Humoral and Cellular Immune Response among Kidney Transplant Recipients after COVID-19 Vaccination: A Systematic Review and Meta-Analysis
A comprehensive search was carried out in mainstream bibliographic databases or Medical Subject Headings, including ScienDirect, PubMed, Scopus, and ISI Web of Science. The search was applied to the articles that were published between 2021 and mid-2023. With strict literature search and screening processes, it yielded 7 articles from 349 articles of initial literature database. A number of previous studies emonstrated that KTRs or non-KTRs with renal failure markedly reduced vaccine response, whereas adaptive protocols of mRNA COVID-19 vaccination or alternative adjuvant vaccines is now not known yet. A recent study revealed that acute kidney injury and mortality could be caused by SARS-CoV-2 (COVID-19) around 50 % and 23 % of the infected KTRs.
Objectives of the Study
The objectives of this study are to identify the better understanding on the immunological responses, both humoral and cellular types between the types of COVID-19 vaccine and number of doses, risk of SARS-CoV-2 (COVID-19) infection and disease and transplantation age among previous hemodialysis or non-hemodialysis patients with kidney transplantation with or without immunosuppressive therapies.
Introduction
With different mRNA COVID-19 vaccination in immunocompromised patients, such as kidney transplant recipients (KTRs), solid organ transplant recipients (SOTRs), etc., binding and neutralizing antibodies measurement clearly revealed lower levels, compared to healthy persons [1, 2, 3, 4, 5]. A number of previous studies demonstrated that KTRs or non-KTRs with renal failure markedly reduced vaccine response, whereas adaptive protocols of mRNA COVID-19 vaccination or alternative adjuvant vaccines is now not known yet [6, 7]. Whereas protective immunity is further impaired immunosuppressants, thus fully restoring adaptive, cellular immunity and renal function in KTRs cannot occur and increase susceptibility to viral-related malignancies and infections [8, 9, 10].
A recent study revealed that acute kidney injury and mortality could be caused by SARS-CoV-2 (COVID-19) around 50 % and 23 % of the infected KTRs [11]. Among KTRs, severe COVID-19 remained with unchanged high mortality rate of approximately 5 % to 10 % through conventional vaccine strategies [12]. Due to recent introduction of the modified vaccine strategies, initial recommendation of COVID-19- Vaccine-booster doses was made [2, 13, 14, 15, 16, 17].
Methods of the Study
Search Strategy and Inclusion Criteria
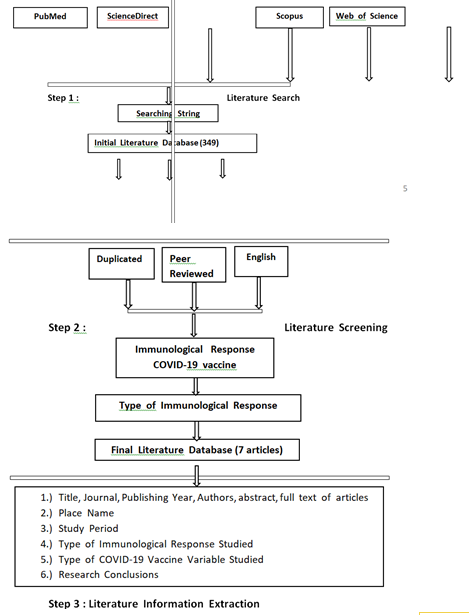
A comprehensive search was carried out in mainstream bibliographic databases or Medical Subject Headings, including ScienDirect, PubMed, Scopus, and ISI Web of Science. The search was applied to the articles that were published between 2021 and mid-2023. Our first involved performing searches of article abstract/keywords/title using strings of [(Kidney Transplantation ” or “ Kidney Transplant Recipient ”, “ SARS-CoV-2 ” or “ COVID-19 ” and “ Vaccine ” or “ Vaccination”, “ Humoral Immunity ” or “ Humoral Immune ” or “ Humoral Immune Response ”, “ Immunosuppressants ” or “ Immunosuppressive Regimens ”, “ Dialysis ”)]. After a first approach of search, published articles focusing on kidney transplantation were retained and the information on immunological response type and COVID-19 vaccination was extracted for having a crude knowledge involving their themes. Another round of publication search was conducted for adding the missing published articles that were not identified by the first round.
All keywords combinations from one immunological response type and immunosuppressive regimen variable to bind the population of cases under consideration. Search string for COVID-19-vaccine-type groups include [“ Recombinant Subunit Vaccines ” or “ Protein Subunit Vaccine ” or “ Virus-like Particle (VLP) Vaccine ” or “ Nucleic Acid Vaccines ” or “ DNA-based Vaccines ” or “ RNA-based Vaccines ” or “ Viral Vector Vaccines ” or “ Non-replicating Viral Vector Vaccines ” or “ Replicating Viral Vector Vaccines ” or “ Whole Virus Vaccines ” or “ Inactivated Vaccines ” or “ Live-attenuated Vaccines ”].
The initial literature databases were further manually screened with the following rules:
- Non-kidney-transplanted-recipient-related articles were excluded.
- Articles that did not report a human-humoral- immunological-response or human-immunological- response related to COVID-19 vaccination were not considered, such as commentary articles, or editorial.
- Non-peer reviewed articles were not considered to be of a scholarly trustworthy validity;
- Duplicated and non-English articles were removed. The articles were carefully selected to guarantee the literature quality, which is a trade-off for quantity.
With strict literature search and screening processes, it yielded 7 articles from 349 articles of initial literature database. Needed article information was extracted from each article by:
- Direct information including journal, title, authors, abstract, full text documents of candidate studies, publishing year.
- Place name of the study area.
- Study period.
- Research method used.
- Type of kidney-transplantation-immunological- response variables studied.
- Types of COVID-19 vaccine studied.
- The conclusions made about the impacts of related- humoral-immunological-response on kidney- transplanted recipients. An overview of the information required for the present analysis that was captured by those themes was shown in the Figure 1.
Results
| Year of Publication | Author (s) | Methodology & Study Design | Results | References |
|---|---|---|---|---|
| 2023 | Hovd, et al. | Prospective cohorts | Humoral vaccine response increased with additional booster doses. | [11] |
| 2023 | Mahallawi, et al. | Cross- sectional | Serum IgG antibody level seropositivity rate was critically higher than the seronegativity rate in KTRs who received three doses, compared to a single dose or two doses. | [18] |
| 2023 | Graninger, et al. | Prospective cohorts | Serum IgA and IgG seroconversion rates, neutralizing antibodies, and cellular immune response were lowest in KTRs, after two doses of mRNA-COVID-19 vaccination, compared to DPs. Serum TTV loads were also critically lower in KTRs with cellular and humoral immune responses to mRNA-COVID-19 vaccination, compared to non-responders. | [19] |
| 2022 | Benning, et al. | Prospective cohorts | 35 % of KTRs after mRNA-COVID-19 vaccination (at least three doses) revealed anti-spike S1 IgG antibody seroconversion above the predefined cutoff. Serum anti-spike S1 IgG index, % inhibition for serum neutralizing antibodies, and MFI for anti- RBD antibodies before mRNA-COVID-19 vaccination increased from IQRs (medians). | [20] |
Table 1: Demonstrating the cellular and humoral immune response after COVID-19 vaccination in kidney transplant recipients (2021-
2022 de Boer, et al. Prospective cohorts
2022 Tylicki, et al. Longitudinal observational Serum IgG antibody levels were critically higher in EVR-received KTRs, compared to MMF-received KTRs after two doses of mRNA-COVID-19 vaccination. All EVR group (100 % responders) demonstrated higher levels of serum IgG antibodies, compared to the MMF group after the third dose of mRNA-COVID-19 vaccination. Half of MMF group revealed positive T-cell response, whereas EVR group demonstrated 44 %. No association between the presence of serum IgG antibody levels and positive T-cell response (p = 0.807) [21]
PI-KTRs and IN-KTRs demonstrated no differences in the aspects of sex, age, type of immunosuppression, graft vintage, and graft function after the third dose of mRNA-COVID-19 vaccination. 100 % of PI-KTRs and 45.78 % of IN-KTRs revealed immediately positive serum anti-S antibody response after primary mRNA- COVID-19 vaccination with median titers of 1,219 and 365.3 (117.3-915.2) BAU/mL, respectively.
[22]
Serum anti-S1 IgA and IgG responses were substantially diminished in KTRs, 68.2 % and 70.5 %, respectively, compared with DPs and HCs after two mRNA-COVID-19 vaccination. DPs and KTRs demonstrated a typical decrease of absolute B cells with some differences in pre-memory, whereas there was no differences within B-memory-cell compartment after two mRNA- COVID-19 vaccination.
Discussion
Four of seven related-published articles (5.71 %) from 349 published articles of the initial databases demonstrated positive humoral immune responses by increasing serum anti-S1 IgA and IgG levels among the KTRs after booster doses of mRNA-COVID-19 vaccination, particularly the elderly (Table 1) [11, 18, 21, 22], whereas serum TTV loads is a indicator of cellular and humoral immune responses that was critically lower in KTRs with humoral and cellular immune responses [21]. Interestingly, EVR could increase immune responses after two doses of mRNA-COVID-19 vaccination, compared to MMF De-Boer SE, et al. [21] after mRNA-COVID-19 vaccination in KTRs [19]. Both dialysis patients and KTRs demonstrated RBD+-B cell (pre-switch-B and naïve-B cells) enrichment [1].
Mycophinolic acid (MPA) withdrawal prior mRNA- COVID-19 vaccination in KTRs demonstrated critical rising of serum anti-S1- and anti-S2-IgG levels, including post-booster vaccination, in comparison to those who remained on MPA maintenance treatment [20]. One of the seven related- published positive articles revealed humoral immune responses above 5 BAU/mL at 33 days after the 5th booster dose of mRNA-COVID-19 vaccination [11]. KTR survivors with age above 70 years who received a living-donor organ demonstrated lower-COVID-19-risk-related death, compared to KTRs with an-organ-receiving from deceased donor, in addition to higher risk of COVID-19 infection among female KTRs [11].
Interestingly, a recent study demonstrated that viral- vector, and heterogenous of all homogenous mRNA- COVID-19 vaccines revealed reduction of levels of anti-S1 IgG between the first and third serum samples [18]. No differences between serum anti-S1 IgG levels at one and six- months after mRNA-COVID-19 vaccination in KTRs with one- month-post-mRNA-COVID-19-vaccination-IgG-immune- response seropositivity and different factors through linear regression analysis [18]. Among the immunocompromised population, including KTRs, DPs, PDs, at least three doses of mRNA-COVID-19 vaccination was recommended to be the preparation of choice [20, 22].
Conclusion
Withdrawal of the immunosuppressants, such as MPA should withdrawn 5-7 days or dose reduction in KTRs and immunocompromised individuals prior COVID-19 vaccination. Thus, this could be applied in KTRs or immunocompromised persons without previous or present DSA. Finally, at least third dose of mRNA-COVID-19 vaccination should be performed.
- 2021
- Rincon-
- Arevalo, et al.
- Prospective cohorts
Table 2: Demonstrating the cellular and humoral immune response after COVID-19 vaccination in kidney transplant recipients
Authors ‘ Contributions
Dr. Attapon Cheepsattayakorn conducted the study framework and wrote the manuscript. Associate Professor Dr. Ruangrong Cheepsattayakorn and Professor Dr. Porntep Siriwanarangsun contributed to scientific content and assistance in manuscript writing. All authors read and approved the final version of the manuscript.
Competing Interests
The authors declare that they have no actual or potential competing financial interests.
Funding Sources
The authors disclose no funding sources.
References
-
Rincvon-Arevalo H, Choi M, Stefanski AL, Halleck F, Weber U, et al. (2021) Impaired humoral immunity to SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients and dialysis patients. Sci Immunol 6(60): eabj1031.
-
Stumpf J, Siepmann T, Lindner T, Karger C, Schwobel J, et al. (2021) Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients : a prospective, multicenter observational study using mRNA 1273 or BNT162b2 mRNA vaccine. Lancet Reg Health Eur 9: 100178.
-
Chen JJ, Lee TH, Tian YC, Lee CC, Fan PC, et al. (2021) Immunogenicity rates after SARS-CoV-2 vaccination in people with end-stage kidney disease: a systematic review and meta-analysis. JAMA Netw Open 4(10): e2131749.
-
Strengert M, Becker M, Ramos GM, Dulovic A, Gruber J, et al. (2021) Cellular and humoral immunogenicity of a SARS-CoV-2 mRNA vaccine in patients on hemodialysis. EBioMedicine 70: 103524.
-
Stumpf JKA, Mauer R, Steglich A, Gembardt F, Martin H, et al. (2022) Equivalent humoral and cellular immune response but different side effect rates following SARS- CoV-2 vaccination in peritoneal and hemodialysis patients using messenger RNA. Nephrol Dial Transpl 37(4): 796-798.
-
Mulley WR, Le ST, Ives KE (2017) Primary seroresponses to double-dose compared with standard-dose hepatitis B vaccination in patients with chronic kidney disease: a systematic review and meta-analysis. Nephrol Dial Transplant 32(1): 136-143.
-
Liao Z, Xu X, Liang Y, Xiong Y, Chen R, et al. (2016) Effect of a booster dose of influenza vaccine in patients with hemodialysis, peritoneal dialysis and renal transplant recipients: a systematic literature review and meta- analysis. Hum Vaccin Immunother 12(11): 2909-2915.
-
Syed-Ahmed M, Narayanan M (2019) Immune dysfunction and risk of infection in chronic kidney disease. Adv Chronic Kidney Dis 26(1): 8-15.
-
Kato S, Chmielewski M, Honda H, Pecoits-Filho R, Matsuo S, et al. (2008) Aspects of immune dysfunction in end- stage renal disease. Clin J Am Soc Nephrol 3(5): 1526- 1533.
-
Betjes MGH (2013) Immune cell dysfunction and inflammation in end-stage renal disease. Nat Rev Nephrol 9(5): 255-265.
-
Hovd M, Asberg A, Munthe LA, Heldal K, Reisaeter AV, et al. (2023) Humoral vaccine response and breakthrough infections in kidney transplant recipients during the COVID-19 pandemic: a nationwide cohort study. Lancet 60: 102035.
-
Nimmo A, Gardiner D, Ushiro-Lumb I, Ravanan R, Forsythe JLR (2022) The global impact of COVID-19 on solid organ transplantation: two years into a pandemic. Transplantation 106(7): 1312-1329.
-
Midtvedt K, Vaag JT, Heldal K, Munthe LA, Lund-Johansen F, et al. (2022) Fourth dose of the SARS-CoV-2 vaccine in kidney transplant recipients with previously impaired humoral antibody response. Am J Transplant 22(11): 2704-2706.
-
Kamar N, Abravanel F, Marion O, Romieu-Mourez R, Couat C, et al. (2021) Assessment of 4 doses of SARS-CoV-2 messenger RNA-based vaccine in recipients of a solid organ transplant. JAMA Netw Open 4(11): e2136030.
-
Boyarski BJ, Barbur I, Chiang TP, Ou MT, Greenberg RS, et al. (2021) SARS-CoV-2 messenger RNA vaccine immunogenicity in solid organ transplant recipients with prior COVID-19. Transplantation 105(11): e270-e271.
-
Hall VG, Ferreira VH, Ku T, Ierullo M, Majchrzak-Kita B, et al. (2021) Randomized trial of a third dose of mRNA- 1273 vaccine in transplant recipients. N Engl J Med 385(13): 1244-1246.
-
Sakuraba A, Luna A, Micic D (2022) A systematic review and meta-analysis of serologic response following coronavirus disease 2019 (COVID-19) vaccination in solid organ transplant recipients. Viruses 14(8): 1822.
-
Mahallawi WH, Alharbi WA, Aloufi SA, Ibrahim NA, Abdelrahman MM, et al. (2023) Decline humoral immunity of kidney transplant recipients to SARS-CoV-2 vaccines. Infection and Drug Resistance 16: 2829-2840.
-
Graninger M, Stumpf J, Bond G, Görzer I, Springer DN, et al. (2023) Prediction of humoral and cellular immune response to COVID-19 mRNA vaccination by TTV load in kidney transplant recipients and hemodialysis patients. Journal of Clinical Virology 162: 105428.
-
Benning L, Morath C, Kühn T, Bartenschlager M, Kim H, Beimler J, et al. (2022) Humoral response to SARS-CoV-2 mRNA vaccination in previous non-responder kidney transplant recipients after short-term withdrawal of mycophenolic acid. Frontiers in Medicine 9: 958293.
-
De-Boer SE, Berger SP, Leer-Buter CCV, Kroesen B, Baarle DV, et al. (2022) Enhanced humoral immune response after COVID-19 vaccination in elderly kidney transplant recipients on everonimus versus mycophenolate mofetil-containing immunosuppressive regimens. Transplantation 106(8): 1615-1621.
-
Tylicki L, Debska-Slizien A, Muchlado M, Slizzien Z, Golebiewska J, et al. (2021) Boosting humoral immunity from mRNA COVID-19 vaccines in kidney transplant recipients. Vaccines 10(1): 56.
- Bedside Pulmonary Rehabilitation – Mandatory and Cost- Effective Tools
- The Role of Chest Radiology in Traumatic Injuries: A Comprehensive Narrative Review
- Pseudosepsis in Acute Inflammation of the Lung
- An Overview of Lung Injury in Covid-19: Evaluating the Impact of Re-Exposure and Emerging Variants
- Fibreoptic Bronchoscopy-its Role in Pulmonary Medicine-Current Trends in Intensive Care Unit
- Retrospective Study on the Efficacy of Homoeopathic Medicines in the Treatment of Acute Rhinitis