Correlation between Bilateral Muscle Loading Asymmetry and Neck Pain - A Prospective Cross-Sectional Study
Background: Neck discomfort is a common musculoskeletal disorder which often manifests into scapular asymmetry, muscle imbalances, and restricted joint mobility. This study attempts to establish the correlation between asymmetries of the posterior chain muscles and individuals with neck pain. Method: 85 subjects, 36 male and 49 female, were required for this study. A biomechanical postural evaluation using a Postural bench and Neck Disability Index (NDI) score was taken for further analysis in this study. Result: The relationship between the NDI, scapular asymmetry and pelvis asymmetry was highly significant. A significant relationship was seen between lumbar asymmetry and NDI whereas no relationship was found between NDI and total body asymmetry. Conclusion: It is concluded that the neck disability was significantly related to scapular and pelvis load asymmetry, however, the total body asymmetry was not significantly related.
Introduction
One of the most prevalent musculoskeletal conditions in the modern world is neck pain [1]. Awkward postures, worry, tension, hard lifting, physically demanding jobs, and gadget addiction are a few prominent reasons for neck pain [2]. The external auditory meatus, shoulder joint, hip joint’s centre, and knee and ankle joints are all passed through by an ideal posture when viewed from the sagittal perspective. Any alteration in this alignment results in bad postures as well as pain, weakness, and tension in the muscles.
A properly aligned spine and shoulder girdle allow the scapula to move freely and symmetrically. Poor posture causes the muscles in the upper back and posterior shoulder to weaken and stretch, while the muscles in the chest and anterior shoulder become stiff and hyperactive. The scapula inhibits motion and causes the shoulder blades to deviate, which further limits the range of motion in the shoulder joint. The muscles and ligaments surrounding the shoulder blades are continuously strained as a result of this. Eventually, asymmetry and abnormalities in the scapula manifest [3].
An unequal development or disparity in strength between the muscles on the dorsal side of the body, particularly the muscles in your legs, hips, and spine, is known as a posterior chain muscle asymmetry. Postural stability, function, and overall movement all depend on the posterior chain [4]. Asymmetry of spinal segments and lower back discomfort; asymmetry of hip muscles and unequal weight distribution; asymmetry of the lower limbs and unpredictable gait; and neck pain and scapular asymmetry are among the conditions for which numerous studies have looked at the effects and consequences of muscle imbalances [5, 6].
Inappropriate neck position causes the muscles involved to become loaded, worn out, and structurally weak [7]. Conditions include text neck syndrome, round shoulder, forward head posture, upper arm syndrome, and others produce scapular asymmetry, decrease mobility, and cause neck discomfort as well as muscle imbalances and additional stress on the cervical spine. Incorrect posture, poor stability of the implicated muscles, and functional restriction are all caused by muscular imbalances in the scapular area [8]. This impairment also has an impact on socioeconomic position by raising health care costs, increasing sick leave, and lowering job and personal care productivity.
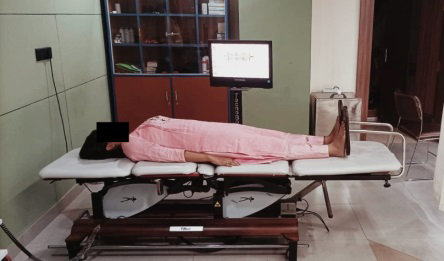
Neck discomfort is a multifactorial disease and in addition to today’s lifestyle, it is emerging as a chronic problem. Identifying the risk factors can guide to prevent neck discomfort or disability. Hence, the Techno-bed otherwise called as Postural bench MF system of Techno-body Italy, a machine analysis used to assess the postural biomechanics, was used in this study to check the muscle tension generated both in supine lying position i.e. 180 degrees and with a body angle at 120 degrees.
One of the primary indicators of musculoskeletal impairment is an imbalance or uneven distribution of muscle mass and strength between the two sides of the body or between various muscle groups. Functional imbalances brought on by impaired muscle asymmetry impact posture, movement, and general physical performance. As the body may overuse certain muscles or change movement patterns to make up for the imbalance, it might raise the risk of injury. Muscular asymmetries can make discomfort or functional restrictions worse for individuals with a musculoskeletal handicap than they would be for individuals without asymmetries. Studies have shown that people with neck- related problems frequently have scapular and upper back muscular imbalances [9, 10].
Despite the above mentioned facts, there is no objective data to quantify the degree and volume of the relationship between muscular asymmetries and neck disability; therefore, this study attempts to establish the correlation between asymmetries of the posterior chain muscles and neck pain.
Methods and Materials
This observational study was conducted amongst 85 university students after approval of the institutional ethical committee approval and a written consent was obtained from all the participants prior to the commencement. As there was no risk involved on the study procedures the institutional ethical approval was obtained. The study was conducted according to the declaration of Helenski. In this study, participants of both gender who had non-specific neck discomfort over the previous three months and were between the ages of 18 and 25 years were included. Those who had segmental incorrect postures, such as forward head position, cervical lordosis, thoracic kyphosis, and hyperextension of the head were excluded from the study.
Before beginning the study, every individual was thoroughly evaluated and appraised. To carry out this study, 85 willing participants were chosen after taking the inclusion and exclusion criteria into account. In addition to gathering demographic information, a Neck Disability Index (NDI) score chart was given to the participants for self-evaluation. After submitting their NDI scores charts, participants were instructed to lie down on the postural bench’s sensor bed so that researchers could measure the amount of tension that their muscles were creating at 180 and 120 degrees of body angle, respectively. Each subject’s demographic information, NDI score, and Postural Benchmark score were gathered for further data analysis.
Postural Bench
Postural bench MF system of Technobody Italy (Figure 1) is used to assess the biomechanical posture and muscle imbalances generated in each segment and on each side of the body. The postural bench is equipped with a sensor bed, foot rest, a remote and a monitor. The sensor bed has a pivot in the middle and four flat, tilting surfaces: the scapula, thorax, pelvis, and tibial section. The subject must position themselves on the sensor bed with the anterior superior iliac spine (ASIS) in the middle and their foot parallel to the foot rest. The subject must remain on the bed in the supine posture for 30 seconds before the monitor reveals the reading regarding the muscle tension in each segment and on either side of the body. Readings are taken in two different angles where the body is in 180 degrees (Figure 1) and in 120 degrees (Figure 2) pivoted at the center of the postural bench.

Neck Disability Index
Neck disability index is a reliable and comprehensively validated self-assessment 10 items questionnaire that assesses the disability associated with neck pain in relation to subjective symptomatology and activities of daily living. The questions are based on pain, intensity, headache, concentration, sleep, lifting, work, driving, recreation, personal care and reading. Each question scores from 0 indicating no disability to 5 indicating maximum disability. At the end of the questionnaire, the subject scores between 0 indicating no disability to 50 indicating total disability. A score less than 4 indicates no disability, 5-14 mild disability, 15-24 moderate disability, 25-34 severe disability and score greater than 35 complete disability.
Data Analysis
SPSS version 26 was used for statistical analysis. The non-parametric Spearman correlation coefficient was used to investigate the relationship between NDI, and asymmetrical difference in whole body, scapula, lumbar and pelvic segment as the data did not follow normal distribution. A low value of p = 0.05 rejects the null hypothesis.
Results
A total of 85 subjects, 36 male and 49 female of mean age 22 +/- 0.64 years, weight 53.4 (10.5) Kgs, height 155.23 +/- 8.6 centimeters and BMI 23.76 +/-7.19 were recruited for this study. The demographical characteristics of these subjects are shown in Table 1. The mean NDI score was 15.51+/-2.42 and the mean difference for the total body was 6.83 +/-3.77, scapular asymmetry 5.53 +/-2.4, lumbar asymmetry 3.54 +/- 3.13, pelvic asymmetry 3.95 +/-2.97.
| DEMOGRAPHICAL DATA | |
|---|---|
| Subjects (n) | 85 |
| Age (years) | 22 (2.64) |
| Gender (male/female) | 36/49 |
| Height (cm) | 155.23 (8.6) |
| Weight (kg) | 53.4 (10.5) |
| BMI (kg/m2) | 23.76 (7.19) |
| Total body asymmetry (kg) | 6.83 (3.77) |
| Scapular asymmetry (kg) | 5.53 (2.4) |
| Lumbar asymmetry (kg) | 3.54 (3.13) |
| Pelvic asymmetry (kg) | 3.95 (2.97) |
| NDI | 15.51 (2.42) |
Table 1: Demographic Data Expressed in Mean (Standard Deviation).
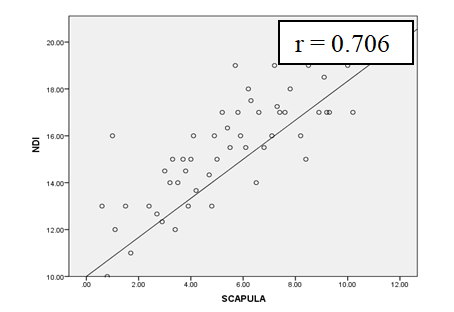
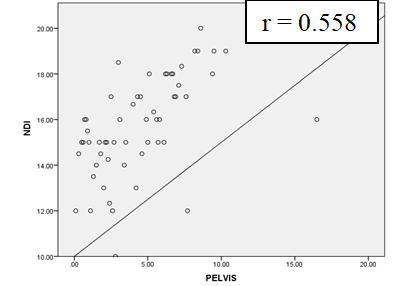
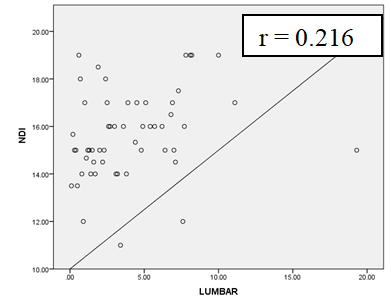
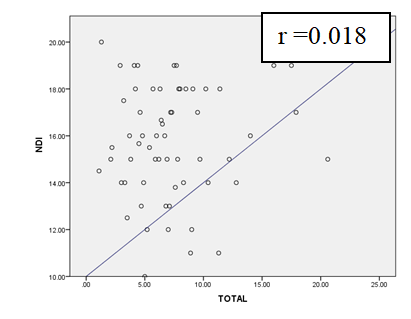
The result of the current study revealed that the neck disability is highly correlated with scapular (Figure 3, r = 0.706) and pelvis (Figure 4, r = 0.558) asymmetry and there was a low correlation between with lumbar asymmetry (Figure 5, r = 0.216). However, the total body asymmetry did not correlate significantly (Figure 6, r =0.018) as shown in Table 2.
The relationship between the NDI, scapular asymmetry and pelvis asymmetry was highly significant. A significant relationship was seen between lumbar asymmetry and NDI whereas no relationship was found between NDI and total body asymmetry.
| Variables | Spearman (r) | P- value | |
|---|---|---|---|
| NDI | Total body asymmetry | 0.018 | 0.86 |
| NDI | Scapular asymmetry | 0.706** | 0 |
| NDI | Lumbar asymmetry | 0.216* | 0.04 |
| NDI | Pelvic asymmetry | 0.558** | 0 |
Table 2: Relationship between the Variables and NDI - Neck Disability Index. ** Highly Significant
Discussion
To perform movements of the shoulder, the muscles attached to the scapula must be balanced and work synchronizing with the thoracic segment. Any change in the balance can alter the stabilization, cause pain in the neck and shoulder and further lead to scapular asymmetry and incorrect posture [11]. Muscles that are attached to the segment bilaterally should be well-balanced and symmetrical to undertake any typical activities or movements. Scapular symmetry is crucial for greater stability and balanced movement, especially during neck- specific movements. Additional spinal or pelvic asymmetries, together with scapular asymmetries, however may have an impact on stability and movement patterns. To the best of the author’s knowledge, this is the first investigation into the relationship between neck dysfunction and the muscle asymmetries of various body regions using a postural bed. The majority of research has used EMG devices to compare healthy and symptomatic persons on one side alone when examining the association between muscle function and musculoskeletal pain and impairment. The current study, however, employed a postural bed technology to measure the muscle asymmetry on both sides of various segments. This study aimed to evaluate the muscle imbalances in the scapular region of subjects having neck pain for the last 3 months. To understand the depth of neck pain, the Neck Disability Index, a self-evaluating questionnaire was used. A lateral scapular slide test, which measures the distance between the scapula and the thorax, was used in a few investigations that validated the association between scapular asymmetry and visual analogue scale [12]. The study also found a correlation of r=0.632 between the visual analogue scale and the neck disability score, showing that neck pain can induce moderate functional impairment in the neck [13]. Furthermore, weak muscles are thought to make it difficult to maintain balance and appropriate posture while performing daily duties, which raises the risk of pain and body asymmetry [6].
One study that looked at the relationship between neck pain disability and the degree of forward head position revealed that muscle imbalance is strongly connected with neck pain disability and that it is also a risk factor for neck pain, which lends credence to the current finding [14]. Similar to this, a study on the upper cross syndrome found a correlation between postural asymmetry and imbalance or asymmetry in the scapular stabilizer muscles [3]. Evidence shows that neck impairment is highly connected with postural muscle imbalance. According to one study that looked at muscle asymmetries and neck discomfort, people with neck pain showed more muscular asymmetries than healthy controls [15].
Comparing people with neck pain to healthy controls, few investigations have focused on the relative difference in scapular and shoulder muscle activation. Patients with neck pain experienced considerably less change in axio- scapular muscle strength than patients in the control group [16]. Similar to this, it has also been noted that people who only had one side of their neck pain had much poorer trapezius strength on that side compared to the other side [17]. Additionally, it is believed that weak muscles increase the risk of pain and body asymmetry by making it difficult to maintain balance and proper posture while doing daily tasks [15].
It has been suggested that altered axio-scapular muscle function may contribute to neck pain due to abnormal loading of the cervical spine or through an altered length- tension relationship because muscle impairment is a known feature of painful neck disorders, and the scapula shares common muscle attachments with the neck. When the hip joint lacks flexibility, compensatory movements occur in the lumbar-pelvic region, and micro damage to the lumbar vertebrae induces lower back discomfort [18, 19].
According to previous research in other body segments Studies show a significant relationship between left and right pelvic misalignment and back discomfort [20]. Similarly, symmetrical imbalances in the bilateral scapular region might contribute to neck impairment in the shoulder region.
The present study was performed on 85 subjects having non-specific neck discomfort for the last 3 months. After thoroughly assessing the postural bench score and NDI score, statistical analysis was done. A significant relationship was found between NDI and the difference in muscle imbalances in the scapular, lumbar and pelvic regions whereas no significant relationship was found between total body asymmetry and NDI score.
As per the body biomechanics, neck asymmetries may eventually result in pelvis asymmetries. The alignment of the entire spine can be impacted by an imbalance or asymmetry in scapular muscles. To preserve balance, the alignment of the spine below the neck will be adjusted to make up for asymmetry in the neck. The thoracic and lumbar segments of the spine will be affected by the changes in scapular musculature. As the body works to maintain stability and function over time, these modifications may cause pelvic asymmetry. Therefore, an analysis of the symmetrical muscular difference on the thorax, pelvis and tibial segment was further continued.
Due to the anatomical relationship, the forward head posture is intimately tied to the upper body posture and is easily influenced by trunk posture as well. According to studies, extended sitting is also linked to forward head posture [21, 22]. There is additional proof that pelvic asymmetry affects the cervical spine’s range of motion, and it has been seen that following pelvic rectification, the cervical spine’s range of motion significantly improved [22]. It is therefore feasible to speculate that the posterior spinal muscles, through the thoracolumbar fascia, connect the lower trunk to the neck. Certain studies have shown a strong correlation between the cervical and pelvic spine’s posture and the alignment of the complete spine [6, 20, 23].
On assessing the ergonomics and daily routine of all subjects, it was found that incorrect postures during activities, prolonged use of smart gadgets, lack of exercise and prolonged sitting with cervical flexion were the most common reasons for muscle weakness. However, this study was limited to 85 subjects aged between 18 to 25 years. As the study was cross-sectional, cause and effect could not be determined.
This study was also restricted to understanding the depth of neck discomfort due to muscular imbalances in the scapular region. Further multi-centric studies can be done with larger sample sizes and different age groups by including other body segments. This study emphasised on muscular asymmetry at the scapular region, further studies can be done on other body segments, to evaluate the imbalance between asymptomatic and symptomatic people as well as between different age groups. Second, a subgroup analysis of occupation and muscle asymmetry is required.
Conclusion
Results show that neck discomfort and muscular asymmetry in the scapular or thorax region are interdependent. It further leads to lumbar and pelvis asymmetry if unnoticed or incorrect postures are adapted. The study highlighted the difference in muscular load asymmetry on both sides in individuals with neck pain. It is concluded that the neck disability was significantly related to scapular and pelvis load asymmetry, however, the total body asymmetry was not significantly related.
Declarations
Ethics Approval and Consent to Participate
Ethical clearance was taken from the ethical committee of the institute and consent was taken from the participants. The study is not a clinical trial, so no clinical trial registration was done. The participants were aware of all procedures involved in the study and a written consent was taken for the same. Consent for Publication The informed written consent form was signed by all the participants before participation in the study and agreed to the publication of the data reports.
Competing Interests
The authors declare that they have no competing interests.
Funding
There was no external funding obtained for this study
Availability of Data And Materials
The data collected and/or analysed during the study are available with the corresponding author.
References
-
Kazeminasab S, Nejadghaderi SA, Amiri P, Pourfathi H, Araj-Khodaei M, et al. (2022) Neck pain: global epidemiology, trends and risk factors. BMC musculoskeletal disorders 23(1): 26.
-
Kim R, Wiest C, Clark K, Cook C, Horn M (2018) Identifying risk factors for first-episode neck pain: A systematic review. Musculoskeletal Science and Practice 33: 77-83.
-
Nitayarak H, Charntaraviroj P (2021) Effects of scapular stabilization exercises on posture and muscle imbalances in women with upper crossed syndrome: Randomized Controlled Trial 34(6): 1031-1040.
-
Vora M, Ranawat d, Arora M, Tiwari A (2018) Analysis of posterior chain muscle symmetry in junior badminton players of South Asia. J Phy Fit Treatment & Sports 6(1): 1-7.
-
O’leary S, Falla D, Elliott JM, Jull G (2009) Muscle dysfunction in cervical spine pain: implications for assessment and management. J Orthop Sports Phys Ther 39(5): 324-333.
-
Kim WD, Shin D (2023) Effects of Pelvic-Tilt Imbalance on Disability, Muscle Performance, and Range of Motion in Office Workers with Non-Specific Low-Back Pain. In Healthcare (Basel) 11(6): 893.
-
Yip CH, Chiu TT, Poon AT (2008) The relationship between head posture and severity and disability of patients with neck pain. Manual therapy 13(2): 148-154.
-
Castelein B, Cools A, Bostyn E, Delemarre J, Lemahieu T, et al. (2015) Analysis of scapular muscle EMG activity in patients with idiopathic neck pain: a systematic review. J Electromyogr Kinesiol 25(2): 371-386.
-
Mahmoud NF, Hassan KA, Abdelmajeed SF, Moustafa IM, Silva AG (2019) The relationship between forward head posture and neck pain: a systematic review and meta- analysis. Current reviews in musculoskeletal medicine 12(4): 562-577.
-
Dong Y, Wang XM, Wang MQ, Widmalm SE (2008) Asymmetric muscle function in patients with developmental mandibular asymmetry. J Oral Rehabil 35(1): 27-36.
-
Ebaugh DD, McClure PW, Karduna AR (2005) Three- dimensional scapulothoracic motion during active and passive arm elevation. Clinical Biomechanics 20(7): 700- 709.
-
Kim SR, Kang MH, Bahng SY, An JK, Lee JY, et al. (2016) Correlation among scapular asymmetry, neck pain, and neck disability index (NDI) in young women with slight neck pain. J Phys Ther Sci 28(5): 1508-1510.
-
Vernon H (1996) The neck disability index: patient assessment and outcome monitoring in whiplash. Journal of Musculoskeletal Pain 4(4): 95-104.
-
Na JG, Lee HS, Park SW (2018) Effects of exercise type on neck disability, pain, and postural changes in subjects with forward head posture: systematic review and meta- analysis. Korean Society of Physical Medicine 13(3): 121-132.
-
Multanen J, Häkkinen A, Kautiainen H, Ylinen J (2021) Associations of neck muscle strength and cervical spine mobility with future neck pain and disability: a prospective 16-year study. BMC Musculoskeletal Disorders 22(1): 911.
-
Chaurasia P, Mhase S, Panda M, Khan S, Bedre V, et al. (2022) Impact of Scapular Repositioning Using a Scapular Belt for Axioscapular Muscle Imbalance in Patients With a Non-specific Neck Pain: A Case Report. Cureus 14(8): e28126.
-
Petersen SM, Wyatt SN (2011) Lower trapezius muscle strength in individuals with unilateral neck pain. journal of orthopaedic & sports physical therapy 41(4): 260- 265.
-
Arab AM, Soleimanifar M, Nourbakhsh MR (2019) Relationship between hip extensor strength and back extensor length in patients with low back pain: a cross- sectional study. Journal of manipulative and physiological therapeutics 42(2): 125-131.
-
Wand BM, O’Connell NE (2008) Chronic non-specific low back pain–sub-groups or a single mechanism? BMC musculoskeletal disorders 9: 11.
-
Yoo WG, Kim MH (2016) The relationship between pelvic asymmetry and low back pain: A systematic review. Phys Ther Korea 23: 1-9.
-
Le Huec JC, Thompson W, Mohsinaly Y, Barrey C, Faundez A (2019) Sagittal balance of the spine. European spine journal 28(9): 1889-1905.
-
Scheer JK, Lau D, Ames CP (2021) Sagittal balance of the cervical spine. Journal of Orthopaedic Surgery 29(1): 23094990211024454.
-
Brandl A, Wilke J, Egner C, Reer R, Schmidt T, et al. Thoracolumbar fascia deformation during deadlifting and trunk extension in individuals with and without back pain. Frontiers in Medicine 10: 1177146.
- An Evaluation of Distraction Control in Experienced Cyclists During a 20 Minute Time-Trial Performance
- Do Games Missed Predict Rankings in the NBA A Machine Learning Approach
- Elite Taekwondo Athletes: The Relationship among Sport Psychology, Mental Health, and the National Sport Organization
- Immediate Effect of Continuous Running on Red Blood Cells (RBC), Packed Cell Volume (PCV) and Red Blood Cell Distribution Width (RDW) Among Physically Trained Boys
- Echocardiographic Insights into Left Ventricular Functional Adaptation in Track and Field Athletes: A Comprehensive Review
- Could there be a Relationship between early Specialization and Load Management Practices in Professional Athletes