Fibreoptic Bronchoscopy-its Role in Pulmonary Medicine-Current Trends in Intensive Care Unit
Fibreoptic Bronchoscopy is an endoscopic procedure to visualize the tracheobronchial tree and also to obtain bronchial washings, biopsies, brush smears, transbronchial biopsies to arrive at an etiological diagnosis of the underlying disease process responsible for the nonresolving shadows in the lung, these can facilitate therapeutic decision. Utilization of bronchoscopy in the intensive care unit (ICU) has made the diagnosis and treatment of many diseases presenting as acute respiratory illness, more possible to interventional pulmonologists and intensivists although challenging in the critical ill cases, specially in ventilator support. We report our one year experience with the use of flexible fiberoptic bronchoscopy. A total 205 cases were undergone this procedure during Aug 2022 till July 2023 out of which 169 cases were taken up from the wards and rest 36 cases were taken up from the intensive care units. Pre-bronchoscopy screening was done. Of 205 patients, there were 124 Male patients and 81 Female patients. Mean age of the patients was 50.1 years. Among 169 cases in the ward were mainly non-resolving consolidation in 99 (58%) cases followed by pulmonary mass lesion in 31(18.3%) cases, Cavitary lesion in 22 (13%) cases, collapse with bronchiectasis-18(10.6%) and in 16 cases with hemoptysis with Normal X-ray. The diagnostic yield were Pulmonary infection - Non TB- 46 %, Tuberculosis-8%, Malignancy 17% – Squamous cell carcinoma-2 cases (18%), Adenocarcinoma 4 cases, Small Cell carcinoma -5 cases Bronchoscopy has ultimately lead to change in therapy in 70% cases, Bronchoscopy among 36 (17.5%)cases in ICU were mainly related to non-resolving consolidation 12(33%), hemoptysis 8(22.4%), for tracheal intubation-3(8.3%). Therapeutic bronchoscopy was performed in collapse due to retained secretion in 13(36%) cases. Complications were minimal indicating its safety in expert hands.
Introduction
- Bronchoscopy is an endoscopic procedure to visualize the tracheobronchial tree and also to obtain bronchial washings, biopsies, brush smears, transbronchial Commentary biopsies to arrive at a conclusion of the underlying disease process.
- Flexible fibreoptic bronchoscope is an essential tool in Interventional pulmonology in recent times. It helps the physician in getting a firm and confirmatory diagnosis in obscure pulmonary diseases specially nonresolving shadows in the lung which can influence the therapeutic decision-making.
- Utilization of bronchoscopy in the intensive care unit (ICU) has made the diagnosis and treatment of many diseases presenting as acute respiratory illness, more possible and feasible to pulmonologists and intensivists.
- Risks and benefits of bronchoscopy should be carefully considered in critically ill patients. The hypoxic patients in ICU pose a challenge as hypoxemia is one of the known complications of bronchoscopy, and this risk is exacerbated in patients with hypoxic respiratory failure.
Therefore, the aim of this study is to report our one year experience with the yield of flexible fiberoptic bronchoscopy at Kalinga Institute Medical sciences, a tertiary respiratory care hospital in Bhubaneshwar.
Methods
This study was a retrospective review of the number of Bronchoscopies performed at in Kalinga Institute of Medical Sciences during the period Aug 2022- July 2023. Cases were included from both Wards and ICU undergoing bronchoscopy during the period.
Bronchoscopy was performed in these patients and collection of pulmonary samples where ever feasible including bronchial washing, bronchial brushing, bronchial biopsy and transbronchial needle aspiration was done.
A total of 205 patients who underwent bronchoscopy during the specified time period. Of which 169 patients were from various wards mainly from Dept of Pulmonary Medicine and 36 patients were from ICUs.
Pre-bronchoscopy screening was done with history, physical examination, PT-INR, X-ray chest PA view, ECG, HRCT Thorax, sputum smear for AFB. All FOBs were performed by spraying 10% lignocaine in the oropharynx. Patients were instructed NPO for 6-8 hours prior to the procedure. Informed consent was taken.
Demographic characters like age, sex, symptoms, Indications, bronchoscopic findings, samples collected, outcomes etc were critically reviewed in all the patients who underwent bronchoscopy in this period. All bronchoscopic examinations were done using a video assisted flexible bronchoscope (Pentax, Olympus) by experienced respiratory interventionists.
Results
A Total number of 205 patients underwent bronchoscopy during time period Aug 2022 – July 2023. Of 205 patients, there were 124 Male patients and 81 Female patients. Mean age of the patients was 50.1 years. Of the 205 brochoscopies performed 169 were performed in bronchoscopy suite, while 36 were performed in the ICU.
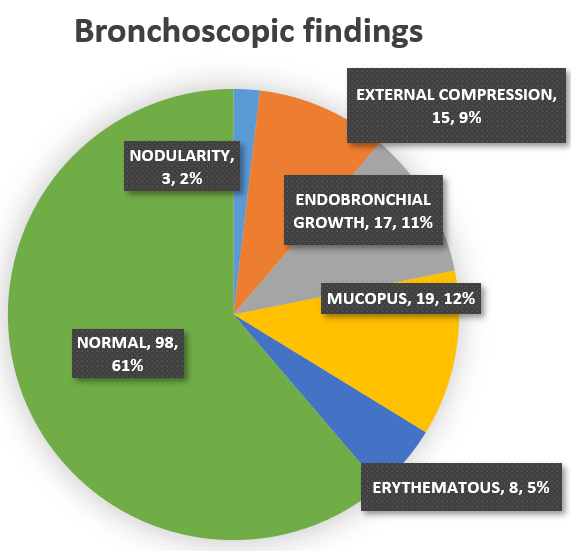
Indications of bronchoscopy among 169 cases in the ward were mainly non-resolving consolidation in 99 (58%) cases followed by pulmonary mass lesion in 31(18.3%) cases, Cavitary lesion in 22 (13%) cases, collapse with bronchiectasis-18(10.6%) and in 16 cases with hemoptysis with Normal Radiographic findings Table 1 & Figure 1.
| Indications | No. of Patients |
|---|---|
| Non Resolving Consolidation | 99 |
| Lung Mass | 31 |
| Cavitatory lesions | 22 |
| Nodular/Reticulonodular lesions | 15 |
| Hilar Lymphadenopathy | 3 |
| Collapse | 18 |
Table 1: Indication in Patients from Wards.
Procedures Performed
Bronchial washing, bronchoalveolar lavages, bronchial brushing, bronchial biopsy and transbronchial needle aspiration was performed (Table 2).
| Procedure | Number done | Positive Results | % Yield |
|---|---|---|---|
| Bronchoalveolar Lavage | 124 | 72 | 58.06% |
| Endobronchial Biopsy | 27 | 16 | 59.25% |
| Brush Biopsy | 15 | 6 | 40% |
Table 2: Bronchoalveolar lavage was collected from 124 patients of which 72 (58.06%) patients have positive cultures, 27 biopsies
The diagnostic yield were Pulmonary infection - Non TB- 46 %, Tuberculosis-8% , Malignancy 17% – Squamous cell carcinoma-2 cases (18%), Adenocarcinoma 4 cases , Small Cell carcinoma -5 cases. Bronchoscopy has ultimately lead to change in therapy in 70% cases.
Brochoscopy in ICU
Bronchoscopy is considered a low-risk procedure in healthy patients or patients with mild, stable cases . However, in patients of ICU with pre-existing hypoxic respiratory failure pose a unique challenge for the bronchoscopist.
Monitoring in ICU Brochoscopy
We routinely perform in ventilated cases to enhance the pressure and peep settings and FiO2 respectively prior to the performing the insertion of the fibreoptic bronchoscope to achieve the ideal oxygenation around 95%, after this careful clinical monitoring then we go ahead with the visualisation of the tracheobronchial tree and necessary diagnostic or therapeutic procedures as deemed proper are performed, incase of persistent desaturation below 88%, bronchoscope will be withdrawn from the airway for a few moments and either FiO2 or PEEP should be increased. Patient’s oxygen saturation should increase to 95% or above prior to resuming the bronchoscopy, and collections of the pulmonary samples were performed, the procedure in totality takes five minutes on an average.
Continuous monitoring of the Spo2, Pulse Rate, Respiratory Rate invasive / Non –invasive BP Monitoring will be done throughout the procedure. The absolute contraindications are severe refractory hypoxemia, refractory shock.
The indications of the bronchoscopy among 36 (17.5%) cases in ICU were mainly related to non-resolving consolidation 12(33%), hemoptysis 8(22.4%), for tracheal intubation-3(8.3%). Therapeutic bronchoscopy was performed in collapse due to retained secretion in 13(36%) cases Table 3 & Figure 2.
| Indications | No of Patients |
|---|---|
| Non resolving consolidation | 12 |
| Haemoptysis/ to identify bleeding site | 8 |
| Removal of retained secretions/Mucus plugs responsible for collapse | 13 |
| Tracheal intubation | 3 |
Table 3: Indications in ICUs.
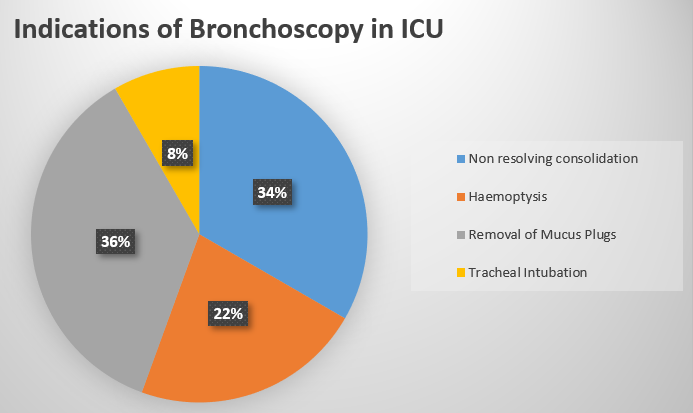
Figure 2: Total of 36 procedures was done in ICU between Aug 2022 July-2023. Therapeutic interventions were done for 12 patients, and the remaining 24 procedures were performed for diagnosis. Therapeutic interventions in intubated/Tracheostomised cases mainly included removal of mucus plugging/retained secretions responsible for the airway obstruction and collapse leading to reaeration of the affected lobes of the lung.
Complications
We encountered minor Complications like Bleeding, Desaturation which were managed conservatively. 2 patients of 169 (1.1%) were shifted to ICU post procedure as a precautionary measure for close observation. There was no mortality till date.
Conclusion
- Bronchoscopy is an invaluable and assisting tool in the diagnosis and management of a variety of undiagnosed respiratory diseases.
- Being a safe procedure in expert hands it is a useful tool to diagnose obscure lung diseases in ICU and wards patients specially non-resolving shadows in the lung.
- The overall diagnostic yield was 56.6% and leads to change in therapy in 70% patients in ward and 50% cases in ICUs.
- Zero Mortality with trivial manageable complication.
It is a safe procedure with good diagnostic value in expert hands. Disclaimer –Nothing to declare.
- Bedside Pulmonary Rehabilitation – Mandatory and Cost- Effective Tools
- The Role of Chest Radiology in Traumatic Injuries: A Comprehensive Narrative Review
- Pseudosepsis in Acute Inflammation of the Lung
- An Overview of Lung Injury in Covid-19: Evaluating the Impact of Re-Exposure and Emerging Variants
- Retrospective Study on the Efficacy of Homoeopathic Medicines in the Treatment of Acute Rhinitis
- Humoral and Cellular Immune Response among Kidney Transplant Recipients after COVID-19 Vaccination: A Systematic Review and Meta-Analysis