Post-ARDS Pulmonary Manifestations in COVID-19 Patients: Assessment of Risk Factors and Treatment Approaches
Background: Mixed radiological pulmonary manifestations with persistent and even progressive dyspnea are the possible consequences of COVID-19 and ARDS and the most worrying long-term complications. Such patients are at high risk for pulmonary fibrosis and non-reversible lung dys-function. The aim of this study was the assessment of risk factors and possible approaches to the treatment of such residual complications in COVID-19 and ARDS patients. Methods: Our study was randomized and controlled. Ninety seven patients were assessed at pul-monary and critical care departments of University Hospital, Baku city 6 weeks after discharge from COVID-19 hospitals. All patients have been treated in ICU for acute respiratory distress syndrome (ARDS) related to severe COVID-19 infection. All patients had persistent, nonimproving symptoms, particularly dyspnea. Depending on residual fibrotic and non-fibrotic changes in lungs all patients have been divided in two groups: 1) 39 patients with lung involvement (50-75%); 2) 58 patients with lung involvement more than 75%. Results: At 6 weeks after discharge all patients reported persistent symptoms: dyspnea 100,0% (97/97), cough 42,3% (41/97), chest pain 51,5% (50/97), fever 29,0% (28/97) and hemoptysis 18,5% (18/97) were assessed. Pulmonary abnormalities were found in all subjects; however, most intensive abnormalities were noticed in intubated patients with severe ARDS (OR 3,75[0,91-8,44] 95% CI; p﹤0,001). In all patients persistent lung function impairment were evaluated. Severity of lung function deficiency was depending on severity of ARDS (p﹤0,001). Follow-up CT chest was done following negative PCR result after 12 weeks to assess degree of recovery and residual fibrotic and non-fibrotic changes. Pulmonary fibrosis has been seen in all patients with lung involvement more than 75% (OR 2,45 [0,81-6,29] 95% CI; p﹤0,001), and organ-izing pneumonia although seen commonly in patients with massive lung involvement (OR 4,24 [0,94-9,26] 95% CI; p﹤0,001). Traction bronchiectasis was higher in patients with massive lung involvement compared to non-massive (OR 2,11 [0,72-5,01] 95% CI; p﹤0,004). CT chest finding like ground glass opacities, consolidation, vascular and bronchial thickening were similar in both group patients (p﹥0,05). Lack of use dexamethasone in acute phase of the disease was higher in patients with lung involvement more than 75% (p﹤0,004) and lack of use prone position ventilation also was one of risk factors for excessive lung involvement (p﹤0,01). Invasive mechanical ventilation incidence was higher in massive lung involvement ((OR 2,84 [0,76-6,44] 95% CI; p﹤0,002). Lack of use HFNC also was associated with higher incidence of more massive lung involvement and development of pulmonary fibrosis (p﹤0,01) and organizing pneumonia (p﹤0,001). Conclusions: Following post-ARDS COVID-19 disease the patients have significant residual radiological inflammatory lung disease, persistent ventilation and functional deficit. There were several risk factors associated with more severe lung fibrotic and non-fibrotic residual changes. Treatment with corticosteroids at the time of ICU admission associated with decrease of extensity of radiological changes and functional impairment.
Introduction
Lung damage is a predominant feature of acute SARS- CoV-2 infection and the incidence of acute respiratory distress syndrome (ARDS) with ICU admission is significantly higher compared to other viral infections [1]. COVID-19 sequelae may range from mild form of fatigue to serious forms requiring long-term oxygen therapy or even lung transplantation owing to pulmonary fibrosis [2]. COVID-19 leads to a broad variety of respiratory diseases with high occurrence of ARDS [3].
The load of fibrotic and non-fibrotic pulmonary changes following SARS-CoV-2 related to ARDS likely to be high; thus, the global burden of fibrosis pulmonary and interstitial lung disease will be increasing significantly [4]. About 150 million people have already been affected by COVID-19 in the course of this pandemic, and about 15% will get a severe COVID-19 pneumonia, 5% will progress to ARDS, meaning that almost 7.5 million will have severe pulmonary involve- ment. As known patients with ARDS most likely will suffer residual sequelae [5]. Although till now the risk factors for post-ARDS fibrotic and non-fibrotic changes and proven treatment of post-ARDS residual pulmonary changes are not completely evaluated. The aim of this study is the evaluation of risk factors for clinically significant residual fibrotic and non-fibrotic changes and the use of anti-inflammatory drugs in post-ARDS COVID-19 patients.
Methods
This was a single-center prospective observational study of patients with a diagnosis of SARS-CoV-2 related to ARDS 6 weeks after discharge from ICU. 97 patients including 58 males (60%) and 39 females (40%) with age range from 50 to 80 years old (mean age 65,4 years) were enrolled in this study in University Hospital of Baku, Azerbaijan, during the period from 10 September 2020 to 30 April 2021. All patients were with ongoing symptoms, subjected to full clinical history and underwent structured assessment by chest CT scan. All examinations and follow-up CT scans are represented for every patient. The distribution features such as ground glass opacity (GGO), consolidation, interstitial thickening, bronchiectasis, ‘crazy paving’, air bronchogram, irregular interface, coarse reticular pattern, parenchymal band, lymphadenopathy, pleural effusion and cystic changes as well as the involving lung lobes were recorded. The main analysis criteria were the number of affected lung lobes. The presence of GGO, consolidation, interstitial thickening, fibrosis and air cyst were analyzed quantitatively using a radiologic scoring system ranging from 0 to 25 points. There were 5 lung lobes and each was evaluated 0-5 points on the basis of the area involved. In our study post-ARDS fibrotic and non-fibrotic residual pulmonary changes was 4 point, where the area of involving was 50-75%. Individual segmental scores were added together as a total score in the statistical analysis. Pulmonary function tests were performed by technicians in the pulmonary function laboratory of University Hospital. Spirometry and pulmonary diffusion capacity test was per- formed using spirometry and body plethismography and the procedure was followed by the ATS-ERS guidelines [6, 7]. The following parameters were measured: forced vital capacity (FVC), forced expiratory capacity at the 1st second of exhalation (FEV₁), total lung capacity (TLC), and diffusion capacity of the lung for carbon monoxide (DLCO) measured by means of the single-breath test. All pulmonary function test measurements were expressed as percentages of predicted normal valves. Diffusion deficit was considered as DLCO﹤80% of predicted value.
Continuous variables were described using mean with standard deviation (SD) or median with interquartile range (IQR), followed by unpaired t-test or Mann-Whitney test. Categorical variables were described as percentage and compared using the Chisquare test. Logistic regression analysis was used to study independent CT abnormalities and abnormal pulmonary function. The conventional level of statistical significance of 0,05 was used for all analyses.
Results
Ninety seven ARDS COVID-19 survivors completed the study. Their mean (SD) age was 65,4 (50-80), among which 40% were female. 81 patients (83,5%) had underlying co-morbidities, while 62 patients (63,9%) had 2 or more comorbidities.
| Characteristics | 50-75% Lung Involvement (N=39) | ﹥75% Lung Involvement (N=58) | Value |
|---|---|---|---|
| Age, years | 52,4 ±10,2 | 68,2 ± 12,1 | ﹤0,001 |
| Male | 23 (59,0%) | 35 (60,3%) | 0,421 |
| Female | 16 (41,0%) | 23 (39,6%) | 0,428 |
| BMI | 28,4 ± 3,5 | 27,9 ± 4,1 | 0,614 |
| Comorbidities (%) | 26 (66,6%) | 55 (94,8%) | ﹤0,01 |
| Ongoing symptoms (%) | |||
| Median dyspnea | 3,00 (1-4) | 4,00 (2-5) | ﹤0,001 |
| Exertional dyspnea | 39 (100,0) | 58 (100,0) | - |
| Non-exertional dyspnea | 9 (23,1) | 43 (74,1) | ﹤0,001 |
| Cough | |||
| Fever | 10 (25,6) | 31 (53,4) | ﹤0,05 |
| Chest pain | 12 (30,8) | 38 (65,5) | ﹤0,01 |
| Hemoptysis | 3 (7,6) | 15 (25,9) | ﹤0,05 |
| Pulmonary function, SD | |||
| FEV₁ | 72,5 ± 12,4 | 61,8 ± 11,6 | ﹤0,01 |
| FVC | 64,7 ± 10,6 | 46,3 ± 11,9 | ﹤0,001 |
| TLC | 71,8 ± 14,5 | 53,7 ± 13,8 | ﹤0,05 |
| DLCO, SD | 70,4 ± 8,4 | 54,6 ± 9,3 | ﹤0,01 |
| Mean PAP, SD | 18,2 ± 6,9 | 23,4 ± 6,7 | ﹤0,05 |
| CT abnormalities, n% | |||
| GGO | 31 (79,5) | 16 (27,6) | ﹤0,002 |
| Fibrosis | 21 (53,8) | 58 (100,0) | ﹤0,01 |
| Traction bronchiectasis | 14 (35,8) | 47 (81,0) | ﹤0,004 |
| Organizing pneumonia | 11 (28,2) | 51 (87,9) | ﹤0,001 |
| Cystic changes | 8 (20,5) | 40 (68,9) | ﹤0,001 |
| Reticular pattern | 23 (39,6) | 5 (87,9) | ﹤0,005 |
| Lack of use dexamethasone, n% | 11 (26,9) | 39 (67,2) | ﹤0,004 |
| Lack of use HFNC, n% | 9 (23,1) | 28 (48,2) | ﹤0,01 |
| Lack of prone position ventilation, n% | 8 (20,5) | 26 (44,8) | ﹤0,01 |
| Intubation, n% | 11 (28,2) | 45 (77,6) | ﹤0,002 |
Table 1: Baseline characteristics of patients with post-ARDS lung disease following infection with SARS-CoV-2 (n=97).
Patients with abnormal CT more than 75% lung involvement were significantly older (68,9 ± 12,1 vs 52,4 ± 10,2; p ﹤0,001). There were differences in gender and male gender was more sensitive to massive lung abnormalities ( ﹤0,05). Comorbidities commonly were occurred in patients group with massive residual lung abnormalities (94,8% vs 66,6%; p﹤0,01). All patients with abnormal residual CT findings were admitted with dyspnea and the incidence of exertional dyspnea was same in both group, however, non exertional (dyspnea at rest) and severe dyspnea was higher in patients group with massive residual lung CT abnormalities (74,1% vs 23,1%; p ﹤0,001). Cough was common in patients with massive lung involvement compared to non-massive CT abnormalities (53,4% vs 25,6%; p ﹤0,05) and fever most common has been found in patients with massive CT abnormalities (OR 4,01 [0, 21] 95% CI; p ﹤0,001) and was common in patients with secondary infection (bacterial and fungal). Chest pain as sign of pleural involvement (pleural thickening and bands) was common finding in patients with more massive lung abnormalities (OR 2,24 [0, 61] 95% CI; p ﹤0,01). Hemoptysis frequently was ongoing in patients group with more massive lung involvement (25,9% vs 7,6%; p ﹤0,05). Interestingly that the incidence of hemoptysis was higher in patients with cystic changes where possibility the colonization of Aspergillus fumigatus and in patients with overuse of the antibiotics in acute phase of COVID-19 infection.
Spirometry was completed in all patients. The lung function abnormalities were detected in all patients with respiratory symptoms (100%). However, more severe lung function impairment was detected in patients with more massive residual lung abnormalities in lung CT scan. Forced vital capacity was significantly lower compared to non-massive lung involvement (46,3 ± 11,9 vs 64,7 ﹤0,05 10,6; p﹤0,001) and total lung capacity although was lower ( 53,7 ± 13,8 vs 71,8 ± 14,5; p﹤0,05). Massive residual lung abnormalities were associated with markedly decrease of diffusing capacity of the lung for carbon monoxide (DLCO) and was 54,6 ± 9,3 (p ﹤0,01). Mean pulmonary artery pressure (mPAP) was higher in patients group with massive residual lung involvement (23,4 ± 6,7 vs 18,2 ±6,9; p ﹤0,05). All patients showed bilateral involvement on chest HRCT scan. GGO was the commonest in patients group with non- massive residual lung CT abnormalities (OR 2,92 [0, 78] 95% CI; p﹤0,002) (Table 2)
| OR (95% CI) | P value | |
|---|---|---|
| Ground glass opacities | 2,56 (0,81-6,14) | < 0,002 |
| Fibrosis | 1,98 (0,72-4,12) | < 0,01 |
| Organizing pneumonia | 2,92 (0,94-7,21) | < 0,001 |
| Cystic changes | 3,25 (0,84-7,28) | < 0,001 |
| Traction bronchiectasis | 2,65 (0,79-6,48) | < 0,004 |
| Reticular pattern | 2,21 (0,69-5,76) | < 0,005 |
Table 2: Logistic regression analysis for lung CT abnormalities.
In contvary to GGO as residual abnormality the incidence of fibrosis was more significant in patients with massive CT abnormalities (OR 1,98 [0, 12] 95% CI; p ﹤0,01). Organizing pneumonia as residual CT abnormality after severe ARDS was common in patients group with massive CT abnormalities (OR 2,92 [0, 21] 95% CI; p﹤0,001). Cystic changes also was the commonest in patients with massive CT abnormalities (OR 3,2 [0, 28] 95% CI;
p﹤0,001). Traction bronchiectasis as result of lung fibrosis was occurred commonly in patients with massive residual lung abnormalities (OR 2,65 [0, 48] 95% CI; p﹤0,004).
There were several laboratory abnormalities which were associated with development of more massive residual lung abnormalities (Table 3).
| Lung Involvement 50-75% (N=39) | Lung Involvement > 75% (N=58) | P value | |
|---|---|---|---|
| PaO2 (mm Hg) | 60,8 (54,7-68,2) | 54,3 (49,4-61,3) | < 0,01 |
| PaCO2 (mm Hg) | 38,0 (35,1-41,7) | 43,4 (36,2-51,7) | < 0,01 |
| pH | 7,39 (7,34-7,44) | 7,36 (7,30-7,39) | < 0,05 |
| Lymphocyte count (x109/L) | 1,4 (0,99-1,7) | 1,45 (1,09-1,79) | 0,671 |
| Albumin, g\l | 43,61 ± 3,76 | 39,16 ± 3,38 | 0,006 |
| Urea nitrogen, mmol/l | 4,81 (3,13-5,12) | 5,72 (3,96-6,34) | 0,001 |
| CRP, mg\l | 8,04 (0,76-21,42) | 25,81 (3,24-39,72) | 0,01 |
| D-dimer, mg\l | 5,2 ± 1,6 | 11,2 ± 1,4 | 0,006 |
| Bacterial infection (n/%) | 5 (12,8) | 23 (39,7) | 0,026 |
| Fungal infection (n/%) | 3 (7,7) | 18 (31,0) | 0,035 |
Table 3: Differences in laboratory findings in patients with COVID-19 related to post-ARDS lung abnormalities.
Admission valves of arterial blood gas analysis results were significantly lower in patients group with massive residual CT abnormalities (p﹤0,01). Compared with non- massive CT abnormalities patients on admission, survivors with massive CT abnormalities after ARDS had lower albumin level (43,61 ± 3,76 vs 39,16 ±3,38; p=0,006), higher urea nitrogen level (4,81 [3, 12] vs 5,72 [3, 34]; p=0,001), higher CRP level (8,04 [0, 42] vs 25,81 [3, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 72]; p=0,01), and higher D-dimer level (5,2 ± 1,6 vs 11,2 ± 1,4; p=0,006).
Bacterial infection, particularly multi-drug resistant pathogens were common finding in patients with massive CT abnormalities (5 [12, 8] vs 23 [39, 7]; p=0,026) and fungal infection, particularly Aspergillus fumigatus was common in patients with massive lung CT abnormalities (3 [7, 7] vs 18 [31, 0]; p=0,035) and frequently was occurred in patients with cystic CT abnormalities. And frequent symptom for such patients was hemoptysis. In our study the most interesting finding was the association of D-dimer high level with lower level of lung function (Figure 1).
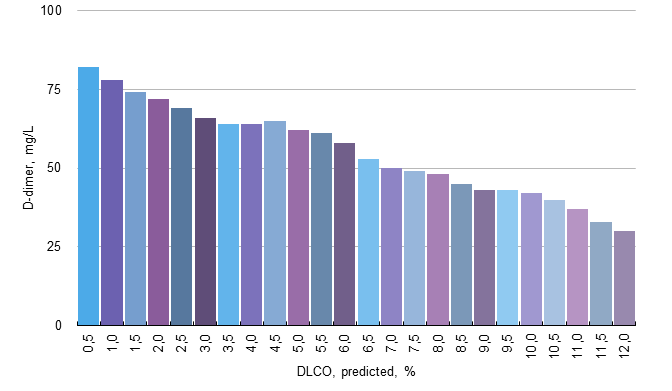
This results indicated that the survivors after COVID-19 related to ARDS still has significant im-paired lung function six weeks after discharge, and D-dimer as biomarker of fibrotic changes in lungs might be a potential biomarker to predict DLCO of these patients. Ninety seven patients completed treatment and follow-up with clinical review, CT scan, and pulmonary function tests. All 97 patients report that their breathlessness had significantly improved following treatment with methylprednisolone (40 mg), and median MRC had improved from 3,00 (± 1) to 2 (± 1) in patients with non-massive CT abnormalities, from 4,00 (± 1) to 3 (± 1) in patients with massive CT abnormalities (Table 4).
| Before treatment | After treatment | P valve | |
|---|---|---|---|
| Median MRC | 4,00 (±1) | 3,00 (±1) | 0,002 |
| FVC, % | 46,3 ± 11,9 | 57,8 ± 12,6 | 0,005 |
| DLCO, % | 54,6 ± 9,3 | 70,8 ± 10,9 | 0,003 |
| Mean PAP | 23,4 ± 6,7 | 17,2 ± 6,9 | 0,004 |
Table 4: Follow-up data from patients with massive lung CT abnormalities after COVID-19 related to ARDS (n=58).
This was associated with a mean relative increase in FVC (± 11,5) at 4 week, and the mean increase in DLCO was (±16,2), which reached statistical significance. Mean pulmonary arterial pressure decrease significantly and to the end of treatment period was 17,2 ±6,9 mm Hg (-6,2; p = 0,004). At the same time improvement in clinical features and lung function on steroid therapy was accompanied with improvement of CT features, and repeat CT imaging demonstrated resolution of the more solid components, decreased density and extension of ground glass pattern and consolidation after treatment. At 4 weeks follow-up imaging, we did not observe the progression of inflammatory change to any fibrosis.
Discussion
Here we describe characteristics of large cohort of patients surviving after ICU admission with COVID-19 related to ARDS, who had residual massive and non-massive pulmonary disease at 6 weeks after discharge.
Ninety seven patients had persistent residual CT abnormalities suggestive of organizing pneumonia, ground- glass pattern and were treated with oral methylprednisolone [8]. The objective was to evaluate risk factors for lung abnormalities post-ARDS related to COVID-19 infection and to prevent the further progression of pulmonary fibrosis with permanent functional impairment [9, 10].
A cohort of patients were identified who had massive and sub-massive radiological inflammatory lung disease (of organizing pneumonia and ground-glass pattern types) and persistent physiological and functional deficit at 6 weeks. As shown in (Table 1) patients who survived fro post-ARDS elated to COVID-19 might have persistent lung damage and long-term pulmonary functions impairment. Clinically patients with abnormal HRCT scans were generally older than those with normal chest HRCT score, which implied that higher chest radiological scores were mostly obtained in elder patients (8,9). In our study all patients have administrated to hospital with chest CT scan abnormalities, however, more massive residual (﹥75%) CT abnormalities have been occurred in elderly patients (﹤0,001) interestingly, in patients with the massive residual CT abnormalities most commonly have noticed in male compared to female (p=0,041). Comorbidities were common findings in patients group with massive CT abnormalities (p﹤0,05) and this finding was not presented in reference. Most intensive ongoing symptoms (dyspnea) were also common in patients with massive residual CT changes compared non-massive residual CT changes (p﹤0,001).
Patients with more massive residual abnormal lung CT changes had common intubation rate (p﹤0,002) and in this group patients dexamethasone at acute phase of COVID-19 infection was used less common (p﹤0,004). These findings also we have not found as result of reference analysis. Additionally, it was found that the level of urea nitrogen, CRP and D-dimer indicated multi-organ damage caused by COVID-19 and triggered deteriorations to general functions which was similar to other reports [6, 11, 12]. At 6 weeks after discharge residual abnormalities of pulmonary function were observed in all (100,0%) of the cohort, mostly demonstrated diffusion reductions in DLCO. However, the extensity of residual radiological abnormalities were associated with more significantly decreased pulmonary function and impaired diffusing capacity of the lung (DLCO). In the following-up studies for the patients rehabilitated from ARDS, impaired lung function could last for month or even years [13].
D-dimer elevation has reported as an important laboratory finding noted in COVID-19 patients which requires additional attention. Several studies have reported that D-dimer on admission was the independent predictor of in-hospital death for patients with COVID-19 [14, 15]. We also found that the level of D-dimer was an important prognostic factor for abnormal DLCO, and more high level of it was associated with lower level of DLCO.
Our other important finding was the significantly improvement of lung function and extensive of residual CT abnormalities in lung tissue under impact low doses of methylprednisolone. Most important finding was the markedly improvement of lung function and reduction of CT abnormalities in patients group with massive residual radiological changes.
However, there were several limitations in this study. Firstly, only 97 patients with confirmed SARS-CoV-2 infection related to post-ARDS patients were enrolled in this study. Larger sample size would be more ideal for the study. Secondly, since the patients included in this study were heterogeneous and small part of patients were critical, related to their massive residual lung CT abnormalities and significantly lower lung function and respiratory failure, and non-critical. And as known the value of pulmonary function test and HRCT scanning in critical patients need to be assessed. In our study we didn’t conduct the objective measurements of lung function status such as exercise lung function test or 6-minute walk test.
In summary, this research has demonstrated that the significant radiographic and physiological abnormalities still existed in all COVID-19 related to post-ARDs patients six weeks after dis-charge. There were several risk factors which highly associated with massive (﹥75% lung involvement) residual lung CT abnormalities, and some of them were associated with more significant lung function impairment. Appropriate management of such patients with low doses of corticosteroids may play important role in reduction of residual lung CT abnormalities and improvement of lung function.
References
-
Zhao W, Zhong Z, Xie X, Yu Q, Liu J, et al. (2020) Relation between chest CT findings and clinical condi-tions of coronavirus disease (COVID-19) pneumonia: a multi center study. AJR Am J Roentgenol 214(5): 1072-1077.
-
Bradley BT, Maioli H, Johnston R, Chaudhry I, Fink SL, et al. (2020) Histopathology and ultra-structural findings of fatal COVID-19 infections in Washington State: a case series. Lancet 396: 320-332.
-
Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, RECOVERY Collaborative Group, et al. (2020) Dexamethasone in hospitalized patients with covid-19. N Engl J Med 384(8): 693-704.
-
Sterne JAC, Murthy S, Diaz JV, Slutsky AS, Villar J, WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group, et al. (2020) Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: a meta-analysis. JAMA 324(13): 1330-1341.
-
George PM, Barratt SL, Condliffe R, Desai SR, Devaraj A, et al. (2020) Respiratory follow-up of patients with COVID-19 pneumonia. Thorax 75(11): 1009-1016.
-
Hui DS, Joynt GM, Wong KT, Gomersall CD, Li TS, et al. (2005) Impact of severe acute respiratory syndrome (SARS) on pulmonary function, functional capacity and quality of life in cohort of survivors. Thorax 60(5): 401- 409.
-
Zhang P, Li J, Liu H, Han N, Ju J, et al. (2020) Long-term bone and lung consequences associated with hospital- acquired severe acute respiratory syndrome: 1 15-year follow-up from a prospective cohort study. Bone Res 8: 34.
-
Matthay MA, Pittet JF, Jayr C (1998) Just say NO to inhaled nitric oxide for the acute respiratory distress syndrome. Crit Care Med 26(1): 1-2.
-
Wilcox ME, Patsios D, Murphy G, Kudlow P, Paul N, et al. (2013) Radiologic outcomes at 5 years after severe ARDS. Chest 143(4): 920-926.
-
Antonio GE, Wong KT, Hui DS, Wu A, Lee N, et al. (2003) Thin-section CT in patients with severe acute respiratory syndrome following hospital discharge: preliminary experience. Radiology 228(3): 810-815.
-
Hui DS, Wong KT, Ko FW, Tam LS, Chan DP, et al. (2005) The 1-year impact of severe acute respiratory syndrome on pulmonary function, functional capacity and quality of life in cohort of survivors. Chest 128(4): 2247-2261.
-
Chan KS, Zheng JP, Mok YW, Li YM, Liu YN, et al. (2003) SARS: prognosis, outcomes and sequelae. Respirology 8(Suppl): 36-40.
-
Das KM, Lee EY, Singh R, Enani MA, Dossari KA, et al. (2017) Follow-up chest radiographic findings in patients with MERS-CoV after recovery. Indian J Radiol Imaging 27(3): 342-349.
-
Ngai JC, Ko FW, Ng SS, To KW, Tong M, et al. (2010) The long-term impact of severe acute res-piratory syndrome on pulmonary function, exercise capacity and health status. Radiology 15(3): 543-550
-
Zhang L, Yan X, Fan Q, Liu H, Liu X, et al. (2020) D-dimer levels on admission to predict in-hospital mortality in patients with COVID-19. J Thromb Haemost 18(6): 1324-1329.
- Bedside Pulmonary Rehabilitation – Mandatory and Cost- Effective Tools
- The Role of Chest Radiology in Traumatic Injuries: A Comprehensive Narrative Review
- Pseudosepsis in Acute Inflammation of the Lung
- An Overview of Lung Injury in Covid-19: Evaluating the Impact of Re-Exposure and Emerging Variants
- Fibreoptic Bronchoscopy-its Role in Pulmonary Medicine-Current Trends in Intensive Care Unit
- Retrospective Study on the Efficacy of Homoeopathic Medicines in the Treatment of Acute Rhinitis