Confirmation of Tb: Salvation of an Elderly Heavy Smoker with Lower Lung Mass
Pulmonary Tuberculosis (PTB) remains one of the major health problems throughout the world. It has variable presentations such as consolidation, pleural effusion, mediastinal lymphadenopathy, miliary pattern and may also present rarely as a mass lesion. Here we are reporting such a rare case presenting with dry cough along with intermittent fever and significant weight loss for 2 months and chest pain for 1 month. A mass lesion was noted in the right lower zone on chest x-ray and confirmed by Computed Tomography (CT) scan. Ultrasound-guided trans-thoracic biopsy confirmed tuberculosis and responded to Anti Tubercular Therapy (ATT).
Introduction
Tuberculosis (TB) is one of the major global health problem, which is responsible for ill-health among millions of people every year. In 2019, an estimated 10 million people developed TB and 1.4 million died from the disease and PTB remains one of the top 10 causes of death worldwide. It is the leading cause of death from a single infectious agent [1]. There are many similarities between PTB and lung cancer presenting as a mass lesion, both are very common, have high prevalence, involve lung parenchyma, and above all, are characterized by similar symptoms [2]. PTB is infectious while lung cancer is a non-infectious disease. There are differences between these two entities as they have different etiologies. Several symptoms such as fever, cough, expectoration, hemoptysis, anorexia, and weight loss are common to both lung cancer and TB [3]. PTB can also present as mass-like lung opacity in asymptomatic patients whose sputum smears or cultures may be negative for mycobacteria [4]. PTB is one of the most common benign lesions that require differentiation from lung cancer [5].
A 61-year-old male patient, a former smoker, presented with history of persistent dry cough, intermittent fever, and significant weight loss for 2 months, and chest pain for 1 month. He had 30-pack-year smoking history and denied history of chills, night sweats, hemoptysis, and dyspnea. The cough and fever did not resolve with antibiotics. No history of tuberculosis in the past, not a known diabetic or hypertensive. Bowel and bladder habits are regular.
No pallor, no icterus, no cyanosis, no clubbing and no generalized lymphadenopathy was seen on general examination. On inspection chest wall moments were symmetrical on both sides, vocal fremitus was decreased on the right infra scapular area. On percussion dull note was noted in the right infra scapular area. Absent breath sounds were noted in the right infra scapular area. Vocal resonance decreased on the right infra scapular area.
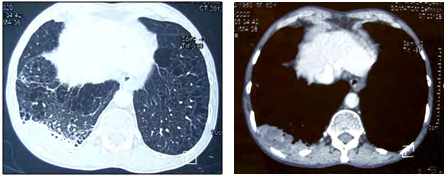
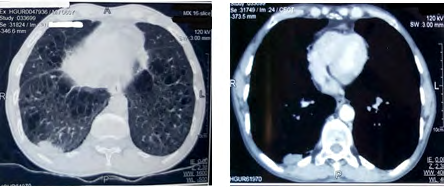
Chest x-ray PA view (Figure 1) showed a mass lesion of approximately 3x4cm in right lower zone. Contrast enhanced Computed Tomography (CECT) of the lungs showed sub-pleural 3.2x 4.7 cm mass with smooth margins, in the right lower lobe, without calcification and cavitation abutting to the chest wall and also showed diffuse paraseptal and centriacinar emphysematous changes in bilateral lungs (Figure 2). No pleural effusion or mediastinal lymphadenopathy was noted. Transthoracic biopsy under ultrasound guidance was done and HPE revealed granulomas with epitheloid cells, multinucleate giant cells, and caseating necrosis suggestive of tuberculosis. The patient was started on ATT (H/R/Z/E) and started responding well to ATT (Figures 1b & 3).
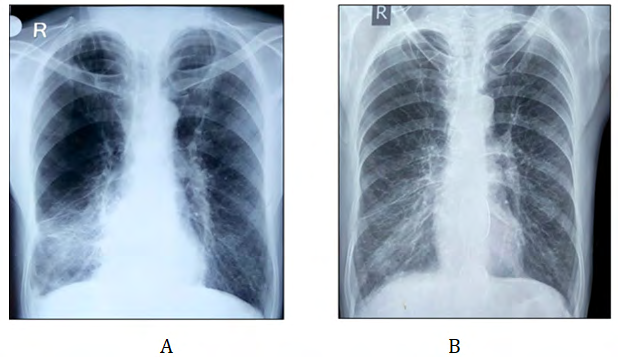
Figure 1a & 1b: Chest X –ray showing Right lower lobe infiltrates and hyperinflation & Chest X- ray Showing response to ATT
Discussion
Mycobacterium tuberculosis is the causative organism of tuberculosis. It typically affects the lungs (pulmonary TB) and mostly manifests as upper lobe cavitary lesions. Certain overlapping symptoms like cough, expectoration, fever, weight loss, hemoptysis, and breathlessness are common for both lung cancer and pulmonary tuberculosis. However, careful history and examination can help the clinician to suspect Tuberculosis [6].
Hadlock, et al. indicated that atypical manifestations of TB (excluding the primary TB pattern in adults) are prevalent in nearly 8% of cases [7]. However, recent studies have suggested that unusual radiographic manifestations are seen in as many as one-third of adult-onset TB cases, which may seriously delay treatment. Confined to the basal segments of lower lobes, the right middle lobe or lingular, or the anterior segment of an upper lobe is considered as uncommon presentation in post primary tuberculosis and also it can manifest as a mass-like density that mimics carcinoma, tuberculoma, or reversible multiple cysts [8, 9, 10]. PTB can manifest as a mass lesion in the upper lobes in 7% of cases but mass presenting in the lower lobe is unusual. Tuberculosis accounted for 27% of all infections, initially presumed to be lung mass on imaging [11]. The involvement of the lower lobe is more common in diabetic patients and immunocompromised patients [12].
Pulmonary TB is one of the most common benign lesions that require differentiation from lung cancer [13]. Due to the overlapping features of tuberculomas and peripheral lung cancer, PTNB (Percutaneous transthoracic needle biopsy) should be performed to confirm the diagnosis [14]. Ultrasound is useful in locating mass lesions and visualization of co-existing pleural effusion and pneumothorax and pleural nodules [15]. We did an ultrasound-aided transthoracic biopsy for this case and confirmed our diagnosis of TB. The patient received ATT and responded to the therapy very well as is obvious from follow-up radiography. He is well at present and has no symptoms. Our case is unusual also because of the patient’s case profile which almost certainly indicated Lung Cancer such as advanced age, heavy smoking history and the radiological findings. It can be said that the diagnosis of PTB was almost a salvation for the patient because the alternative would have been much more inimical for his health and survival.
Conclusion
To infer, TB can also manifest as a mass-like density that resembles lung cancer. The main delay in diagnosis and treatment is patients’ ignorance in reporting to general practitioners &possible misinterpretation of chest radiograph findings especially in context of advanced age and history of smoking. Distinguishing between lung cancer and TB remains a challenge, as TB has been misdiagnosed as lung cancer and vice versa in many cases which can have disastrous consequences. Establishing an accurate early diagnosis can decrease the likelihood of disease progression and further complications. One should always think of tuberculosis in the differential diagnosis until proven otherwise; regardless of the thoracic imaging and clinical history, especially in an endemic country like India.
References
-
WHO TB Report (2020) Global Tuberculosis Report 2020.
-
Cherian MJ, Dahniya MH, Marzouk AN, Osmanagich E, Abul A, et al. (1998) Primary pulmonary tuberculosis presenting as mass lesions and simulating tumours in children. Australas Radiol 42(4): 309-312.
-
Cherian MJ, Dahniya MH, Marzouk ANF, Abel A, Bader S, et al. (1998) Pulmonary tuberculosis presenting as mass lesions and simulating neoplasms in adults. Australas Radiol 42(4): 303-308.
-
Ferreirós J, Bustos A, Merino S, Castro E, Dorao M, et al. (1999) Transthoracic needle aspiration biopsy: value in the diagnosis of mycobacte¬rial lung opacities. J Thorac Imaging 14(4): 194-200.
-
Zwirewich CV, Vedal S, Miller RR, Müller NL (1991) Solitary pulmonary nodule: high-resolution CT and radiologic-pathologic correlation. Radiology 179(2): 469-476.
-
Fishman AF, Elias JA, Grippi MA, Fishman JA, Robert M, et al. (2008) Fishman’s pulmonary diseases and disorders.
-
Hadlock FP, Park SK, Awe RJ, Rivera M (1980) Unusual radiographic findings in adult pulmonary tuberculosis. AJR Am J Roentgenol 134(5): 1015-1018.
-
Miller WT, MacGregor RR (1978) Tuberculosis: Frequency of unusual radiographic findings. AJR Am J Roentgenol 130(5): 867-875.
-
Lee KS, Song KS, Lim TH, Kim PN, Kim IY, et al. (1993) Adult-onset pulmonary tuberculosis: findings on chest radiographs and CT scans. AJR Am J Roentgenol 160 (4): 753-758.
-
Palmer PE (1979) Pulmonary tuberculosis-usual and unusual radiographic pre-sentations. Semin Roentgenol 14(3): 204-243.
-
Rolston KV, Rodriguez S, Dholakia N, Whimbey E, Raad I, et al. (1997) Pulmonary infections mimicking cancer: a retrospective, three year review. Support Care Cancer 5(2): 90-93.
-
Segarra F, Sherman DS, Aguero AJ (1963) Lower lung field tuberculosis. Am Rev Respir Dis 87: 37-40.
-
Murayama S, Murakami J, Hashimoto S, Torii Y, Masuda K, et al. (1995) Noncalcified pulmonary tuberculomas: CT enhancement patterns with histological correlation. J Thorac Imaging 10(2): 91-95.
-
Thiessen R, Seely JM, Matzinger FR, Agarwal P, Burns KL, et al. (2007) Necrotizing granuloma of the lung: imaging characteristics and imaging-guided diagnosis. AJR Am J Roentgenol 189(6): 1397-1401.
-
Kim Y, Goo JM, KIm HY, Song JW, Im J, et al. (2001) Coexisting bronchogenic carcinoma and pulmonary tuberculosis in the same lobe: radiologic findings and clinical significance. Korean J Radiol 2(3): 138-144.
- Bedside Pulmonary Rehabilitation – Mandatory and Cost- Effective Tools
- The Role of Chest Radiology in Traumatic Injuries: A Comprehensive Narrative Review
- Pseudosepsis in Acute Inflammation of the Lung
- An Overview of Lung Injury in Covid-19: Evaluating the Impact of Re-Exposure and Emerging Variants
- Fibreoptic Bronchoscopy-its Role in Pulmonary Medicine-Current Trends in Intensive Care Unit
- Retrospective Study on the Efficacy of Homoeopathic Medicines in the Treatment of Acute Rhinitis