their Apple Watch 4, which makes it simple to collect an ECG and diagnose atrial fibrillation. This information may then be transmitted with the preferred practitioner via a smartphone. Numerous criticisms of wearable and portable ECG systems have been discussed, pointing out drawbacks like false positive rates that result from movement artefacts and obstacles.
Cardiovascular Risk
Artificial intelligence (AI) has been used to predict the risk of cardiovascular disease, such as acute coronary syndrome and heart failure, more accurately than traditional scales when applied to electronic patient records. However, recent thorough evaluations have documented how the sample size employed in a study report might affect the outcomes.
Pulmonary Medicine
According to reports, one area where AI applications in pulmonary medicine show promise is the interpretation of lung function testing. According to a new study, artificial intelligence (AI)-based software facilitates decision- making by offering more precise interpretation and acting as a decision support tool when analysing findings from pulmonary function testing. One of the criticisms levelled at the study noted that the pulmonologists who took part in it had a far lower accurate diagnosis rate than the national average.
Endocrinology
Patients with diabetes can examine interstitial glucose readings in real time and receive information on the direction and rate of change of blood glucose levels thanks to continuous glucose monitoring. Medtronic’s smartphone- paired Guardian glucose monitoring system was approved by the FDA. With the Watson AI system created by IBM, the company joined in 2018 to offer their Sugar. IQ solution, which helps clients better prevent hypoglycemia episodes through frequent measurement. Patients can improve their blood glucose control and lessen the stigma attached to hypoglycemic episodes with continuous blood glucose monitoring. However, a study on patients’ experiences with glucose monitoring found that although participants expressed confidence in the notifications, they also expressed feelings of personal failure to control their blood glucose levels.
Nephrology
Artificial intelligence has been used in clinical nephrology in a number of contexts. Examples include predicting the progression of IgA nephropathy and determining risk for glomerular filtration rate reduction in patients with polycystic kidney disease. Nonetheless, a recent study notes how the sample size required for inference currently limits research.
Gastroenterology
Gastroenterology is a specialty that benefits from a broad range of AI uses in clinical settings. Among other deep learning models, gastroenterologists employed convolutional neural networks to interpret endoscopy and ultrasound pictures and identify anomalous structures like colonic polyps. In addition to being used to diagnose atrophic gastritis and gastroesophageal reflux disease, artificial neural networks have also been used to predict outcomes related to gastrointestinal bleeding, esophageal cancer survival, inflammatory bowel disease, and metastasis in colorectal and esophageal squamous cell carcinoma.
Neurology
Epilepsy with continuous ambulatory monitoring, intelligent seizure detection devices represent a promising technological advancement in management. In 2018, the FDA approved Empatica’s wearable device, Embrace, which when used in conjunction with electrodermal captors can identify generalised epilepsy seizures and report the information to a mobile application that can notify trusted medical professionals and close family members about the patient’s location. According to a patient experience report, individuals with epilepsy showed great enthusiasm in wearing wearables and faced no obstacles when implementing seizure detection devices, unlike those using heart monitoring wearables.
Gait, Posture and Tremor Assessment
Wearable sensors have shown promise in helping individuals with multiple sclerosis, Parkinson’s disease, Parkinsonism, and Huntington’s disease statistically assess their gait, posture, and tremor.
Computational Diagnosis of Cancer in Histopathology
The FDA has granted Paige.ai breakthrough status for its AI-based system, which can accurately diagnose cancer in computational histopathology and free up pathologists’ time to work on critical slides.
Medical Imaging and Validation of AI-Based Technologies
The performance of radiologists and deep learning software in the field of imaging-based diagnosis was compared in a long-awaited meta-analysis. While deep learning appears to be just as effective in diagnosing as radiologists, the authors noted that 99 percent of studies lacked a robust design, and only one thousandth of the reviewed papers validated their findings using algorithms that diagnosed medical imaging from different source populations. These results confirm the necessity of conducting thorough clinical studies to validate AI-based technology.
Plain Film Radiography
With two billion conducted annually, the chest radiograph is the most common imaging examination in the world. The fact that chest radiography is widely available globally and can be used to diagnose a variety of illnesses explains its appeal. Moreover, chest radiographs have the largest availability of labelled pictures, which is the currency of AI research.
Applications in Pathology
Pathology has advanced more slowly to the digital media than radiology did from lighted X-ray films to digital imaging, which is where the adoption of AI depends. Pathologists can now view full histopathology slides in high resolution and with depth manipulation thanks to whole-slide imaging (WSI). Even with WSI’s availability and advantages, glass slide digital conversion is not a common practise. Technology is advancing quickly, making things faster.
Applications in Ophthalmology
One of the most prevalent disorders in general ophthalmology practise is diabetic eye disease, which is also a serious and expanding public health concern. The most prevalent cause of vision loss in working-age individuals is diabetic retinopathy (DR), which impacted 2.6 million people worldwide in 2015 and is predicted to affect 3.2 million by 2020. In higher-income nations, the prevalence of life-threatening diabetic retinopathy is declining as a result of improved diabetic management.
Applications in Dermatology
In the field of dermatology, the ability to recognise visual patterns is a crucial diagnostic skill. Artificial intelligence (AI) has the potential to significantly enhance picture processing and improve diagnostic precision in this domain. In visual image identification, recently developed computer neural networks have been used to diagnose skin problems and have shown equivalent, and often greater, sensitivity and specificity in classifying photos than even dermatologists with years of clinical experience.
For Challenges
The use of AI in healthcare will present a number of difficulties. To provide some context, we will highlight three that are related to the earlier investigations included in this paper: Over-fitting, the black box issue, and regulatory approval [10, 19].
Future Outlook
Weakly Supervised Learning
In the medical field, supervised learning is highly costly due to the difficulty in obtaining comprehensive ground-truth labels and robust supervision information. In particular, classifying a histological image is a crucial and time-consuming task for the diagnosis of cancer, since it is clinically significant to divide the cancerous tissues into several groups. The very large image size (and the associated problems for DL), the inadequately labelled images (the sparse training data available), the pathologist’s time required (expensive labelling), the insufficient labels (region of interest), the various levels of magnification (resulting in different levels of information), colour variation and artefacts (sliced and placed on glass slides), etc. Are some of the issues that are typically present in digital pathological image?
The phrase “weakly supervised learning” refers to a broad range of techniques for building predictive models by learning under insufficient, imprecise, or erroneous supervision. We wish to learn in a strong supervision task from the training data set where the feature space is and are always supposed to be identically and independently distributed data (which are not in real-world problems. scoring systems) We suggest classifying entire slide images in the context of weakly supervised learning using commonly-used based on correlation with histomorphological features and an overall predictive score. Additionally, we provide a relevance map created by watching the human expert during diagnosis making. The human causal model can be expanded using established human features in conjunction with novel multiscale morphological classifiers. Additionally, the CNN model can be clarified using established histomorphological features. In order to correlate chromatin organisation inside single cell nuclei—both benign and malignant with histopathological features and molecular markers, we propose to extract from these nuclei and classify them.
Research on structural causal models is a crucial area of focus. AI now operates in two modes: statistical and model- free. This implies Figure 3.

Structure Causal Model
Strict limitations on performance as well as efficacy. Strong AI cannot be supported by such systems since they are incapable of reasoning about interventions or reflection. AI needs the direction of a reality model, such the ones used in causal inference tasks, in order to reach human level intelligence. Therefore, in order to examine the underlying explanatory elements of the data, we propose to: (1) build novel visualisation techniques that can be educated by medical specialists; and (2) formalise a structural causal model of human decision making and map features in these to DL approaches [2, 12].
Develop Causability as a New Scientific Field
Numerous usability techniques have been devised by Community of human-computer interaction. In order to establish causability as a scientific field which will become necessary with increased use of AI we need to develop causability methodologies, methods, and tests that are similar to these usability methodologies, methods, and tests. These methods and tests must be based on precise scientific principles and theories of causality. Causability measures need to guarantee the “quality of explanations,” much as usability measures do [20, 21, 22, 23].
We must create techniques to assess effectiveness (does an explanation provide enough detail to describe a statement), efficiency (is this done with the least amount of time and effort), and user satisfaction (how satisfactory was the explanation for the decision making process) for each of these levels. It is important to reiterate that there are three categories of explanations: Three types of explanations are possible: (1) peer-to-peer, as in medical reporting; (2) educational, like in teacher-student interactions; and (3) scientific, like in the strict meaning of science theory. We want to be clear that the first kind of explanation is what we always refer to in this post [24].
Technology Transfer
What is technology transfer? A “logical procedure that controls the transfer of any process together with its documentation and professional expertise between development or manufacture sites” is the definition of technology transfer [25, 26, 27, 28, 29].
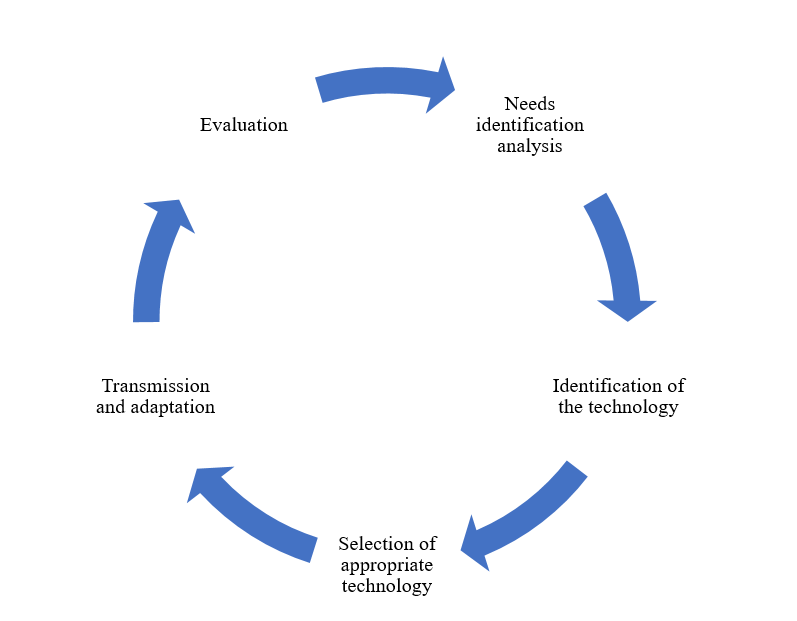
The process of finding new drugs and developing new medical goods depends heavily on technology transfer. It’s the procedure by which a technology inventor makes their creations available to a business partner so they can use them for profit (Figure 4).
In the pharmaceutical sector, “technology transfer” describes the methods by which a medicine is successfully discovered, developed, tested in clinical trials, and then brought to market on a large scale. For these researchers to materialise on a bigger scale for commercialization, particularly in the case of developing products, technology transfer is crucial. Technology transfer covers commercial operations like knowledge and skills in addition to patentable components of production. This Figure illustrates the many phases of technology transfer [30, 31, 32, 33, 34, 35, 36].
Facts of Technology Transfer
There are several methods that technology can be transferred. Public laboratories to private industry companies. Within the same nation’s private sector companies. Between foreign private sector companies. From commercial companies to academic institutions [37, 38].
WHO guidelines for Technology Transfer (TT)
Rather than providing rigorous, inflexible guidance, these guiding principles on technology transfer are meant to act as a framework within which flexibility can be used. In keeping with the WHO’s mandate, the quality aspects have been the focus. 1. Most goods undergo process transfers at some point during their lifetime, from development, scale- up, manufacture, production, and launch to the post-approval stage. 2. “A rational procedure that controls the transfer of any process together with its documentation and professional expertise between development and manufacture or between manufacture sites” is the definition of technology transfer. Therefore, in its 42nd report, the WHO Expert Committee on Specifications for Pharmaceutical Preparations advised that WHO address this issue by developing WHO guidelines on the subject. 5. Technology transfer calls for a planned, documented strategy with skilled workers operating inside a quality system, with data documentation encompassing all facets of development, production, and quality assurance. Sending units (SU), receiving units (RU), and the unit directing the process which might or might not be a different entity are typically present [39, 40, 41, 42, 43, 44, 45, 46].
Conclusion
One of the most important technologies in our economy right now is AI. It will usher in changes akin to those brought about by the invention of the steam engine or electricity. But worries over a possible loss of control in the interaction between humans and AI are becoming more prevalent. The public has long debated topics like autonomous driving and the vehicle’s imprecise decision-making, for instance, in extreme situations right before an accident. The issue of whether AI should or can assist in making medical decisions or even make them also stands to be addressed. It will frequently be required to evaluate the quality of the explanation and comprehend the process by which a machine judgement was made. In the modern world, deep learning algorithms are incredibly helpful for things like recommendation systems, face recognition, autonomous driving, and speech interpretation. Already perform admirably. People find it really challenging to comprehend how these algorithms arrive at a conclusion, nevertheless. These are essentially “black box” models. The issue with these models is that they don’t have an explicit declarative representation of knowledge, even if we comprehend the underlying mathematical theories and concepts. The purpose of early artificial intelligence (AI) solutions, which were referred to as expert systems at the time, was to make answers accessible, understandable, and hence explainable. This was attainable in very specific issues. Of course, it should be noted that there may be numerous issues for which there is never a need for an explanation [47, 48, 49].
In this context, “explainable AI” refers to more than just recorded expertise and knowledge obtained throughout research and/or commercialization to a suitable, accountable, and approved entity. 3. Little information on the topic from national or regional regulatory organisations was found in literature searches. The International Society for Pharmaceutical Engineering (ISPE) published guidelines for intra-company transfers. The dynamic business strategies of pharmaceutical businesses are characterised by a growing involvement in intra- and intercompany technology transfers. These transfers may occur due to several factors, including the requirement for increased capacity, relocation of operations, consolidations, and mergers not only essential and helpful, but also a great chance for AI solutions in general.
Pearl (2018) recently highlighted that the primary issue with the most effective machine learning systems today is that they operate in a statistical, or model-free, mode, which places severe restrictions on their functionality. Because these systems are incapable of comprehending context, they are unable to make sense of interventions or reflection. To address the “Why?” question, these methods require the direction of a human model akin to those employed in causality research (Pearl & Mackenzie). Here, the development of causality as a reliable scientific discipline can be beneficial.
Will Doctors be replaced by Artificial Intelligence?
Artificial intelligence is unlikely to replace doctors, as has been recently explored in the literature. Instead, smart medical technologies exist to help physicians and enhance patient management. However, as recent studies have shown comparisons between physicians and artificial intelligence solutions often take place, as though the two entities were in rivalry. Future research should compare medical professionals who use artificial intelligence solutions with those who do not, and should expand those comparisons to translational clinical trials. Only then will artificial intelligence be acknowledged as a medical professional’s ally.
References
-
Coppola F, Faggioni L, Gabelloni M, Vietro F, Mendola V, et al. (2021) Human, all too human? An all-around appraisal of the “artificial intelligence revolution” in medical imaging. Frontiers in Psychology 12: 710982.
-
Patel VL, Shortliffe EH, Stefanelli M, Szolovits P, Berthold MR, et al. (2009) The coming of age of artificial intelligence in medicine. Artificial intelligence in medicine 46(1): 5-17.
-
Briganti G, Moine O (2020) Artificial intelligence in medicine: today and tomorrow. Frontiers in medicine 7: 1-27.
-
Beam AL, Drazen JM, Kohane IS, Leong TY, Manrai AK, et al. (2023) Artificial intelligence in medicine. New England Journal of Medicine 388(13): 1220-1221.
-
Mesko B (2017) The role of artificial intelligence in precision medicine. Expert Review of Precision Medicine and Drug Development 2(5): 239-241.
-
Hashimoto DA, Rosman G, Rus D, Meireles OR (2018) Artificial intelligence in surgery: promises and perils. Annals of surgery 268(1): 70-76.
-
Hamet P, Tremblay J (2017) Artificial intelligence in medicine. Metabolism 69: S36-S40.
-
Ahmad Z, Rahim S, Zubair M, Ghafar J (2021) Artificial intelligence (AI) in medicine, current applications and future role with special emphasis on its potential and promise in pathology: present and future impact, obstacles including costs and acceptance among pathologists, practical and philosophical considerations. A comprehensive review. Diagnostic pathology 16: 1-6.
-
Bohr A, Memarzadeh K (2020) The rise of artificial intelligence in healthcare applications. In Artificial Intelligence in healthcare. Academic Press pp: 25-60.
-
Gumbs AA, Frigerio I, Spolverato G, Croner R, Illanes A, et al. (2021) Artificial intelligence surgery: How do we get to autonomous actions in surgery. Sensors 21(16): 5526.
-
Koteluk O, Wartecki A, Mazurek S, Kolodziejczak I, Mackiewicz A (2021) How do machines learn? Artificial intelligence as a new era in medicine. Journal of Personalized Medicine 11(1): 32.
-
Becker A (2019) Artificial intelligence in medicine: What is it doing for us today. Health Policy and Technology 8(2): 198-205.
-
Mesko B, Gorog M (2020) A short guide for medical professionals in the era of artificial intelligence. NPJ digital medicine 3(1): 126.
-
Bajwa J, Munir U, Nori A, Williams B (2021) Artificial intelligence in healthcare: transforming the practice of medicine. Future healthcare journal 8(2): e188.
-
Busnatu S, Niculescu AG, Bolocan A, Petrescu GE, Paduraru DN, et al. (2022) Clinical applications of artificial intelligence: An updated overview. Journal of clinical medicine 11(8): 2265.
-
Pesapane F, Codari M, Sardanelli F (2018) Artificial intelligence in medical imaging: threat or opportunity? Radiologists again at the forefront of innovation in medicine. European radiology experimental 2(1): 35.
-
Alsuliman T, Humaidan D, Sliman L (2020) Machine learning and artificial intelligence in the service of medicine: Necessity or potentiality. Current research in translational medicine 68(4): 245-251.
-
Kulkarni S, Seneviratne N, Baig MS, Khan AH (2020) Artificial intelligence in medicine: where are we now. Academic radiology 27(1): 62-70.
-
Hashimoto DA, Ward TM, Meireles OR (2020) The role of artificial intelligence in surgery. Advances in Surgery 54: 89-101.
-
Panesar SS, Kliot M, Parrish R, Miranda J, Cagle Y, et al. (2020) Promises and perils of artificial intelligence in neurosurgery. Neurosurgery 87(1): 33-44.
-
Liu PR, Lu L, Zhang JY, Huo TT, Liu SX, et al. (2021) Application of artificial intelligence in medicine: an overview. Current Medical Science (6): 1105-1115.
-
Liu R, Rong Y, Peng Z (2020) A review of medical artificial intelligence. Global Health Journal 4(2): 42-45.
-
Haleem A, Javaid M, Khan IH (2019) Current status and applications of Artificial Intelligence (AI) in medical field: An overview. Current Medicine Research and Practice 9(6): 231-237.
-
Malik P, Pathania M, Rathaur VK (2019) Overview of artificial intelligence in medicine. Journal of family medicine and primary care 8(7): 2328.
-
Agah A (2013) Medical applications of artificial intelligence. CRC Press.
-
Jiang L, Wu Z, Xu X, Zhan Y, Jin X, et al. (2021) Opportunities and challenges of artificial intelligence in the medical field: current application, emerging problems, and problem-solving strategies. Journal of International Medical Research 49(3): 03000605211000157.
-
Mintz Y, Brodie R (2019) Introduction to artificial intelligence in medicine. Minimally Invasive Therapy & Allied Technologies 28(2): 73-81.
-
Xing L, Giger ML, Min JK (2020) Artificial intelligence in medicine: technical basis and clinical applications. Academic Press.
-
Zhou XY, Guo Y, Shen M, Yang GZ (2020) Application of artificial intelligence in surgery. Frontiers of medicine14: 417-430.
-
Davenport T, Kalakota R (2019) The potential for artificial intelligence in healthcare. Future healthcare journal 6(2): 94.
-
Safdar NM, Banja JD, Meltzer CC (2020) Ethical considerations in artificial intelligence. European journal of radiology 122: 108768.
-
Hamamoto R, Suvarna K, Yamada M, Kobayashi K, Shinkai N, et al. (2020) Application of artificial intelligence technology in oncology: Towards the establishment of precision medicine. Cancers. 12(12): 3532.
-
Wong SH, Hasani H, Alam Z, Alam A (2019) Artificial intelligence in radiology: how will we be affected. European radiology 29: 141-143.
-
Hartskamp M, Consoli S, Verhaegh W, Petkovic M, Stolpe A (2019) Artificial intelligence in clinical health care applications. Interactive journal of medical research 8(2): e12100.
-
Matheny M, Israni ST, Ahmed M, Whicher D (2019) Artificial intelligence in health care: The hope, the hype, the promise, the peril. National Academy of Medicine pp: 1-15.
-
Haug CJ, Drazen JM (2023) Artificial intelligence and machine learning in clinical medicine, 2023. New England Journal of Medicine 388(13): 1201-1208.
-
Dzobo K, Adotey S, Thomford NE, Dzobo W (2020) Integrating artificial and human intelligence: a partnership for responsible innovation in biomedical engineering and medicine. Omics: a journal of integrative biology 24(5): 247-263.
-
Stefanelli M (2001) The socio-organizational age of artificial intelligence in medicine. Artificial intelligence in medicine 23(1): 25-47.
-
Yu KH, Beam AL, Kohane IS (2018) Artificial intelligence in healthcare. Nature biomedical engineering 2(10): 719-731.
-
Ramesh AN, Kambhampati C, Monson JR, Drew PJ (2004) Artificial intelligence in medicine. Annals of the Royal College of Surgeons of England 86(5): 334.
-
Peek N, Combi C, Marin R, Bellazzi R (2015) Thirty years of artificial intelligence in medicine (AIME) conferences: A review of research themes. Artificial intelligence in medicine 65(1): 61-73.
-
Shortliffe EH (1993) The adolescence of AI in medicine: will the field come of age in the’90s. Artificial intelligence in medicine 5(2): 93-106.
-
Holzinger A, Langs G, Denk H, Zatloukal K, Muller H (2019) Causability and explainability of artificial intelligence in medicine. Wiley Interdisciplinary Reviews: Data Mining and Knowledge Discovery 9(4): e1312.
-
Kaul V, Enslin S, Gross SA (2020) History of artificial intelligence in medicine. Gastrointestinal endoscopy 92(4): 807-812.
-
Szolovits P (2019) Artificial intelligence in medicine. Routledge.
-
Schwartz WB, Patil RS, Szolovits P (1987) Artificial intelligence in medicine. New England Journal of Medicine 316(11): 685-688.
-
Holmes J, Sacchi L, Bellazzi R (2004) Artificial intelligence in medicine. Ann R Coll Surg Engl 86: 334-338.
-
Scerri M, Grech V (2020) Artificial intelligence in medicine. Early human development 145: 105017.
-
Buch VH, Ahmed I, Maruthappu M (2018) Artificial intelligence in medicine: current trends and future possibilities. British Journal of General Practice 68(668): 143-144.
- Revolutionizing Property Measurement Through Artificial Intelligence: The Journey of PropertyMeasure.ai
- AI Infused Business Model Innovation for Competitive Advantage in the Era of Big Data and Digital Transformation
- Use of CPM/PERT in the Effort to Eradicate Polio
- Integrated Multimodal Deep Learning Framework for Early Detection of Mouth Cancer Using CT Imaging and Clinical Symptom Analysis
- Artificial Intelligence in Medical Robotics and Assistance: An Overview
- Server Migration with Multipath-QUIC