Future Therapeutic Options for Alpha-1 Antitrypsin Deficiency
Alpha-1 antitrypsin deficiency (AATD) is a genetic disorder that results in low circulating levels of alpha-1 antitrypsin (AAT). Low levels of AAT can result in damaged lung tissue, and pro-inflammatory state. The accumulation of polymerized Z-AAT protein within hepatocytes also causes cytotoxicity, resulting in liver cirrhosis. The current therapy includes weekly augmentation with plasma derived products. This has not proven to affect the progression of liver disease. Current research is targeting new modalities of treatment that will improve the progression of liver toxicity related to the polymerization of the Alpha-1 protein in the hepatocytes, in addition to offering patients more flexible treatment options, including oral therapy and less frequent intravenous infusions. These novel therapies include recombinant protein therapy, small molecule correctors,inhaled AAT therapy, RNA interference and monoclonal antibodies. The anti-inflammatory effect of Alpha-1 therapy is being explored in other disease states, including COVID-19 Pneumonia.
Introduction
Alpha-1 antitrypsin deficiency (AATD) is a genetic disorder characterized by low circulating levels of alpha-1 antitrypsin (AAT). AAT is produced primarily in the liver and secreted into the blood, although other cell types, including lung epithelial cells, monocytes, macrophages, and neutrophils, produce the protein locally. AAT inhibits several serine proteinases secreted by inflammatory cells (most notably neutrophil elastase, cathepsin G, and proteinase-3) and thus protects organs such as the lung from damage by these proteinases, especially during periods of infection and increased inflammation. A single point mutation in the Z-allele of SERPINA1 (the gene encoding AAT) leads to protein misfolding, intracellular polymerization of misfolded mutant Z-AAT protein, and reduced secretion of active Z-AAT protein. Consequently, circulating AAT levels in individuals homozygous for the Z-allele (PiZZ) are markedly reduced; only approximately 15% of Z-AAT protein folds correctly and is secreted by the cell. The reduced levels of circulating, active AAT result in an imbalance between proteinase and antiproteinase activity, which has its greatest impact in the lung. Alpha one protein also inhibits other neutrophil proteases, such as protease – 3 and cathepsin – G, and counters the cytotoxic effect of neutrophil defensins. This will help to maintain a balanced milieu between anti- and pro- inflammatory proteins in the lower respiratory tract. Consequently, lung tissue is damaged over time, resulting in emphysema, a form of chronic obstructive pulmonary disease (COPD). This effect is most pronounced in PiZZ individuals and typically manifests in middle age. The accumulation of polymerized Z-AAT protein within hepatocytes causes cytotoxicity that can result in neonatal liver disease or progressive liver disease in adulthood that can lead to cirrhosis or liver cancer. Alpha-1 antitrypsin deficiency is estimated to affect 1 in 2,500 people in the USA, Australia, UK, and Europe. Approximately 3% of subjects with chronic obstructive pulmonary disease (COPD) are thought to have AATD. Barriers to treatment of AATD include under diagnosis, the high cost of chronic augmentation therapy, and the need for weekly intravenous (IV) infusions.
Discussion
Underdiagnosis of AATD likely stems from a misperception of low prevalence, misinformation about the usual presentation of a patient, and a misunderstanding that AATD and other chronic lung diseases are mutually exclusive diseases. The average age of diagnosis for AATD is 45.5 + 9.5 years, with 30% of patients diagnosed after 50 years of age. It has been reported that patients with AATD often endure a delay in diagnosis of approximately 8 years [1]. The following, Box 1, summarizes the ATS/ERS recommendations regarding identifying patients for AATD testing.
Box 1: ATS/ERS Task Force recommendations on which individuals should undergo diagnostic testing for AATD (Type A categorization) and for women discussion of testint is appropriate (Type B categorization) [1].
Type A: Recommendation for Testing
- All adults with symptomatic emphysema. Regardless of smoking history
- All adults with symptomatic COPD, regardless of smoking history
- All adults with symptomatic asthma whose airflow obstruction is incompletely after bronchodilator therapy
- Asymptomatic patients with persistent obstruction on pulmonary function tests with identifiable risk factor (ie. Cigarette smoking, occupational exposure)
- Sibling of individual with AATD
- Individuals with unexplained liver disease and adults with necrotizing panniculitis Type B: Discussion for Testing
- Adults with bronchiectasis without evidence of etiology
- Adolescents with persistent airflow obstruction
- Asymptomatic individuals with persistent airflow obstruction and no risk factor
- Adults with positivity for cytoplasmic antineutrophil cytoplasmic antibodies (antiproteinase-3) vasculitis
- Individuals with a family history of COPD or liver disease not known to be attributed to AAT
- Immediate of distance relatives of an individual homozygous for AATD Figure 1 summarizes one of the diagnostic approaches to diagnosing alpha one deficiency. The serum level is acute phase reactant and the level will increase with acute exacerbation of the underlying lung disease, in addition to acute inflammatory process and malignancy. Once diagnosed with AATD, patients have limited options for treatment. Augmentation therapy using plasma-derived AAT (pdAAT) has been in use since 1987, and there are currently 4 pdAAT products approved by the US Food and Drug Administration (FDA): Prolastin®/Prolastin-C®, Aralast®, Zemaira®, and Glassia®. Plasma-derived AAT is purified from pooled human plasma and given via IV once a week at a dosage of 60 mg/kg, aiming to maintain AAT serum concentrations at more than the accepted protective threshold of 11 μM. Trough antigenic and functional AAT levels have been used as endpoints for pivotal trials to license these approved pdAAT products. Bronchoalveolar lavage (BAL) is used to determine whether or not AAT augmentation produces measurable increases in the antielastase activity in pulmonary epithelial lining fluid (PELF) in the lung. While no randomized controlled study was conducted to demonstrate pulmonary function or survival benefits of augmentation therapy with pdAAT, observational and cohort studies support the benefit of augmentation in reducing the rate of decline in lung function as determined by rate of loss in forced expiratory volume in 1 second (FEV1); a reduction in mortality was seen in the largest of these studies [3]. Not only are there limited options for treatment, there are multiple barriers to augmentation therapy as well. Chronic augmentation therapy comes with a high cost that is oftentimes not covered by insurance, along with the need for patients to receive weekly IV infusions.
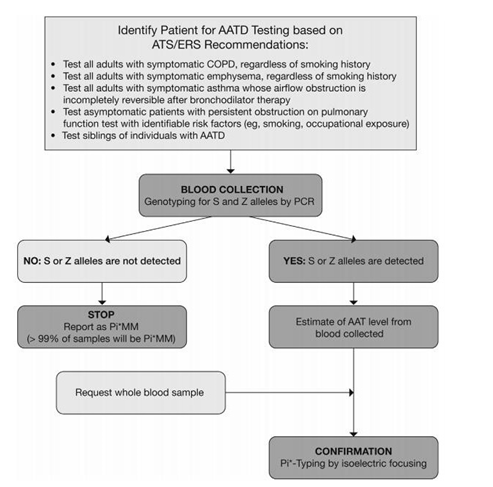
Figure 1: Example of an AATD testing algorithm. With this scheme, rare allele variants will not be picked up and further investigation may need to be considered if clinical suspicion of AATD is high. AAT, alpha1 –antirypsin deficiency; ATS: American Thoracic Society; COPD: Chronic obstructive pulmonary disease; ERS: European Respitaroty Society; PCR: Polymerase Chain Reaction; Pi: Proteinase Inhibitor.
The weekly infusions can lead to the need for a port placement for patients, along with a limitation in their weekly schedules. Current research is working toward introducing new options for therapy [4].
Recombinant Protein Therapy
Inhibrx rhAAT-Fc (INBRX-101) is intended for chronic augmentation and maintenance therapy in adults with emphysema due to AATD. The active ingredient of INBRX-101 is a recombinant protein comprised of 2 human alpha-1 protease inhibitor (A1PI, A1AT, or AAT) molecules covalently linked to the Fc domain of human IgG4. The recombinant AAT sequences are derived from the human sequence (UniProtKB - P01009; A1AT) with the addition of 2 amino acid changes to prevent loss of activity in oxidative environments, such as the lung and sites of inflammation. In addition, the human IgG4 Fc portion of the molecule includes 2 amino acid changes for hinge stabilization and effector function silencing, and 2 additional mutations to extend plasma half-life. In contrast, to the current marketed plasma derived AAT products for which exposures drop below the normal range when dosed weekly, INBRX-101 is intended to maintain exposures within the normal range observed in non-AAT deficient individuals with a less frequent dose schedule.
INBRX-101 has been shown to inhibit human, cynomolgus monkey, and rodent neutrophil elastase with comparable molar activity to a plasma derived AAT (pdAAT) comparator, Prolastin-C. The pharmacological relevance of these preclinical species has allowed investigation into the function and safety of INBRX-101 in a variety of settings. In a mouse model of acute pulmonary inflammation induced by intranasal lipopolysaccharide (LPS), treatment with INBRX-101 or pdAAT reduced neutrophil elastase activation, as measured by an activatable imaging agent (NE680), to near baseline levels. In contrast, 90% of mice exposed to LPS without AAT treatment showed a high signal. These data suggest that pdAAT and INBRX-101 had significant impact on neutrophil elastase activity in the lung when administered systemically.
The potential for INBRX-101-related effects on safety pharmacology, including neurological, respiratory, or cardiovascular parameters, was evaluated in Good Laboratory Practice (GLP)-compliant, repeat-dose, IV toxicity studies in Sprague-Dawley rats and cynomolgus monkeys. Repeated administration of INBRX- 101 to male and female Sprague Dawley rats at 50, 150, or 450 mg/kg/dose once weekly for three months was well tolerated and did not result in any adverse findings. The no observed adverse effect level (NOAEL) was 450 mg/kg/dose. Similarly, repeat intravenous infusion of INBRX-101 to male and female cynomolgus monkeys at 50, 150, or 450 mg/kg/dose once weekly for three months was well tolerated, with the no observed effect level (NOEL) considered to be 450 mg/kg/dose. In both studies, the achieved exposures are expected to be at or above the anticipated human exposure at therapeutic doses.
Pharmacokinetic (PK) data in rats and cynomolgus monkeys demonstrate that the half-life extended Fc domain portion of INBRX-101 achieves a substantially prolonged half- life, as compared to plasma derived products. Particularly in cynomolgus monkeys, the half-life of INBRX-101 is approximately 15 days, which compares favorably to the published human half-life of 4.6 days for Glassia®, 5.1 days for Zemaira®, 5.9 days for Aralast® and 6.1 days for Prolastin-C®. A clinical study is ongoing to confirm this extension in humans, which would allow for a significantly longer dosing interval, while maintaining AAT equivalent trough levels in the normal range. This profile would likely be more protective against progression of emphysema than pdAAT dosed at the approved dose of 60 mg/kg, with significantly fewer infusions annually [5].
Small Molecule Corrector
Polymerization of the Z protein in the hepatocyte is another possible treatment option. Ninety five percent of severe deficiency of AAT results from the Glu342Lys mutation or Z allele. This mutation arose approximately 2000 years ago and is found in 1 out of 25 of the North European white population with 1 out of 2000 individuals carrying 2 Z alleles (homozygotes). The Z mutation causes approximately 70% of the synthesized protein to be degraded by the proteasome, 15%-20% misfolds to form ordered intracellular polymers and 10%-15% folds normally and is secreted into the circulation.3 The intracellular polymers are sequestered within the endoplasmic reticulum as Periodic Acid Schiff- positive, diastase resistant inclusions 2,4 that are associated with neonatal hepatitis, cirrhosis and hepatocellular carcinoma. The intracellular polymerization of Z AAT occurs in the context of chaperone-mediated folding, proteasomal degradation and a cooperative proteostatic network. Small molecule corrector has the potential to restore physiological levels of circulating AAT activity and thus reduce the risk of lung disease. By preventing Z-polymer formation in the liver, they may also reduce the risk of developing progressive liver disease (fibrosis and cirrhosis). The Z protein is less active than the M protein against neutrophil elastase. Smoking and infection have the potential to oxidize the Z protein which does further reduce the activity to protect the lung. Clinical trials will be needed to determine the need for augmentation therapy along with oral therapy in patients with the ZZ phenotype, especially with active infection or exacerbation of the underlying lung disease [6].
Inhaled Therapy
Inhalation therapy is currently being developed and tested as well. Direct delivery of AAT to the lung by nebulization might have a higher impact on airway inflammation than intravenous augmentation therapy. The inhalational therapy offers the opportunity of easier and more efficient delivery of AAT to the lungs, enriching the epithelial lining fluid with AAT levels at least 3 times higher than those achieved by the IV route. This would enhance the local antielastase effect, in addition to inhibiting inflammation and proinflammatory cytokines. The RAPID trial in 2015 showed a statistically significant slower decline in lung density, but no effect on lung function. In addition, there was no significant effect on COPD exacerbation. The lack of effect on exacerbation in the RAPID trial could be due failure to include exacerbation prone patients or lack of diary cards to monitor the events. However, it is possible that alpha one level in the airways is insufficient to modify inflammation and the risk of exacerbation when treatment is delivered by the intravenous route. Brantly, et al. [7] conducted clinical trial studying the effect of inhaled AAT on lower respiratory tract Protease- Anti- Protease homeostasis in Pi ZZ patients using bronchoalveolar lavage (BAL). The study showed inhaled AAT restored protease anti- protease homeostasis, and reduced the percentage of neutrophils and neutrophil elastase concentration in the lower respiratory tract in AAT deficient individuals. Detection or normal M protein in the plasma of study subjects indicate the inhaled AAT passed from the alveolar compartment and the interstitial space [7].
Stolk, et al. [8] conducted a multicenter, double blind placebo-controlled trial over 50-week period in patients with the ZZ phenotype with diagnosis of emphysema confirmed by computed tomography (CT) scan with serum level below 11 micromoles. The inclusion criteria included two or more moderate to severe exacerbations requiring a change in the treatment or hospitalization over the previous 18 months. Eligible patients were randomized 1 to receive a twice daily inhalation of human plasma – derived AAT (80 mg in 4 mL, high purity liquid ready to use in sterile, single – use glass vials or placebo. The treatment duration was 50 weeks. Each nebulized session lasted 8 to 15 minutes. The study concluded inhalation therapy with AAT has no effect on the time to first exacerbation in patients with severe COPD and history of frequent exacerbation during the 50-week treatment period. Th safety profile was similar between the groups. The AAT group did not experience a reduction in the lung function at the end of the study, which decreases the possibility that they inhaled Alpha-1 Antitrypsin may have experienced hypersensitivity reaction. The rapid increase in FEV1 after 4 weeks of inhaled FEV1 and the decline of FEV1 after 4 weeks of stopping treatment warrants further clinical trials with rate of decline in FEV1 as the primary end point [8].
Endobronchial Lung Volume Reduction
It is performed by one-way valves placed by flexible bronchoscope. The data are limited to case series. The insertion of one-way endobronchial valves in 15 individuals with AATD resulted in an increase in FEV1 of 54% after 12 months in 12 of the individuals, quality of life was much improved and 2 individuals were taken off oxygen therapy. There was no significant deterioration in lung function during the 4-year follow-up.22 However, there were complications in 3 of the individuals: 1 developed a pneumothorax and had valve displacement and subsequent removal, 1 coughed up the valves after 2 months and 1 developed repeated and severe pneumonia and the valves had to be removed [6].
Small Interfering RNA to Silence the Expression of Z Alpha-1 Antitrypsin
RNA interference- based approaches to silence Z AAT synthesis within hepatocytes is another treatment modality for liver disease. RNA interference, or RNAi, is a mechanism present in living cells that inhibits the expression of a specific gene, thereby affecting the production of a specific protein. Arrowhead Pharmaceuticals, Inc. released information on 28APR2021 regarding the positive study results from their open label phase 2 clinical ARO-AAT, RNAi therapy trial. This RNAi treatment will silence the alpha-1 antitrypsin Z protein production in affected individuals, which would lead to the decrease of toxic accumulation of Z alpha-1 antitrypsin in the liver, in turn reducing liver fibrosis [2].
Intrabodies as a Strategy to Block Intracellular Polymerization and Increase Secretion of Z Alpha-1 Antitrypsin
Monoclonal antibody technology has allowed the identification of antibodies that detect the polymeric4 and latent70 conformers of AAT and antibodies that can block71 and accelerate72 polymer formation. The 4B12 monoclonal antibody blocked AAT polymerization at a 1:1 molar ratio in vitro by binding to an epitope that encompasses residues Glu32, Glu39 and His43 on helix A and Leu306 on helix I.73 This antibody identified a region that may be targeted for the rational design of ligands that can dynamically influence AAT polymerization. Moreover, the expression of a single chain-variable-fragment intrabody of mAb4B12 reduced the intracellular polymerization of Z AAT by 60% and increased the secretion of Z AAT that retained inhibitory activity against neutrophil elastase71. This demonstrates that monoclonal antibodies can block the transition of Z AAT to aberrant polymers without compromising inhibitory activity of the protein [6].
AAT therapy is also being investigated for use in other disease states: The alpha one molecule modulates different cell types during inflammation. There are several lines of evidence implication AAT as a participant in the immune response. In addition, AAT is an acute – phase reactant. Upregulation of AAT occurs in response to infection and tissue injury to aid in tissue repair. AAT also inhibits various lymphocyte cytotoxic reactions, including T-cell, natural killer cell, and antibody dependent cell–mediated processes. The anti- inflammatory effects and tissue healing of alpha one indicates other potential therapeutic uses of AAT in addition to replacement therapy. This may include Diabetes mellites, inflammatory bowel disease and graft versus host disease [9].
Cytokine storm is an umbrella term that encompasses several disorders of immune dysregulation characterized by constitutional symptoms, systemic inflammation and multiorgan dysfunction. This can lead to multiorgan failure and death if inadequately treated in a timely manner. Covid-19, which is caused by SARS- CoV-2, is characterized by heterogenous symptoms ranging from mild fatigue to life- threatening acute respiratory failure. Cytokine storm was also reported in patients with SARS and was associated with poor outcomes. Elevated levels of cytokines and hemophagocytosis contribute to the pathogenesis of Covid-19. According to clinicaltrials.gov, AAT is currently under investigation in a randomized placebo controlled clinical trial as a potential therapeutic option for patient with Covid-19 pneumonia [1].
![Figure 2: AAT Modulation of different cell types during inflammation [1].](/fulltextimages/7420/fig_2.png)
Conclusion
AATD is a disease in which patients experience delayed or missed diagnosis, lack of treatment options and multiple treatment barriers. Research continues to move forward for AATD, with hopes of advancing a wider range of therapeutic options. Currently, there are multiple advanced therapeutic options for the treatment of AAT which include oral, inhalation and intravenous infusion being studied. These therapeutic options will allow AATD patients to have more flexibility than they currently have with weekly augmentation therapy. The development of a variety of treatments for AATD is likely to have a positive impact on other disease states with inflammation and cytokine storm responses as well.
References
-
Farah H, Steinbeck K, Sadikot R (2020) Potential Anti- Inflammatory Approaches for the Management of SARS- CoV2 Infections. J Pulmon Respir Sci 5(S1): 1-6.
-
Alpha-1 Foundation (2021) Arrowhead Announces Improvement in Fibrosis after ARO-AAT Treatment in Patients with Alpha-1 Liver Disease.
-
Teschler H (2015) Long-term experience in the treatment of α1-antitrypsin deficiency: 25 years of augmentation therapy. Eur Respir Rev 24(135): 46-51.
-
Siri D, Farah H, Hogarth DK (2013) Distinguishing alpha1-antitrypsin deficiency from asthma. Ann Allergy Asthma Immunol 111(6): 458-464.
-
Lomas, DA (2018) New Therapeutic Targets for Alpha-1 Antitrypsin Deficiency. Chronic Obstr Pulm Dis 5(4): 233-243.
-
Brantly M, Stock J, Rouhani F, Lascano J, Jeffers A, et al. (2020) Inhaled Alpha-1 Antitrypsin Restores Lower Respiratory Tract Protease – Anti-Protease Homeostasis and Reduces Inflammation in Alpha-1 Antitrypsin Deficient Individuals: A Phase 2 Clinical Study Using Inhaled Kamada-API. Am J Respir Crit Care Med 195: A7677.
-
Stolk J, Tov N, Chapman KR, Fernandez P, MacNee W, et al. (2019) Efficacy and safety of inhaled alpha-1-antitrypsin in patients with severe alpha-1-antitrypsin deficiency and frequent exacerbations of COPD. Eur Respir 54: 1900673.
-
Bergin D, Hurley K, McElvaney NG, Reeves EP (2012) Alpha-1 Antitrypsin: A Potent Anti- Inflammatory and Potential Novel Therapeutic Agent. Arch Immunol Ther Exp (Warsz) 60(2): 81-97.
- Bedside Pulmonary Rehabilitation – Mandatory and Cost- Effective Tools
- The Role of Chest Radiology in Traumatic Injuries: A Comprehensive Narrative Review
- Pseudosepsis in Acute Inflammation of the Lung
- An Overview of Lung Injury in Covid-19: Evaluating the Impact of Re-Exposure and Emerging Variants
- Fibreoptic Bronchoscopy-its Role in Pulmonary Medicine-Current Trends in Intensive Care Unit
- Retrospective Study on the Efficacy of Homoeopathic Medicines in the Treatment of Acute Rhinitis