Artificial Intelligence versus Healthcare and Medical System: An Editorial
Artificial intelligence (AI) research within medicine is growing rapidly. Healthcare AI projects attracted more investment than AI projects within any other sector of the global economy. Nevertheless, among the excitement, there is equal scepticism, with some urging caution at inflated expectations. Since the turn of the century, AI has also been successfully progressive into the fields of medicine and health care. The core of evidence-based medicine is using historical data to inform clinical decision making. This task has traditionally been tackled by statistical methods, which describe patterns in data as mathematical equations. For instance, neural networks use a large number of interconnected neurons to represent data in a manner akin to that of the human brain. These include the availability of robust and reasonably priced computing (processing) tools, hardware (such as graphics processing units), software, and applications- even in consumer-grade personal computers and mobile devices- and large (big) data sets with a wide variety of information types and formats, both in online and cloud platforms and produced in real time by wearable technology and the internet of things (IoT); the growth of open source coding resources and online communities of practitioners and users exchanging resources, know-how, and experience; and the integration of computer processing with other technologies like photonics (the fusion of applied optics and electronics) and human-machine interfaces.
Editorial
Artificial intelligence (AI) research within medicine is growing rapidly. Healthcare AI projects attracted more investment than AI projects within any other sector of the global economy. Nevertheless, among the excitement, there is equal scepticism, with some urging caution at inflated expectations [1, 2]. Since the turn of the century, AI has also been successfully progressive into the fields of medicine and health care [3, 4]. The core of evidence-based medicine is using historical data to inform clinical decision making. This task has traditionally been tackled by statistical methods, which describe patterns in data as mathematical equations [5]. For instance, neural networks use a large number of interconnected neurons to represent data in a manner akin to that of the human brain. These include the availability of robust and reasonably priced computing (processing) tools, hardware (such as graphics processing units), software, and applications- even in consumer-grade personal computers and mobile devices- and large (big) data sets with a wide variety of information types and formats, both in online and cloud platforms and produced in real time by wearable technology and the internet of things (IoT) [6]; the growth of open source coding resources and online communities of practitioners and users exchanging resources, know-how, and experience; and the integration of computer processing with other technologies like photonics (the fusion of applied optics and electronics) and human-machine interfaces [5, 6].
Certain AI systems have advanced from testing to deployment in recent years, gaining administrative backing and overcoming regulatory obstacles. By permitting funding for the use of two particular AI systems for medical picture diagnosis [7] at the Centers for Medicare and Medicaid Services, which authorizes public insurance reimbursement expenses, has promoted the application of AI in clinical settings. In addition, a 2020 study discovered that the US Food and Drug Administration (FDA) are rapidly approving AI products, especially those that use machine learning (ML), a subset of AI [8]. These developments mostly come in the form of FDA clearances, which set a lower regulatory threshold for goods than full-fledged approvals but nonetheless pave the way for the application of AI/ML systems in actual clinical settings. It is important to point out that the datasets used for these regulatory clearances are often made up of retrospective, single-institution data that are mostly unpublished and considered proprietary. To build trust in medical AI systems, stronger standards for reporting transparency and validation will be required, including demonstrations of impact on clinical outcomes [7, 8].
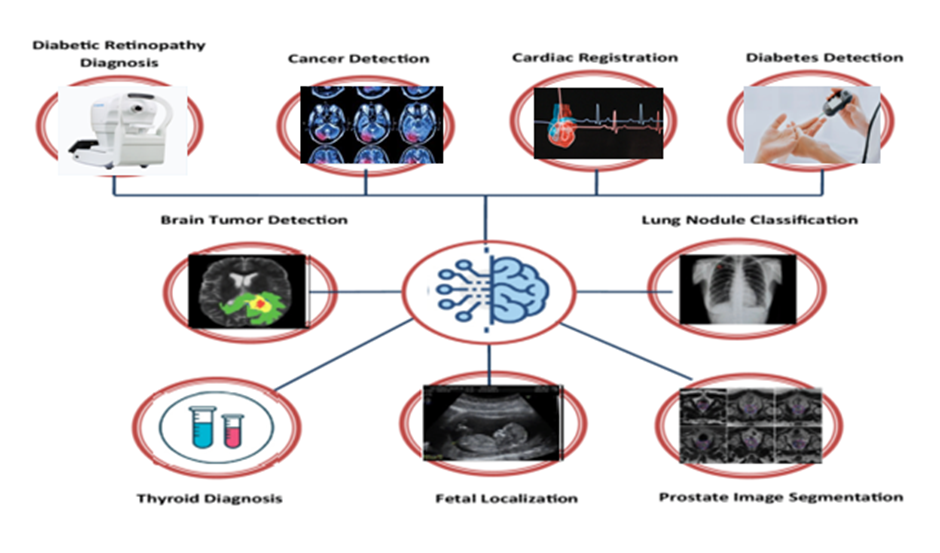
Recent years have seen a notable advancement in image categorization thanks to deep learning that uses neural networks to directly identify patterns in raw data. Medical AI research has so flourished in fields like radiology, pathology, gastrointestinal, and ophthalmology that mostly rely on image interpretation [9, 10]. In the field of ophthalmology, deep learning models have been used extensively, leading to significant advancements in deployment (Figure 1). Studies have examined the human impact of such models on health systems in addition to measuring model performance.
Apart from utilizing new data sources, current research has experimented with non-traditional issue formulations. Traditionally, models like as neural networks are used to learn functions mapping from inputs to labels, and datasets are created using actual data to generate inputs and labels. However, datasets with accurate inputs and labels are typically hard to come by and are commonly reused across numerous researches due to the time-consuming and costly nature of labeling. To address issues where data are unlabeled or otherwise noisy, additional paradigms have been employed, such as unsupervised learning (more especially, self-supervised learning), semi-supervised learning, causal inference, and reinforcement learning. By improving current technology and expanding our knowledge of diseases, these developments have pushed the limits of medical AI. Instead of being restricted to preexisting labels, as in the supervised paradigm [11] unsupervised learning-learning from data without any labels has yielded useful discoveries by enabling models to discover new patterns and categories.
For instance, clustering algorithms, which group similar unlabeled data points together to organize them, have been used to identify clinically significant patient subgroups for illnesses like endometriosis, breast cancer, and sepsis [11]. These classifications may eventually aid in the diagnosis, prognosis, and therapy of diseases by exposing new patterns in their appearance [11].
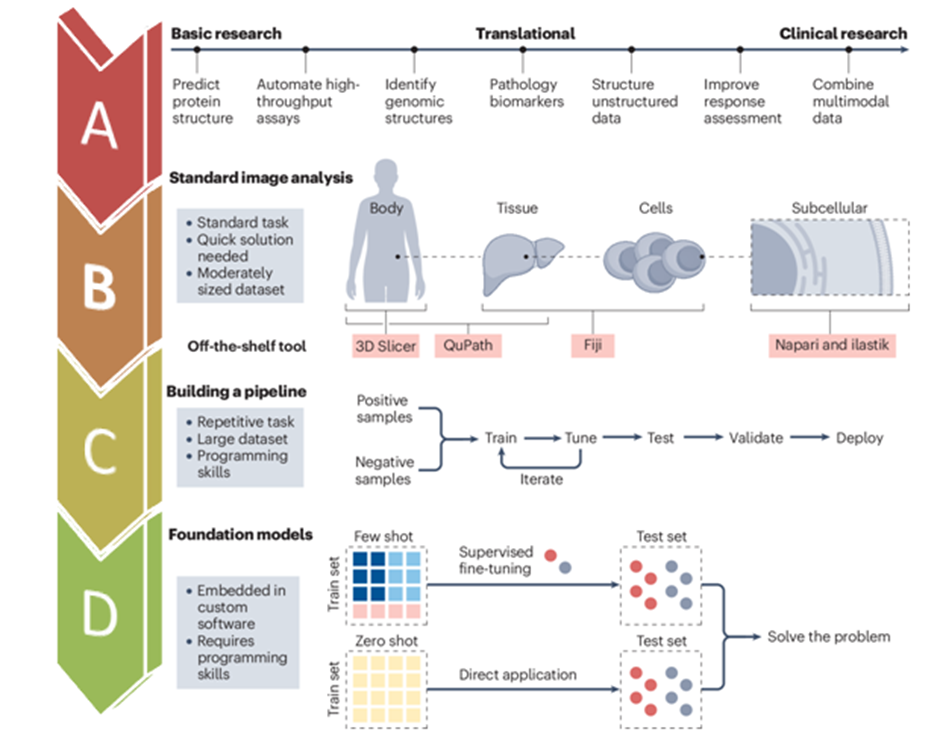
Medical AI research frequently follows a well-known pattern: it starts with an image classification problem, trains an AI system using supervised learning on labeled data, and then assesses the system by comparing it to human experts (Figure 2).
Despite the notable advancements made in these studies, we provide three more exciting research directions that deviate from the norm we start by talking about non-image data sources that can offer valuable medical insights, like text, chemical, and genetic sequences. Secondly, we go over problem formulations that go beyond supervised learning, using paradigms like unsupervised or semi-supervised learning to extract insights from unlabeled or otherwise defective data (Figure 2). In order to improve performance, we lastly examine AI technologies that work alongside people rather than against them than either AI or humans alone [12, 13].

Recent developments in biochemistry have been made possible by AI, leading to a better knowledge of the composition and behavior of biomolecules 33-36. Senior et al.’s work on AlphaFold marked a breakthrough in the crucial process of protein folding that entails predicting a protein’s three-dimensional structure based on its chemical sequence. Protein structure prediction advances can offer mechanistic understanding of a variety of phenomena, including drug- protein interactions and the consequences of mutations [14]. Additionally, Alley and colleagues made significant progress in the field of protein analysis by developing statistical summaries that capture important protein characteristics and support learning by neural networks using fewer data 34. Instead of utilizing raw chemicals, such summaries sequences, models for jobs that come after, such as molecular function may use a lot less labeled data and yet achieve good performance. Despite the challenges, AI has also advanced the area of genetics. Modeling 3D genomic connections is difficult. When utilized circulating cell-free DNA data, AI has made non-invasive cancer identification, prognosis, and tumour origin 37-39. By predicting guide-RNA activity and identifying anti-CRISPR protein families, deep learning has improved CRISPR-based gene editing efforts. Furthermore, the rapid identification of antibiotic resistance in pathogens has been achieved by AI-based analysis of microbial transcriptomic and genomic data. Physicians may now quickly choose the best courses of action, which could lower mortality and avoid the needless use of broad-spectrum antibiotics [14]. Moreover, AI is already starting to speed up the drug discovery process. It has been demonstrated that deep learning models for molecular analysis speed up the process of finding new medications by eliminating the need for slower, more expensive physical experiments. Predicting pertinent physical characteristics like the toxicity or bioactivity of possible medications has been made easier with the help of such models. The application of AI in certain medical fields and healthcare has been updated as follows:
• AI in Psychiatry: Clinical information about mental health is more individualized and quality. However, there are still many benefits for mental health from artificial intelligence [15]. Algorithms for machine learning have effectively separated patients in good health from those in with psychotic disorders with greater than 70% accuracy, as well as run pre-diagnostic tests and create risk models. to assess a person’s potential for developing psychological disorder [15]. EEG-based deep learning techniques are capable to determine depressed persons with greater accuracy than 90%. Psychotherapy tools such as Tess and others chatbots that use an interactive display to function. The one that Patients might use Woebot to recognize their feelings, lessen anxiousness, as well as lessen symptoms of depression. The Avatar treatment effectively raises medication compliance in schizophrenia, particularly those who are not responding to therapy schizophrenia and helps with depressed symptoms, hallucinations, and symptoms as well as general life satisfaction. Children with autism spectrum condition have shown improvements in spontaneous language during therapy sessions, and socially robotic assistance was created to help them develop social skills. Compared to human therapists, children appear to perform better with their robot companions [15]. Patients with dementia, the elderly, and those suffering from depression can benefit from companion bots, which also aid to improve mood and social relationships while lowering stress, anxiety, and loneliness [15]. As compared to spoken presentations, text-based psycho- educational interactions result in reduced substance use and increased program adherence.
• AI in Cancer Research: Machine learning was aided by the genomes, proteomics, histology, and radiology pictures found in cancer data pools such as Genome Atlas. On utilizing H and E-stained tissue to distinguish between cancer and healthy cells with good prediction accuracy, a comparable pictures of skin lesions taken using a camera and a microscope Dermatologists did not perform as well as the model [16] (Figure 3). In forecasting gastric occult peritoneal metastases DNNs have a better AUC (0.92-0.94) for cancers as contrast to employing pathological and clinical qualities. Prostate cancer based on MRI differentiation revealed a cancer risk AUC of 0.84.27. Mammography results indicate a high degree of accuracy in instances verified by biopsy [16]. Studies revealed a rise in Mammograms’ perfect specificity and sensitivity for detection of cancer in contrast to a typical radiograph. Zhou et al. developed a deep learning technique to predict the grade from liver cancer patients’ MRI scans, and they reported an AUC of 0.83. Non-neural network-based methods have been used to predict drug characteristics and toxicity. AI has been used to stage lung nodules from computed tomography (CT) images [17], identify COVID-19 from chest X-rays, and classify thyroid tissue using ultrasound imaging. Convolutional neural networks have demonstrated high accuracy and precision of 93% and 67%, respectively, when utilized for the automated detection of liver cancers on CT scans [18, 19] (Figure 3).
AI in Cardiology
Although quantitative data collection for AF is a laborious, time-consuming, and error-prone procedure, cardiac magnetic resonance is a recent breakthrough [20]. DL approaches are very useful for image processing, segmentation, and reconstruction. Its increased accuracy and decreased processing time [20]. Electrocardiogram Signal information resembling that of wearable smart devices is utilized in order to obtain a 0.91 area under the ROC to determine It performed better than cardiologists in these rhythms. [20, 21, 22]. The one that Apple research assessed an irregular pulse’s capacity to alerting system to detect atrial fibrillation, as well as a total of approximate 35% of cases were clinically confirmed with a positive predictive value. Predicting the long-term efficacy of rhythm control strategies is a critical step in the clinical decision-making process for patients with AF. In the AADGEN study, the potential of different ML algorithms to monitor the initiation of Dofetilide was demonstrated and predicted dosing decisions with 96% accuracy. Radio-frequency ablation can be evaluated using computational simulation AF with an average sensitivity and specificity of 84% and 90%, respectively, and an AUC of 0.82 to predict the recurrence risk of AF [20, 21, 22, 23].
AI in Surgery
Every autonomous activity in surgery is based on every facet of artificial intelligence. Chang et al. have compiled collective data on AI applications in various spinal operations [24]. AI is being used more often as a result of the advancements in surgical automation. From partial functions like picture guidance to operations where no direct human involvement is needed, the surgeries have the potential to eventually become fully AI-based and autonomous [24]. One of the most well-known robotically assisted surgical systems is the Da Vinci Surgical System. Using a remote booth with technology to control the robot’s arms, the surgical system enables the surgeons to perform surgery [25]. The majority of doctors typically accept this minimally invasive technique because of its accuracy. Artificial intelligence (AI)-driven internet or mobile platforms can be used to remotely perform surgery, even in spaceships or in areas affected by natural catastrophes or conflict [26]. AI is undoubtedly moving in the right direction, even though it doesn’t appear to be directly involved in surgery because of certain aspects of human anatomy and the requirement for spontaneous decision-making [24, 25, 26, 27].
AI in Intestinal Diseases
With an accuracy of almost 95%, ANNs trained on VCE pictures can detect small intestinal ulcerations and nonobstructive stenosis [28]. A method for AI-ulcer detection was created by Barash et al using more than 16,000 images from over 3000 UC patients, the [28]. MES model demonstrated exceptional AuROC, sensitivity, and specificity of 0.970, 0.83, and 0.96 [29]. Syed and colleagues conducted a new study in which they found that a convolutional neural network could analyse sets of duodenal samples and distinguish between celiac disease and both normal tissue and environmental enteropathy [30]. In a study employing 23 MREs in young CD patients, neural network segmentation of the lumen, bowel wall, and backdrop matched manually segmented bowel images in 75%, 81%, and 97% of the cases, respectively Stidham RW, et al. [30] with 0.754 vs.
0.590 accuracy. Humans are more likely to perceive images incorrectly due to a variety of factors, including exposure, education, experience, weariness, distractions, a vast amount of visual data, and the image’s physical quality [28, 29, 30, 31].
Nonetheless, AI and human intellect are predicted to coexist in the field of medicine in the future. Thence, healthcare practitioners must be regularly taught to use, enhance, and improve AI in view of evolving the healthcare system. This should be confirmed by adequate study in the area. AI is threatening the jobs of healthcare professionals. As per survey of about eighty percent of 791 psychiatrists AI would not be able to provide compassionate care, and 3.8% said it would render their professions obsolete [32, 33, 34, 35, 36]. Similar to pathologists, who were open to AI and only 17.6% worried about their future job security, 89% of radiologists did not fear losing their jobs. According to neurosurgeons, AI is being used to forecast results [34]. AI can reduce the burden of work for health professionals, so physicians can focus on the interpersonal relationship with patients. In recent years researches published on topics connecting AI and medical fields are in increasing exponentially.
AI can enable healthcare systems to achieve their ‘quadruple aim’ by democratizing and standardizing a future of connected and AI augmented care, precision diagnostics, precision therapeutics and, ultimately, precision medicine [32, 33, 34, 35, 36]. Research on the use of AI in healthcare is still progressing quickly, and potential applications are being shown in a variety of healthcare domain (physical and mental health), encompassing medication administration, disease diagnosis, prognosis, drug discovery, virtual clinical consultation, and health monitoring. In the short, medium, and long terms, authors outline a limited set of AI applications in healthcare for the potential capabilities of AI to augment, automate and transform medicine. Artificial intelligence cannot reason in the same manner as human doctors, who can rely on “clinical intuition and experience” or “common sense.” This is because AI systems are not yet reasoning engines [32, 33, 34, 35, 36]. AI instead acts as a signal translator, interpreting patterns found in datasets. AI technologies are currently being used by healthcare organizations to automate repetitive, time-consuming procedures with a high volume. The application of AI to precision diagnostics (such as diabetic retinopathy and radiation planning) has also advanced significantly [36].
Conclusion and Future Perspectives
Research in medical artificial intelligence frequently follows a corresponding pattern: it begins with an image classification problem, trains an AI system using supervised learning on labeled data, and then compares the system to human specialists for assessment. Despite the noteworthy advancements made in these studies, authors provide three more thrilling research directions that pervert from the criterion. Initially, there is a discussion on non-image data sources that can output worthy medical insights, including text, chemical, and genetic sequences. Secondly, using paradigms like unsupervised or semi-supervised learning, the problem is explored for developing formulations that go beyond supervised learning and extract insights from unlabeled or otherwise defective data. In order to get higher performance, author lastly examines AI technologies are precisely examined, likely to work alongside people rather than against them. Unconventional issue formulations have been tried in recent studies in addition to new data sources. In a traditional dataset, inputs and labels are extracted from actual data, and functions mapping inputs to labels are learned by models such as neural networks. Other paradigms have been employed to address issues where data are unlabeled or otherwise noisy, such as unsupervised learning (more especially, self-supervised learning), semi-supervised learning, causal inference, and reinforcement learning. These developments have improved current technology and expanded the understanding of disease, thus pro-pulsing the limits of medical AI. Despite impressive advancements, there are still significant technical obstacles in the field of medical AI, especially when it comes to creating training datasets and gaining user trust in AI systems. The speedy progression of AI technology presents an opportunity for its application in clinical practice, potentially revolutionizing healthcare services, though there are still concerns over the regulation of AI in medicine as well as how it might change and add roles across the healthcare system, equally impacting patients, medical practioners and researchers.
References
-
Mishra S, Tiwari AM (2024) Current trends of artificial intelligence in biotechnology: An editorial. Open Access Journal of Data Science & Artificial Intelligence 2(1): 000112.
-
Ahmad M, Gupta P, Singh B, Tiwari AM, Mishra S (2023) Biotechnology is a boon to mankind: Scenario in India. Asian J Curr Res 8(2): 1-8.
-
Buch VH, Ahmed I, Maruthappu M (2018) Artificial intelligence in medicine: current trends and future possibilities. British J General Prac 68: 143-144.
-
Milea D, Najjar RP, Jiang Z, Ting D, Vasseneix C, et al. (2020) Artificial intelligence to detect papilledema from ocular fundus photographs. N Engl J Med 382: 1687- 1695.
-
Porumb M, Stranges S, Pescape A, Pecchia L (2020) Precision medicine and artificial intelligence: a pilot study on deep learning for hypoglycemic events detection based on ECG. Sci Rep 10: 170.
-
Attia ZI, Noseworthy P, Jimenez F, Asirvatham S, Deshmukh A, et al. (2019) An artificial intelligence- enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: a retrospective analysis of outcome prediction. Lancet 394: 861-867.
-
Bhinder B, Gilvary C, Madhukar NS, Elemento O (2021) Artificial intelligence in cancer research and precision medicine. Cancer Discov 11(4): 900-915.
-
Ting DSW, Cheung C, Lim G, Tan G, Quang ND, et al. (2017) Development and validation of a deep learning system for diabetic retinopathy and related eye diseases using retinal images from multiethnic populations with diabetes. JAMA 318(22): 2211-2223.
-
Gulshan V, Peng L, Coram M, Stumpe M, Wu D, et al. (2016) Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 316(22): 2402-2410.
-
Hosny A, Parmar C, Quackenbush J, Schwartz LH, Aerts HJWL (2018) Artificial intelligence in radiology. Nat Rev Cancer 18(8): 500-510.
-
Olczak J, Fahlberg N, Maki A, Razavian AS, Jilert A, et al. (2017) Artificial intelligence for analyzing orthopedic trauma radiographs. Acta Orthop 88(6): 581-586.
-
Niazi MKK, Parwani AV, Gurcan MN (2019) Digital pathology and artificial intelligence. Lancet Oncol 20(5): e253-261.
-
Abbasgholizadeh RS, Legare F, Sharma G, Archambault P, Zomahoun HTV, et al. (2021) Application of artificial intelligence in community based primary health care: Systematic scoping review and critical appraisal. J Med Internet Res 23(9): e29839.
-
Luxton DD (2014) Recommendations for the ethical use and design of artificial intelligent care providers. Artif Intell. Med 62(1): 1-10.
-
Shatte A, Hutchinson DM, Teague SJ (2019) Machine learning in mental health: a scoping review of methods and applications. Psychol Med 49(9): 1426-1448.
-
Ding L, Bailey MH, Pardo E, Thorsson V, Colaprico A, et al. (2018) Perspective on oncogenic processes at the end of the beginning of cancer genomics. Cell 173: 305-320.
-
Coudray N, Ocampo PS, Sakellaropoulos T, Narula N, Snuderl M, et al. (2018) Classification and mutation prediction from non-small cell lung cancer histopathology images using deep learning. Nat Mef 24: 1559-1567.
-
Esteva A, Kuprel B, Novoa RA, Ko J, Swetter SM, et al. (2017) Dermatologist-level classification of skin cancer with deep neural networks. Nature 542: 115-118.
-
Jiang Y, Liang X, Wang W, Chen C, Yuan Q, et al. (2021) Noninvasive prediction of occult peritoneal metastasis in gastric cancer using deep learning. JAMA Netw Open 4: e2032269.
-
Jamart K, Xiong Z, Talou GD, Stiles MK, Zhao J (2020) Mini review: deep learning for atrial segmentation from late gadolinium-enhanced MRIs. Front Cardiovasc Med 7: 86.
-
Bai W, Sinclair M, Tarroni G, Oktay O, Rajchl M, et al. (2018) Automated cardiovascular magnetic resonance image analysis with fully convolutional networks. J Cardiovasc Magn Reson 20: 65-71.
-
Hannun AY, Rajpurkar P, Haghpanahi M, Tison GH, Bourn C, et al. (2019) Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat Med 25: 65-69.
-
Deo RC (2015) Machine learning in medicine. Circulation 132: 1920-1930.
-
Chang M, Canseco JA, Nicholson KJ, Patel N, Vaccaro AR (2020) The role of machine learning in spine surgery: The future is now. Front Surg 7: 54.
-
Panesar S, Cagle Y, Chander D, Morey J, Miranda J, et al. (2019) Artificial intelligence and the future of surgical robotics. Ann Surg 270: 223-226.
-
Rasouli JJ, Shao J, Neifert S, Gibbs WN, Habboub G, et al. (2021) Artificial intelligence and robotics in spine surgery. Glob Spine J 11: 556-564.
-
Panesar SS, Ashkan K (2018) Surgery in space. Br J Surg 5:1234-1243.
-
Klang E, Barash Y, Margalit RY, Soffer S, Shimon O, et al. (2020) Deep learning algorithms for automated detection of Crohn’s disease ulcers by video capsule endoscopy. Gastrointest Endosc 91: 606-613.
-
Barash Y, Azaria L, Soffer S, Yehuda R, Shlomi O, et al. (2021) Ulcer severity grading in video capsule images of patients with Crohn’s disease: An ordinal neural network solution. Gastrointest Endosc 93: 187-192.
-
Stidham RW, Liu W, Bishu S, Michael DR, Peter DRH, et al. (2019) Performance of a deep learning model vs. human reviewers in grading endoscopic disease severity of patients with ulcerative colitis. JAMA Netw Open 2(5): e193963.
-
Syed S, Lubaina E, Aman S, Saurav S, Marium K, et al. (2021) Artificial intelligence- based analytics for diagnosis of small bowel enteropathies and black box feature detection. J Pediatr Gastroenterol Nutr 72(6): 833-841.
-
Quinn TP, Senadeera M, Jacobs S, Coghlan S, Le V (2021) Trust and medical AI: the challenges we face and the expertise needed to overcome them. J Am Med Inform Assoc 28: 890-894.
-
Wang C, Scott SM, Subramanian K, Loguercio S, Zhao P, et al. (2019) Quantitating the epigenetic transformation contributing to cholesterol homeostasis using Gaussian process. Nat Commun 10: 5052.
-
Amodio M, Dijk D, Srinivasan K, Chen W, Mohsen H, et al. (2019) Exploring single-cell data with deep multitasking neural networks. Nat Methods 16: 1139-1145.
-
Urteaga I, McKillop M, Elhadad N (2020) Learning endometriosis phenotypes from patient- generated data. NPJ Digit Med 3: 88.
-
Courtiol P, Maussion C, Moarii M, Pronier E, Pilcer S, et al. (2019) Deep learning-based classification of mesothelioma improves prediction of patient outcome. Nat Med 25: 1519-1525.
- Revolutionizing Property Measurement Through Artificial Intelligence: The Journey of PropertyMeasure.ai
- AI Infused Business Model Innovation for Competitive Advantage in the Era of Big Data and Digital Transformation
- Use of CPM/PERT in the Effort to Eradicate Polio
- Integrated Multimodal Deep Learning Framework for Early Detection of Mouth Cancer Using CT Imaging and Clinical Symptom Analysis
- Artificial Intelligence in Medical Robotics and Assistance: An Overview
- Server Migration with Multipath-QUIC