Evaluation of Vaccine Hesitancy and the Influence of Side Effects on Vaccination Drive amidst Covid-19 Pandemic in India
The COVID-19 pandemic is the most severe public health challenge the world has encountered. Although necessary precautions laid by the government are being followed to control the spread of the disease, vaccination is the only long-term answer to such a global issue. The COVID-19 vaccines have been rapidly developed and approved for emergency use. However, many people were hesitant to vaccinate against COVID-19 which reduced the success rate of vaccination programs. Through this research, we aim to study the reasons contributing to vaccine hesitancy and their probability of occurrence amongst the Indian population. A survey focusing on vaccine hesitancy and side effects of the COVID-19 vaccine was conducted and the data obtained were analyzed to understand the reasons behind vaccine hesitancy and the impact of side effects on the vaccination drive. The hesitation of people towards getting vaccinated revolves around a variety of aspects including, brand name, lack of confidence in vaccines and vaccination drive, conspiracy theories, educational and socio-economic status, underlying health issues, etc. Of notice, concern about side effects, and possible long-term side effects were the most important determinants. The severity of the short-term effects was found to be very low, implying that vaccination is completely safe and that people should get vaccinated against this virus as soon as possible and should not worry about side effects that are milder and shortlived. However, the real scenario of long-term side effects cannot be determined for now.
Introduction
Coronaviruses (CoV) are a broad family of viruses that can cause a variety of illnesses, from the common cold to more serious illnesses. A novel coronavirus (nCoV) is a new strain of coronavirus that has never been seen in humans before. The novel virus was given the moniker “COVID-19 virus” [1, 2]. The SARS-CoV-2 virus causes Coronavirus Disease (COVID-19), an infectious disease. The virus spreads in microscopic liquid particles from the mouth or nose when an infected person speaks, sneezes, coughs or even breathes. The particle size varies from larger respiratory droplets to smaller aerosols. The virus causes mild to moderate respiratory disease in the majority of infected people [3, 4]. Severe sickness is more likely to strike the elderly [5] and those with underlying medical disorders such as cardiovascular disease [5, 6], diabetes [7], obesity [7], chronic respiratory disease [5, 8], or cancer [9]. The ongoing COVID-19 pandemic has instilled the fear of uncertainty in all aspects of life, including one’s health. Many people turned to vaccination as a medium of safeguarding themselves against the life- threatening effects of the virus while others are hesitant to adopt vaccination as a shield protecting from the disease to certain limits. People’s unwillingness to acquire safe and recommended accessible vaccines has been recorded way before the COVID-19 pandemic, known as ‘vaccine hesitancy. It was already an increasing concern. Understanding whether people are willing to be vaccinated, the reasons for their willingness or unwillingness, and the most trusted sources of information contributing to their decision-making will be necessary for increasing vaccine uptake (especially against COVID-19). The reasons for accepting and refusing the COVID-19 vaccine remain complex. As new variants of the virus emerge, adding further complexity, along with new vaccines entering the market, a fine balance must be maintained between communicating what is known and acknowledging the remaining uncertainties.
India has approved nine vaccines, three of which have been developed in India. All these have different mechanisms but the same goal- immunization against the coronavirus. Vaccines available in India are; Covisheld- a recombinant vaccine developed by Serum Institute of India (Oxford/ AstraZeneca formulation), Covaxin- an inactivated vaccine developed by Bharat Biotech, Pfizer- an mRNA vaccine manufactured by Pfizer Inc., and Sputnik-V- a viral vectored vaccine developed by Gamaleya Research Institute of Epidemiology and Microbiology in Russia. Apart from these vaccines other vaccines like Moderna, Janssen (Johnson & Johnson), Corbevax, and ZyCoV-D vaccine are also available for the Indian population. Data show that Covishield was most administered in India, followed by Covaxin, Sputnik-V, and Pfizer [10].
It is tough to persuade people in developing countries like India to get vaccinated where media and publications play a major role in such matters. In a diverse country with a population of 138 crores, the huge population is rather hard to manage. Under the universal immunization program, the government of India tried to provide both doses of vaccine throughout the country at affordable rates. Despite all the efforts made for the vaccination program, a significant amount of people were hesitant to get vaccinated. This study attempted to identify and analyze the reasons behind the development of hesitation towards vaccination and their probability of occurrence amongst the population under survey. People of different ages, gender, educational backgrounds, and socioeconomic statuses were surveyed for a wide variety of reasons ranging from fear of needles to conspiracy theories to fear of side effects that could be bothering them and contributing to their vaccine hesitancy.
Materials and Methods
Study Design, Population, and Sampling
First, an electronic questionnaire (google forms) was generated and circulated (between July 2021 and October 2021) to conduct a study on the reasons for COVID-19 vaccine hesitancy in India. The questions were meant for people who come under the vaccine-eligible age (18 and above). Between October 2021 and February 2022, another survey-based study was conducted to collect data on the COVID-19 vaccines’ side effects among people in various parts of India. Consent was obtained for both surveys before answering questions and the anonymity of their identities has remained throughout.
Questionnaires
Questionnaire Based on Vaccine Hesitancy: The initial questions were aimed at categorizing people based on their age, gender, educational background, state they belong to, and employment status. In the next section, we asked if they were vaccinated or not. Non-vaccinated people were asked for their reasons for not getting vaccinated yet, and if they have any hesitancy about getting vaccinated. The last section of the questionnaire had questions specifically related to the reasons for vaccine hesitancy amongst people. All the data collected was analyzed.
Questionnaire Based on Side Effects: In this questionnaire first, we asked people to fill in their details like gender, age, etc which helped us to study the relationship between the side effects versus gender and age. Second, if they were vaccinated, third, the name of the vaccine they received, and finally the participants who experienced side effects were asked about the kind of side effects they experienced, the duration and the severity of the side effects and whether they had to visit the doctor. They were also asked if they experienced any long-term side effects. They were also asked if they experienced any long-term side effects. Participants with underlying medical conditions were asked if vaccination had worsened their underlying medical conditions.Lastly, they were asked if they got infected by COVID-19 after getting vaccinated. All the data collected was analyzed.
Results
Sample Characteristics
For Vaccine hesitancy: All respondents agreed to be a part of the study. More than 50% of them (57.3%) belonged to the age group 18-25. Around 26.2% were in the age group 26-45 and 16.5% were 46 and above.
Approximately, 68.9% of the respondents were female, while 31.1% were male. No third-gender responses were obtained. A vast majority of them (53.3%) were students, 20.3% were involved in the government sector, 14% were in the private sector, 6.5% were self-employed and 5.9% were unemployed.
For side effects: All respondents agreed to be a part of the study. Approximately 68.6% of the respondents were female, while 31.4% were male. No third-gender responses were obtained. More than 50% of them (60.6%) belonged to the age group 18-25. Around 14.7% were in the age group 26-40 and 21.4% were 40 and above. Out of all respondents, 81.6% of people had taken both doses of the vaccine, 11.7% had taken just the first dose and 6.7% were still not vaccinated. Amongst vaccinated people, 78.7% were recipients of Covisheld followed by 19.3% Covaxin recipients. Very few were vaccinated with Sputnik V and Pfizer Vaccine.
Reasons for Vaccine Hesitancy
Despite 99.6% of individuals being aware of the importance of administering the vaccine, 14.7% of individuals were hesitant about getting vaccinated. Keeping the total number of hesitant participants at 100%, 65.9% hesitant were females and 34.1% were males. When considering age groups, 46.5% of people fell into the age group of 18-25, 36.5% people fell in the age group of 26-45, and 17% people aged 46 and above. Based on our survey, it was observed that there was usually more than one reason responsible for inducing hesitancy in people. The reasons vary from simple misinformation about the vaccine to genuine fear of side effects.
Fear of Side Effects: When observing the reasons for vaccine reluctance in people, it was found that approximately 91.4% of vaccine-hesitant persons were hesitant due to fear of side effects (Figure 1).
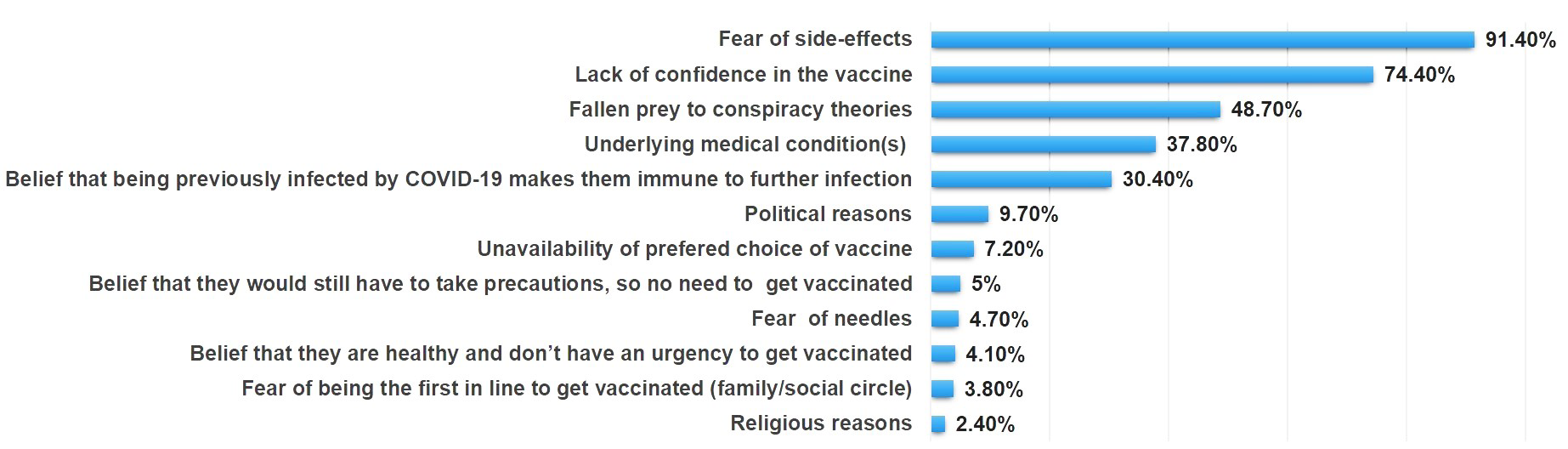
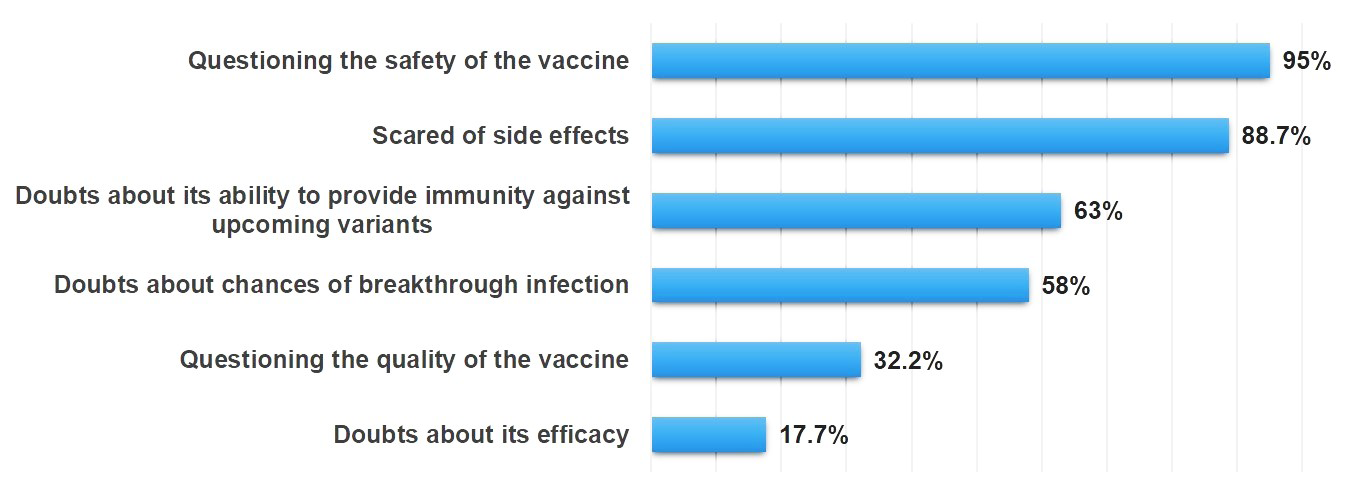
Lack of Confidence and Vaccine Hesitancy: Lack of confidence in the COVID-19 vaccine was the second major reason for hesitancy among people as 74.4% of hesitant people lack confidence in the vaccine (Figure 1). 95% of them were questioning the safety of the vaccine with regards to its short manufacturing period and whether or not it underwent proper clinical trials, i.e., accelerated R&D process. 88.7% of the people were scared of the side effects. Almost 63% of the people had doubts about its ability to provide immunity against upcoming variants and 58% were hesitant about the chances of breakthrough infection. 32.2% of people were questioning the quality of the vaccine, and factors like the manufacturing conditions, storage conditions, and transport conditions. 17.7% had doubts about its working and efficiency(Figure 2).
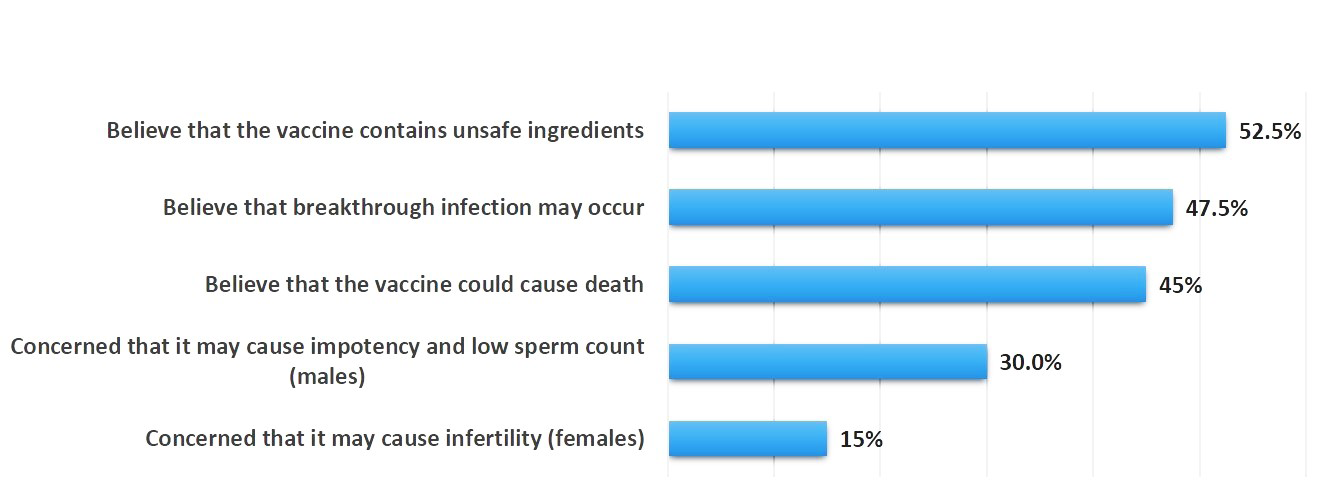
Conspiracy Theories and Vaccine Hesitancy: 48.7% of the participants in our study have fallen prey to conspiracy theories [most concerned for more than one reason] (Figure 1). Around 52.5% of this population believes that the vaccine contains unsafe ingredients that may cause side effects in the long run or adversely affect health conditions. 47.5% believe in breakthrough infection. 45% believe that the vaccine could even cause death. Around 30% of males believed that it may cause impotency and result in low sperm count, while 15% of the females believed that it may cause infertility in them (Figure 3).
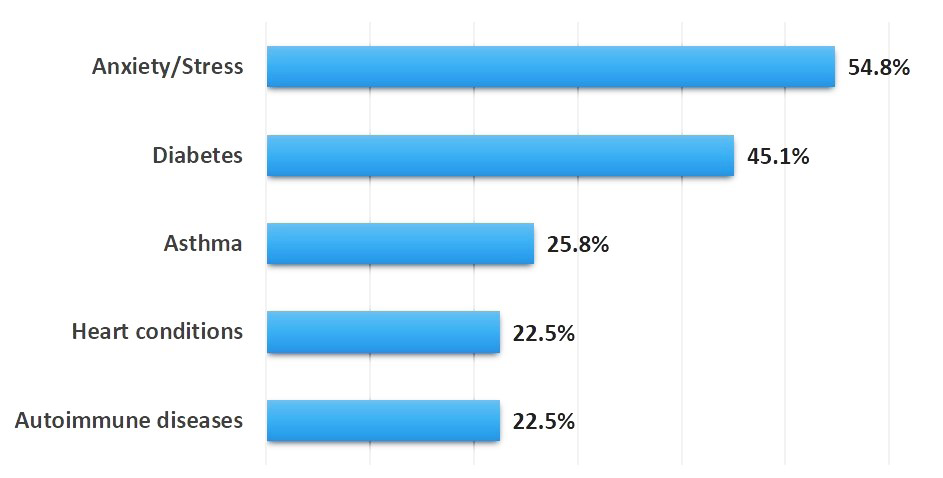
Underlying Medical Conditions and Vaccine Hesitancy: Around 37.8% were hesitant due to their underlying medical conditions [most concerned due to more than one reason] (Figure 1). 54.8% were reluctant due to anxiety/stress,
45.1% due to diabetes, 25.8% due to asthma, 22.5% due to heart conditions, and another 22.5% due to autoimmune disease (Figure 4). Pregnancy, allergies, and recent surgeries were also some concerns.
Other Concerns: Approximately, 30.4% of unvaccinated individuals believed that being previously infected by COVID-19 makes them resistant to the infection and therefore there is no need for them to take the vaccine. 7.2% of people were hesitant because of the unavailability of their preferred choice of the vaccine in their locality. Around 5% of people believed that there is no need to get vaccinated if all the precautions (wearing a mask, social distancing, and regular sanitization) still have to be taken. 4.7% of individuals had a fear of needles. 4% of people believed that being healthy does not require getting vaccinated. Around 3.8% of people were hesitant due to the fear of being the first one in the line to be vaccinated in their family or social circle. Some of the individuals were also hesitant owing to political (9.7%) and religious issues (2.4%) (Figure 1).
Side Effects Reported After COVID-19 Vaccination Drive
Since, in our study, the major cited reasons for COVID-19 vaccine hesitancy were due to fear of side effects (91.4%) (Figure 1), we aimed to know how rational this fear is. So, we focused on side effects and their severity encountered by people post-vaccination. Short-term Side Effects: It was observed that 91% of the participants were afraid of side effects, as revealed by the vaccine hesitation study (Figure 1), more than half (52%) of them experienced side effects; 36.9% after the first dose,
4.3% after the second dose, and 10.8% after both doses. The remaining 48% did not show any side effects.
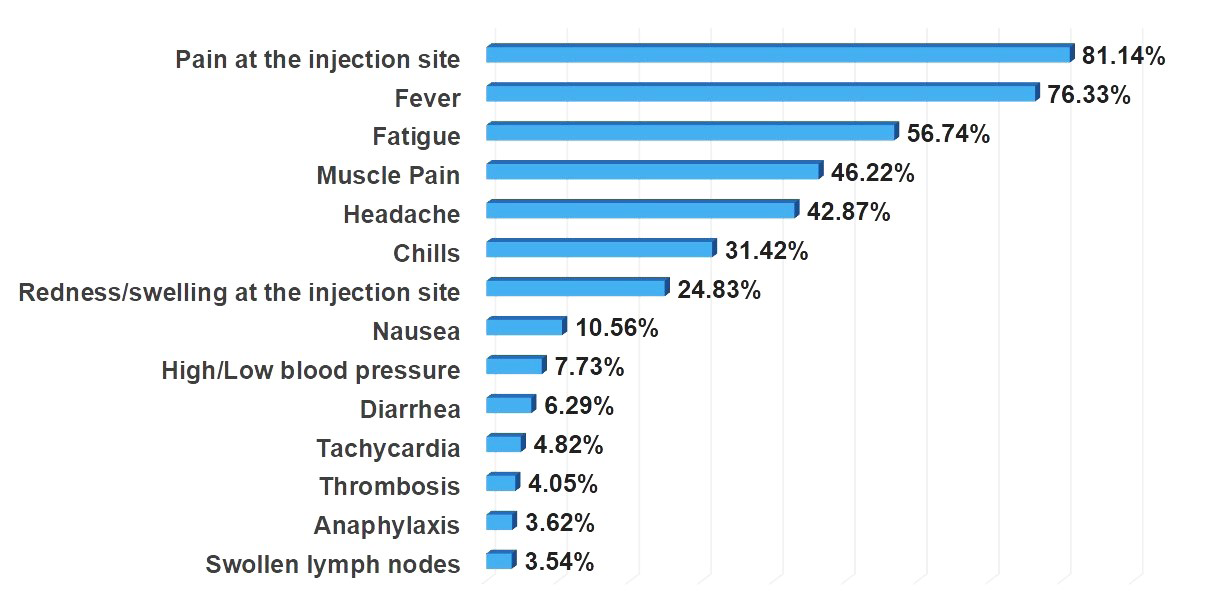
The most observed side effects were pain at the injection site (81.14%), fever (76.33%), fatigue (56.74%), muscle pain (46.22%), headache (42.87%), chills (31.42%), redness/ swelling at the injection site (24.83%), and nausea (10.56%) as depicted in Figure 5. Lesser observed side effects were high/low blood pressure (7.73%), diarrhea (6.29%), tachycardia (4.82%), thrombosis (4.05%), anaphylaxis (3.62%), and swollen lymph nodes (3.54%) (Figure 5).
| Age Group | 18-25 (65.75%) | 26-45 (14.02%) | 45 and above (20.23%) | |||
|---|---|---|---|---|---|---|
| Gender | Males (18.93%) | Females (81.07%) | Males (33.34%) | Females (66.66%) | Males (26.92%) | Females (73.08%) |
| Pain at the injection site | 84.37% | 91.24% | 58.33% | 83.00% | 85.71% | 84.21% |
| Fever | 78.12% | 83.21% | 75.00% | 79.16% | 71.43% | 71.05% |
| Fatigue | 59.37% | 57.66% | 66.66% | 50.00% | 35.71% | 71.05% |
| Muscle Pain | 53.12% | 46.71% | 50.00% | 41.00% | 28.57% | 57.89% |
| Headache | 53.12% | 49.63% | 66.66% | 25.00% | 28.57% | 34.21% |
| Chills | 40.62% | 27.00% | 40.00% | 8.33% | 35.71% | 36.84% |
| Redness/swelling at the injection site | 34.37% | 36.49% | 16.66% | 20.83% | 14.29% | 26.32% |
| Nausea | 21.87% | 22.62% | 8.33% | 0% | 0% | 10.53% |
| High/Low blood pressure | 9.37% | 9.48% | 0% | 12.50% | 7.14% | 7.89% |
| Diarrhea | 9.37% | 9.48% | 0% | 8.33% | 0% | 10.53% |
| Tachycardia | 12.5% | 5.10% | 0% | 4.16% | 7.14% | 0% |
| Thrombosis | 12.5% | 6.56% | 0% | 0% | 0% | 5.26% |
| Anaphylaxis | 12.5% | 6.56% | 0% | 0% | 0% | 2.63% |
| Swollen lymph nodes | 9.37% | 5.10% | 0% | 4.16% | 0% | 2.63% |
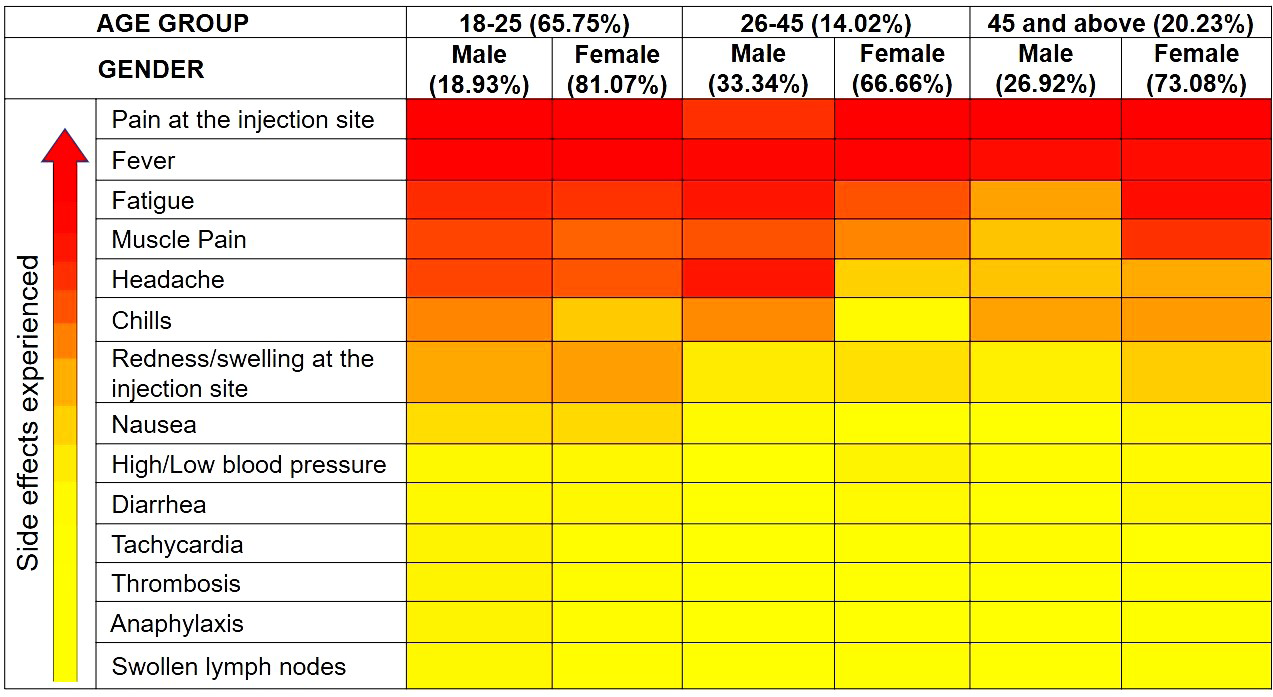
Table 1: Comparative analysis of side effects with age and gender. Yellow shading (where females complained more in number), gree
Of notice, females experienced more side effects than males as depicted in Table 1. When considering age groups, age groups 18–25 experienced more side effects (65.75%) compared with other age groups as shown in Table 1.
To find out whether any side effects were more prevalent in any age group or gender, it was found that more women aged 18-25 and 26-45 experienced pain at the injection site compared to men in the same age group. For those over the age of 45, an equal number of men and women experienced pain at the injection site. Muscle pain, headache, and chills were more noticed in the males in the age group 18-25 and 26-45 than the females of the same age group. However, for those above 45 years of age, more females complained about muscle pain and headache, while, a similar number of cases were reported in both males and females experiencing chills. Fatigue and nausea were observed in a similar percentage of males and females of ages 18-25 and 26-45, while in the age group 45 and above more females reported fatigue and nausea than males. Redness/swelling at the injection site and diarrhea was reported in a similar number of males and females in the age group 18-25, but more females from age group 26-45 and above 45 reported these side effects. Fluctuations in blood pressure were equally reported in both males and females of the age group 18-25 and the age group 45 and above. For the age group 26-45, females were found to experience fluctuations in blood pressure. Of notice, no males reported fluctuations in blood pressure in our survey. Thrombosis and anaphylaxis were found to be more common in males in the age group 18-25, while more females in the age group 45 and above complained about these side effects. Of notice, no data was found for age groups 26-45 in our survey. Swollen lymph nodes were noticed more in males in the age group 18-25, while in other age groups, more females complained about the side effect. Males in the age group 18- 45 and 45 and above reported more cases of tachycardia. A heat map of the same is shown in Figure 6.
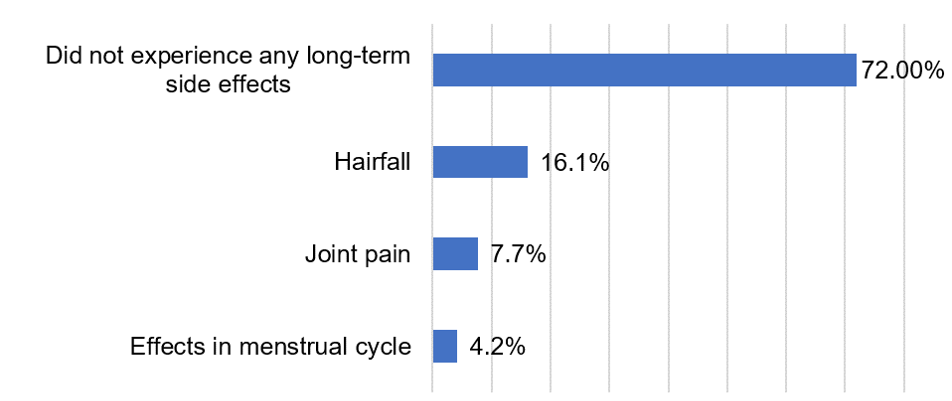
Long-term Side Effects: Although the maximum number of participants (72%) did not report any long-term side effects, some individuals did experience long-term side effects like hair fall (16.1 %), joint pain (7.7%), and effects in the menstrual cycle (4.2 %) (Figure 7).
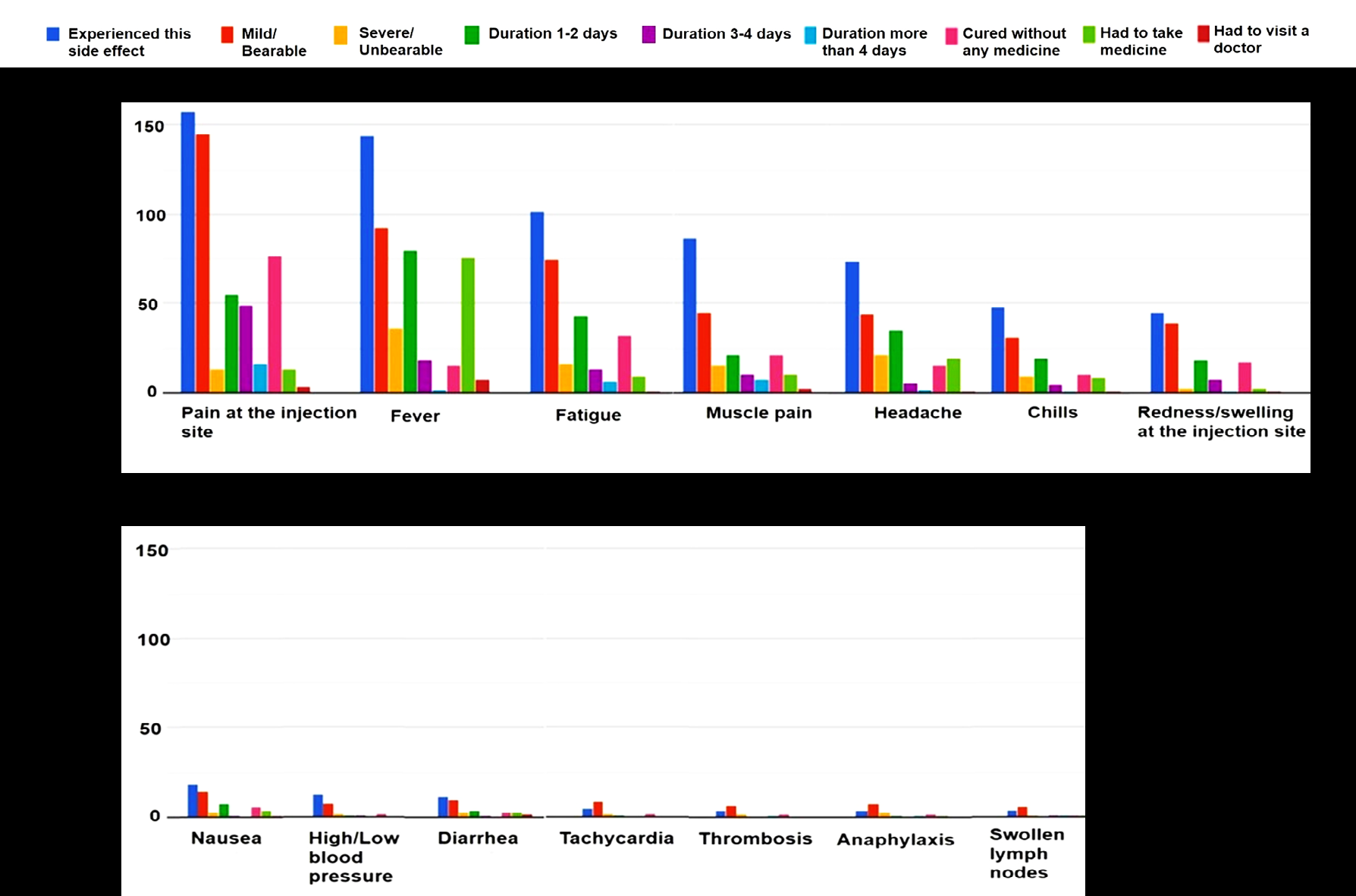
Duration and Severity of Side Effects: Within 11 hours of immunization, symptoms were observed (range 2-24 hours), with a 30-hour average duration. Figure 8 describes the type of side effects experienced from the most observed side effects (Figure 8A) to the least observed (Figure 8B), each with their duration (from 1-2 days to 3-4 days, and more than 4 days), severity (from mild/bearable to severe/unbearable), and if cured without medicine, or had to take medicine. Conclusions could only be made for side effects such as pain at the injection site, fever, fatigue, muscle pain, headache, chills, and redness/swelling at the injection site (Figure 8A), as participants showing nausea, high/low blood pressure, diarrhea, tachycardia, thrombosis, anaphylaxis, and swollen lymph nodes (Figure 8B) were few in numbers. The severity of post-vaccination symptoms was milder i.e., bearable with a duration of 2-3 days. Side effects like pain at the injection site, fatigue, muscle pain, and redness/swelling at the injection site were cured without any medicine. However, antipyretics had to be taken in case of fever. Similarly, analgesics were reported to be taken for headaches. None of the side effects were life-threatening nor did they demand hospitalization. Moreover, the severity of side effects was found significantly lower in the second dose.
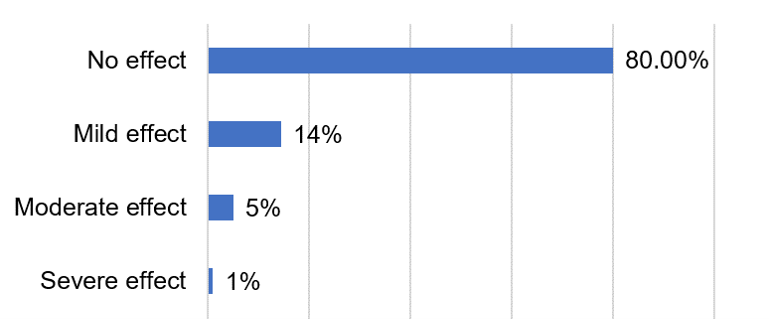
Post-vaccination Effect on Underlying Medical Conditions If Any: Amongst the individuals (37.8%) who were in doubt that vaccines may worsen their underlying medical conditions (Figure 1), and therefore were hesitant towards vaccination, most of them (80%) did not experience any ill effects of their health issues (Figure 9). Nearly 14% experienced mild effects, and 5% experienced moderate effects. Of notice, only 1% of them complained about the severity of their underlying medical condition as depicted in Figure 9.
Discussion
It has been proved earlier in history and by many studies how successful implementation of the vaccination program can help control epidemics and pandemics. Despite vaccination being the only long-term effective solution to reduce and thereby eliminate the virus, there have been several cases of vaccine hesitancy in the country. There are several issues concerning people when it comes to vaccination. Despite the vaccination program in India being more or less successful, vaccine hesitancy remains high. In our study females were found to have vaccine hesitancy more than males. Males feel the need to get vaccinated more frequently than females and are content with their vaccination decision. Another study also revealed that women were substantially more likely than men to suspect COVID-19 [11].
It was also found that a person’s educational background directly correlates with their decision to get vaccinated and whether or not they have enough information about the vaccine. As most of our study’s respondents had at least an undergraduate degree, there were lesser occurrences of vaccine hesitancy among them. As proven by another study [11], higher-educated people were aware of the technology behind the vaccines they received. While fear of needles remains an ignorant reason for vaccine hesitancy, some people delayed getting their shot due to the unavailability of their preferred choice of vaccine. Some did not want to be the first person to get vaccinated in their family and some believed that they were healthy enough to skip the vaccine. Additionally, access to COVID-19 vaccination is mainly determined by socio-economic status, with very low coverage in rural areas and among disadvantaged urban populations. As a result, Indians of all ages are increasingly resorting to private purchases, and the country’s minimal pension system makes this especially unaffordable for older people. Moreover, no special provision has been made to facilitate vaccine access for older and people with impaired mobility. For them, reaching vaccination centers was itself a big task. Some people tend to be less familiar with the digital technology required to make a booking. For some, the cost was the issue as private hospitals charge more for the vaccine than decided by the government, which is unaffordable for lower-income people as we saw in our study and other studies [12, 13, 14] also.
As far as the lack of confidence among people and their beliefs in conspiracy theories is concerned, it is seen that despite different socioeconomic, cultural, and biological characteristics, the beliefs of people in the study reflect an alignment in their psychological mindsets. These people tend to indulge in conspiratorial and paranoid beliefs making it hard for them to trust others, even authorized sources. They may hold strong religious and political beliefs and be less comfortable with change. They’re often impulsive and less conscientious. People often perceive the disease with less seriousness and therefore don’t feel the need to get vaccinated. A lower sense of responsibility is often associated with resistance to vaccines. If people start to think of getting vaccinated as a social responsibility, they might feel credible and accountable, as also reported in a study by Barello, et al. 2021 [15]. Concerns among the male and female population regarding impotency or low sperm count and infertility have also been seen. Similarities were seen in a study conducted in some Arab countries [16]. Of notice, only 2.7% of vaccinated individuals in our study were infected by the virus after the vaccination which discredits the belief of breakthrough infection occurring in people as some people were candidly worried about the same. However, in another study [11], a significant correlation between the development of COVID-19 and the incidence of side effects after the first dose was observed. Also, stronger side effects occurred after the second dose of the vaccine in those who had not previously been infected with COVID-19. The severity of COVID-19 clinical illness is linked to T-cell and antibody responses. Those who had previously been exposed to COVID-19 experienced more severe side effects after receiving the first dose of the COVID-19 vaccination, which could be due to decreased antibody-dependent enhancement (ADE) (cytokine storm).
As per the Union Health Ministry, India’s vaccination program against COVID-19 has been one of the most successful and largest in the world as it is a developing nation with a large population [12]. Since the start of the national COVID-19 vaccination drive on January 16 last year, India has administered over 90% of its eligible citizens’ first doses and 65% of second doses. However, there were great challenges during the implementation of vaccination programs in India, which also remains a cause for concern among individuals. The low proportion of vaccinated people was not only the result of vaccine hesitancy, but the crowd at the vaccination center, difficulty in registering for vaccination, and inability to get a slot were among the main concerns.
Most of the individuals experienced short-term side effects such as pain at the injection site, fever, fatigue, muscle pain, and headache. Some of them also experienced nausea, chills, and joint pain. Similar side effects were seen in other studies as well [11]. Concerning gender, post-vaccination side effects were more common in women than in males. Women have a higher innate and adaptive immune system than males, and as a result, they have a stronger immunological response to both foreign and self-antigen than men. Concerning age, the age group of 18–25 experienced more adverse effects than other age groups due to the stronger and more rapid immune response in the younger age group. Very few people over the age of 60 reported any symptoms. Aging results in a slow immune response to foreign antigens, and immune senescence, making them more susceptible to infectious diseases, and the efficacy of vaccines is also reduced [17]. Post-vaccination symptoms indicate a decrease in vaccine reactogenicity with age [17]. Although vaccine reactogenicity is linked to a brief increase in inflammatory cytokines, it is not regarded as a reliable indicator of a positive immune response [17].
Regarding duration and severity, short-term side effects were authentic but short-lived. Most of them reported that the severity of the post-vaccination symptom was milder, with few people observing symptoms worse than expected. Similarly, in another study [17] it was reported that the symptoms that were observed were neither life-threatening nor did they demand hospitalization. Concern about possible long-term side effects was the most important determinant of both unpredictability and reluctance to vaccinate against COVID-19. Although a maximum number of participants (72.4%) did not report any long-term side effects, some individuals did experience hair fall, joint pain, and effect on the menstrual cycle. However, the real scenario of long-term side effects cannot be determined as of now and this number may continue to increase as new COVID-19 cases occur. Long- term effect not only includes medical conditions, and mental health disorders such as fear, anxiety, anger, and depression during and after the post-COVID-19 pandemic, but the loss of loved ones, family members, and neighbors [18, 19, 20]. Many children have lost at least one parent to COVID-19.
Conclusion
In conclusion, the hesitation of people towards getting vaccination revolves around a variety of aspects including, brand name and quality of vaccine, presumptive notions, underlying health issues, stress and anxiety, implementation of the vaccination program, etc. Concern about side effects and possible long-term side effects were the most important determinants of both unpredictability and reluctance to vaccinate against COVID-19. However, the severity of the short-term effects was found to be very low, implying that vaccination is completely safe and that people should get vaccinated against this virus as soon as possible and should not worry about side effects that are milder and short-lived. No adverse effect on underlying medical conditions was seen post-vaccination, as some of them were conscious of their health issues. However, nothing can be claimed for long-term side effects as of now.
Declarations
Funding
The authors did not receive support from any organization for the submitted work.
Competing Interests
Authors have no financial or non-financial interests that are directly or indirectly related to the work submitted for publication.
Consent to participate
All the authors participated in the drafting and revisions.
Consent for publication
All the authors approved for publication
Availability of data and material
Survey data is available as supplementary data
Author Contributions
MKR contributed to drafting the work and revising it critically for important intellectual content, and final approval of the version to be published. JH, PU, RS, TN, AD, and IM contributed to drafting and revising the work
References
-
Lu R, Zhao X, Li J, Niu P, Yang B, et al. (2020) Genomic Characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet 395(10224): 565-574.
-
Feng H, Deng Y, Li W (2020) Coronavirus disease 2019: What We Know? J Med Virol 92(7): 719-725.
-
Huang C, Wang Y, Li X, Ren L, Zhao J, et al. (2020) Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 395(10223): 497- 506.
-
Chen N, Zhou M, Dong X, Qu J, Gong F (2020) Epidemiological and Clinical Characteristics of 99 Cases of 2019 Novel Coronavirus Pneumonia in Wuhan, China: A Descriptive Study. The Lancet 395(10223): 507-513.
-
Flaherty GT, Hession P, Liew CH, Lim BCW, Leong TK, et al. (2020) COVID-19 in adult patients with pre-existing chronic cardiac, respiratory and metabolic disease: a critical literature review with clinical recommendations. Trop Dis, Travel Med Vaccines 6: 16.
-
Tan W, Aboulhosn J (2020) The cardiovascular burden of coronavirus disease 2019 (COVID-19) with a focus on congenital heart disease. Int J Cardiol 309: 70-77.
-
Zhou Y, Chi J, Lv W, Wang Y (2021) Obesity and diabetes as high-risk factors for severe coronavirus disease 2019 (Covid‐19). Diabetes Metab Res Rev 37(2): e3377.
-
Aveyard P, Gao M, Lindon N, Boyce JH, Watkinson P, et al. (2021) Association between pre-existing respiratory disease and its treatment, and severe covid-19: a population cohort study. Lancet Respir Med 9(8): 909- 923.
-
Saini KS, Tagliamento M, Lambertini M, McNally R, Romano M, et al. (2020) Mortality in Patients with Cancer and Coronavirus Disease 2019: A Systematic Review and Pooled Analysis of 52 Studies. Eur J Cancer 139: 43-50.
-
Jayadevan R, Shenoy R, Anithadevi TS (2021) Survey of Symptoms Following COVID-19 Vaccination in India. Medrxiv.
-
Jeskowiak I, Wiatrak B, Dziewiszek PG, Szeląg A (2021) The Incidence and Severity of Post-Vaccination Reactions after Vaccination against COVID-19. Vaccines (Basel) 9(5): 502.
-
Bagchi S (2021) The World’s largest COVID-19 vaccination campaign. Lancet Infect Dis 21(3): 323.
-
Kumar VM, Perumal SRP, Trakht I, Thyagarajan SP (2021) Strategy for COVID-19 Vaccination in India: the country with the second highest population and number of cases. NPJ Vaccines 6(1): 60.
-
Sherlock PL, Kandiyil NM, McKee M, Perianayagam A, Venkatapuram S, et al. (2021) Pandemic Lessons from India: inappropriate prioritization for vaccination. BMJ 373: n1464.
-
Barello S, Palamenghi L, Graffigna G (2021) Looking inside the ‘Black Box’ of vaccine hesitancy: unlocking the effect of psychological attitudes and beliefs on covid-19 vaccine acceptance and implications for public health communication. Psychol Med 8: 1-2.
-
Sallam M, Dababseh D, Eid H, Mahzoum KA, Haidar AA, et al. (2021) High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines (Basel) 9(1): 42.
-
Lord JM (2013) The Effect of aging of the immune system on vaccination responses. Hum Vaccin Immunother 9(6): 1364-1367.
-
Jiang DH, Roy DJ, Gu BJ, Hassett LC, McCoy RG (2021) Postacute sequelae of severe acute respiratory syndrome coronavirus 2 infections: a state-of-the-art review. JACC Basic Transl Sci 6(9): 796-811.
-
Mose A, Haile K, Timerga A (2022) COVID-19 vaccine hesitancy among medical and health science students attending Wolkite University in Ethiopia. PLos One 17(1): e0263081.
-
Alwi SARS, Rafidah E, Zurraini A, Juslina O, Brohi IB, et al. (2021) A survey on COVID-19 vaccine acceptance and concern among Malaysians. BMC Public Health 21(1): 1129.
- Antifungal Activity of New Acetophenone Derivatives
- Interconnected Microbiomes Human Health Within an Environmental Framework
- Silkworm-Based Vaccine Production for H5N1: A One Health Approach to Pandemic Preparedness
- Microbial Diversity and Lipolytic Activity of Bacteria and Fungi from Oil-Contaminated Sites in Makurdi Metroplois
- Antibiotic Resistance Profile of Bacteria Isolated at the Central Laboratory of the National Hospital Center of Nouakchott
- Epidemiology and Sensitivity to Antibiotics of Germs Isolated from Blood Cultures in the Laboratory of the National Hospital Center of Nouakchott-Mauritania