Extrapulmonary Tuberculosis a Clinico-Epidemiological Perspective from a Tertiary Care Centre
Introduction: Tuberculosis is a major global health problem. India accounts for one-fifth of the worldwide incidence of tuberculosis. The proportion of Extra-Pulmonary Tuberculosis among all TB cases varies from country to country. In India, Extra-Pulmonary tuberculosis accounted for 15%-20% of all forms of Tuberculosis. There are sparse data describing the epidemiology of Extra-Pulmonary Tuberculosis, hence this study was done in a tertiary care centre. Methodology: A retrospective longitudinal study was conducted at a tertiary care centre from 2012 to 2016. It included 297 consecutive patients aged>18 years, with a confirmed diagnosis of Extra-Pulmonary Tuberculosis. Demographics, clinical information, investigations, imaging, organ involvement, the mode of diagnosis and time to diagnosis were noted from medical records. Treatment offered and the outcome was analysed. Results: Mean age of the patients was 41 years with majority being young adults. The most common type of EPTB was TB Pleural effusion, followed by Spine and Meninges. The most common modality of diagnosis was Pleural aspiration followed by clinico-radiological and biopsy. The time taken for diagnosis of Skeletal TB was the longest. A total of 287 (96.63%) patients were initiated on anti-tuberculosis treatment after establishing the diagnosis. Conclusion: Early diagnosis of EPTB is challenging due to its atypical presentation. EPTB is prevalent even amongst those without immunocompromising conditions. The delay in diagnosis noted in this study is largely on account of patients presenting late to the hospital, thus making education and awarenes
Introduction
Extrapulmonary Tuberculosis (EPTB) refers to the involvement of tissues by Mycobacterium tuberculosis in the absence of lung involvement. Tuberculosis is a global health problem and India in particular represents a high burden country. There is a rising trend in EPTB cases globally, despite an overall decline in cases of tuberculosis. This is largely due to the HIV pandemic and due to voids in National policies regarding its optimal management [1, 2, 3, 4]. In view of the scant literature related to EPTB, this study was taken up to analyse its clinical spectrum and identify potential factors related to its rising incidence and gaps in optimal management, at a tertiary care centre.
Materials & Methods
A retrospective, longitudinal study was conducted in a tertiary care centre in South India from 2012 to 2016. The source of information was the patient’s case records from the medical records department. Inclusion criteria-Patients aged >18 years with a diagnosis of extrapulmonary tuberculosis. Exclusion criteria-Patients with pulmonary tuberculosis with or without extrapulmonary organ involvement. Data of all consecutive patients aged≥18 years, with confirmed diagnosis of EPTB as per records were included. The study population consisted of all patients attending various departments with a probable diagnosis of EPTB. Thus 297 consecutive patient records satisfying study criteria were included.
Demographics, clinical information, relevant investigations, HIV status, imaging, organ affected, the mode of diagnosis, time taken to diagnose, treatment offered, treatment duration and treatment outcome were recorded. Patients who were referred to other centres for follow up while on antituberculosis treatment (ATT) were telephonically contacted to assess adherence to treatment and treatment completion. The diagnosis of EPTB was based on clinical features, radiological changes, analysis of fluid samples, histopathology consistent with tuberculosis and satisfactory response to ATT, as defined in the INDEX-TB guidelines for Management of extrapulmonary tuberculosis [5]. This study was approved by the Institutional Ethics Committee.
Statistical Analysis
All quantitative variables such as age, duration of symptoms, time from onset of symptoms to diagnosis, time from the first consultation to a health care facility to initiation of ATT and duration of treatment were expressed in terms of mean and standard deviation or median with an interquartile range based on the distribution. Categorical variables such as comorbidities, mode of diagnosis, organs involved, and various aspects of treatment were expressed in terms of percentage. A Chi-square test was employed to estimate the association between age and gender distribution. A graphical presentation of data was undertaken for salient features. Statistical analysis was done using SPSS Inc. 2009 Release, PASW, Statistics for Windows, version 18.0, Chicago: SPSS Inc. A P value of less than 0.05 was considered to be significant.
Results
This study included 297 consecutive patients. The median age of the study population was 39 years with interquartile range (IQR) of 26 to 53 years with majority (34%, n=101) being young adults (<30 years). 64% (n=190) of the patients were male and 36% (n=107) female. The cases were categorised by age into 4 groups as follows, 18- 29 years, 30-44 years, 45-59 years and≥60 years. The differences in the age distribution between the genders was not statistically significant (p=O.339) (Figure 1).
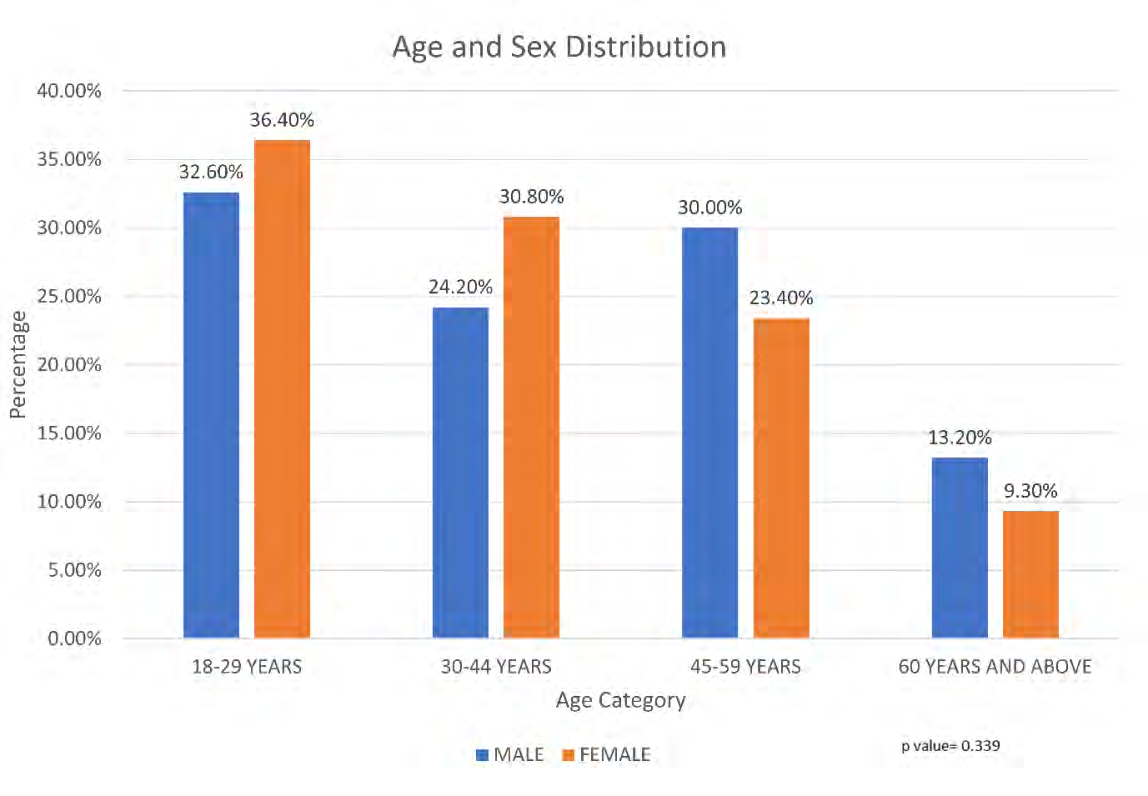
The majority of cases occurred in the age group of 18 to 29 years (34%, n=101). Those between 30 to 44 years accounted for 26.6% (n=79) of cases, between 44 to 59 years accounted for 27.6% (n=82) and 11.8% (n=35) of cases occurred in those above 60 years of age. However, these differences were not statistically significant (p=0.286). The most common symptoms observed were fever (43.4%) and joint pain (38.4%) as shown in Table 1.
| Serial No. | Symptom* | Frequency (%) |
|---|---|---|
| 1 | Joint pain | 114(38.0) |
| 2 | Fever | 128(42.7) |
| 3 | Loss of weight | 40(13.3) |
| 4 | Headache | 15(4.7) |
| 5 | Dysuria | 2(0.7) |
| 6 | Scrotal swelling | 4(1.3) |
| 7 | Weakness | 26(8.7) |
| 8 | Cough | 61(20.3) |
| 9 | Loss of appetite | 25(8.3) |
| 10 | Breathlessness | 35(11.6) |
| 11 | Hematuria | 1(0.3) |
| 12 | Chest pain | 50(16.7) |
Table 1: Symptoms at presentation.
*The most predominant symptom in each patient was considered. Table 1: Symptoms at presentation.
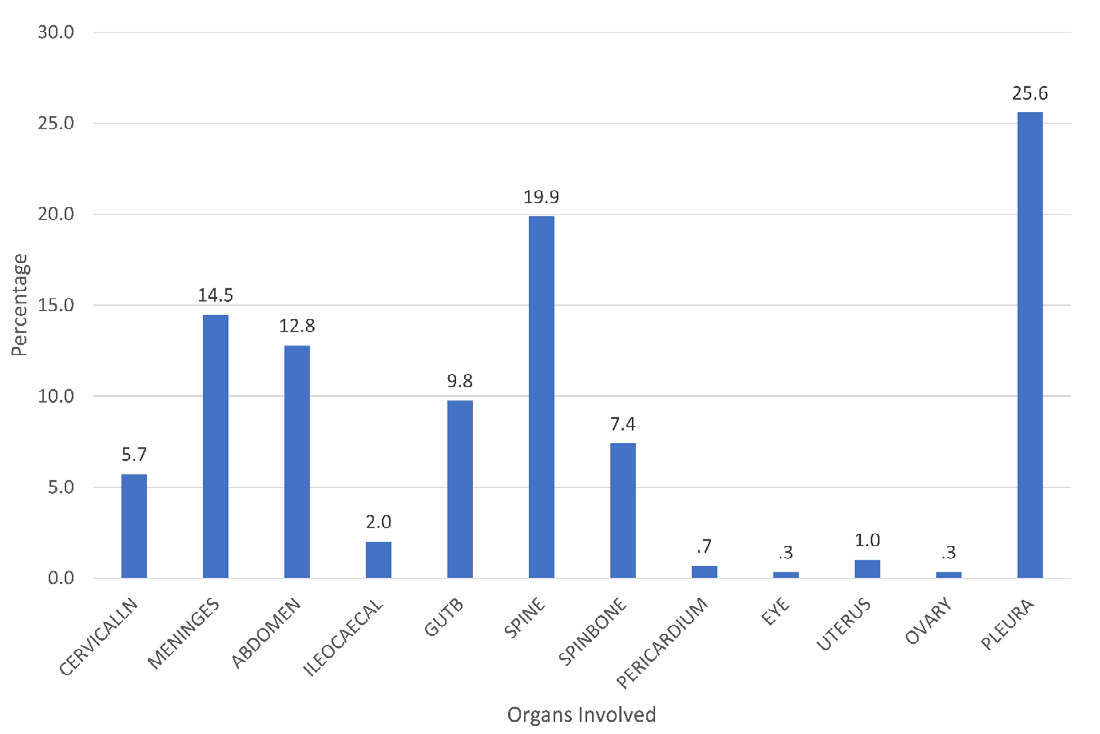
Tuberculous pleural effusion was the most common type of EPTB in our study with 25.6% (n=76) of cases, followed by TB spine (19.9%, n=59) and meningeal TB (14.5%, n=43). TB of the Abdomen occurred in 12.8% (n=38), that of genitourinary in 9.8% (n=29), bones other than spine in
7.4% (n=22), cervical lymph nodes in 5.7% (n=17), ileocecal in 2% (n=6), uterus in 1% (n=3), pericardium in 0.7% (n=2), ocular in 0.3% (n=1) and ovarian in 0.3% (n=1) of patients. The difference in distribution of organs involved between the two genders was statistically significant (p=0.001) with males accounting for the majority (Figure 2).
Tuberculous pleural effusion when distributed by age categories did not show any statistical significance (p= 0.581), 55.3% of cases occurred before and 44.7% after the age of 44 years. However, the gender wise incidence of tuberculous pleural effusion among all EPTB cases in this study was statistically significant (p= 0.000001) with 82.9% being males. Of the 190 males, the involvement of TB spine was 21.6% (n=41) as compared to 16.82% (n=18/107) among females. This difference was not statistically significant when compared to other organs (p=0.324). 47.5% of cases of TB spine in this study occurred before the age of 44 years (18-29 years-33.9%; 30-44 years-13.6%), the remaining 52.5% of cases occurred above the age of 44 years (18-29 years-35.6%; 30-44 years-16.9%). This difference between age groups was found to be statistically significant (p=0.045). There was no significant difference in the gender wise distribution of TB Spine (p=0.324).
Tuberculous pleural effusion when distributed by age categories did not show any statistical significance (p= 0.581), 55.3% of cases occurred before and 44.7% after the age of 44 years. However, the gender wise incidence of tuberculous pleural effusion among all EPTB cases in this study was statistically significant (p= 0.000001) with 82.9% being males. Of the 190 males, the involvement of TB spine was 21.6% (n=41) as compared to 16.82% (n=18/107) among females. This difference was not statistically significant when compared to other organs (p=0.324). 47.5% of cases of TB spine in this study occurred before the age of 44 years (18-29 years-33.9%; 30-44 years-13.6%), the remaining 52.5% of cases occurred above the age of 44 years (18-29 years-35.6%; 30-44 years-16.9%). This difference between age groups was found to be statistically significant (p=0.045). There was no significant difference in the gender wise distribution of TB Spine (p=0.324).
Among those with meningeal tuberculosis the incidence by age wise distribution was not statistically significant (p=0.065) although 76.29% of cases occurred before the age of 44 years. Similarly, the gender-wise distribution of Meningeal Tuberculosis also showed no statistical significance (p=0.389). A confirmed diagnosis of EPTB requires a combination of mycobacterial culture, histological examination, and strong evidence of active disease.
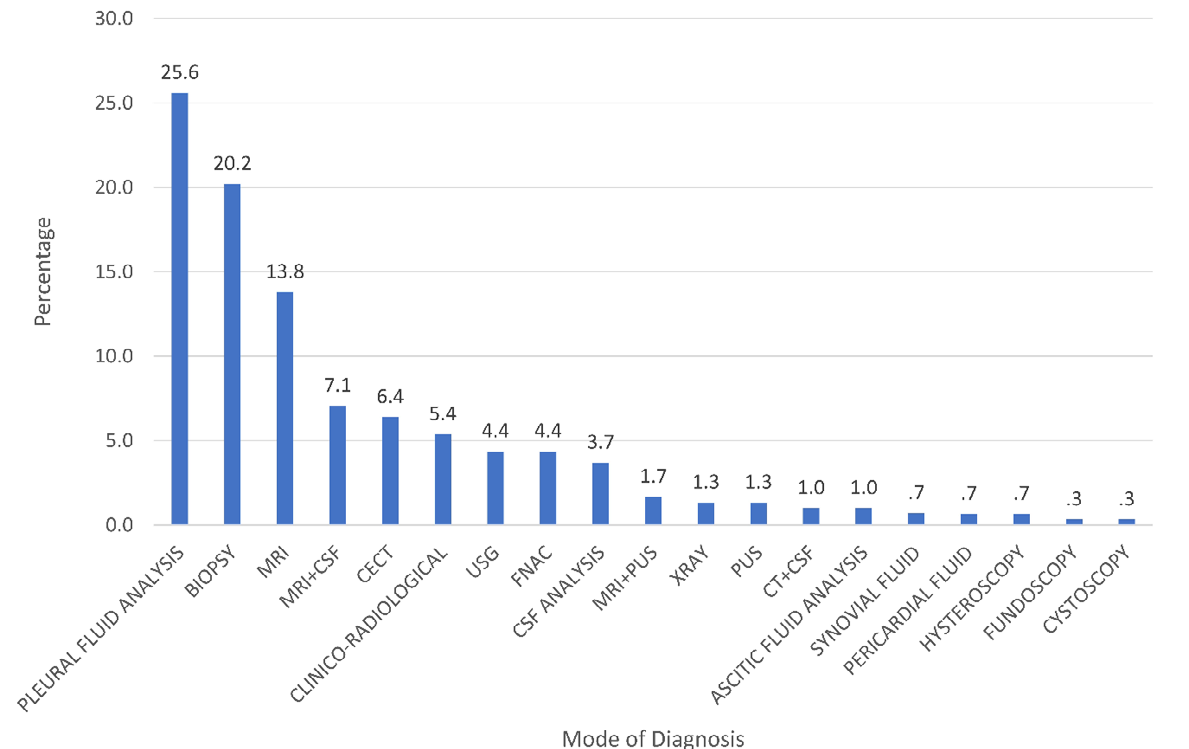
Investigations done included Chest X-Ray in all cases to rule out PTB. Other tests were decided upon organ involvement. It included imaging, fine needle aspiration cytology, Histopathology examination of biopsied tissue, and analysis of pleural fluid, cerebrospinal fluid, ascitic fluid, pericardial fluid, and synovial fluid. Some patients also required cystoscopy, colonoscopy, upper gastrointestinal endoscopy, and hysteroscopy. Pus was tested for Acid-fast bacilli in patients of TB spine with paraspinal collection. AFB positivity was seen in 2.7% of patients. The most common modality of diagnosis was pleural fluid analysis followed by diagnosis based on clinico-radiological findings and biopsy (Figure 3).
The median time taken for diagnosis from onset of symptoms was 30 days with an IQR of 10 to 90 days. 53.5% of the patients were diagnosed in < 30 days, 21.9% in 31-90 days, 6.1% in 91-180 days, 9.4% in 180-270 days, 0.7% in 270-360 days and 8.4% in > 360 days (Table 2).
| <30 days | 31-90 days | 91-180 days | 181-270 days | 270-360 days | >360 days | |
|---|---|---|---|---|---|---|
| Cervical Lymph Node | 35.30% | 41.20% | 5.90% | 5.90% | 0.00% | 11.80% |
| Meninges | 83.70% | 7.00% | 2.30% | 4.70% | 0.00% | 2.30% |
| Abdomen | 50.00% | 31.60% | 10.50% | 7.90% | 0.00% | 0.00% |
| Ileo-caecum | 33.30% | 33.30% | 0.00% | 16.70% | 0.00% | 16.70% |
| Genito-Urinary Tract | 44.80% | 20.70% | 6.90% | 17.20% | 3.40% | 6.90% |
| Spine | 22.00% | 32.20% | 5.10% | 15.30% | 1.70% | 23.70% |
| Bones other than spine | 45.50% | 4.50% | 9.10% | 18.20% | 0.00% | 22.70% |
| Pericardium | 50.00% | 0.00% | 0.00% | 50.00% | 0.00% | 0.00% |
| Eye | 100.00% | 0.00% | 0.00% | 0.00% | 0.00% | 0.00% |
| Uterus | 100.00% | 0.00% | 0.00% | 0.00% | 0.00% | 0.00% |
| Ovary | 100.00% | 0.00% | 0.00% | 0.00% | 0.00% | 0.00% |
| Pleura | 71.10% | 19.70% | 6.60% | 2.60% | 0.00% | 0.00% |
| Total | 53.53% | 21.90% | 6.10% | 9.40% | 0.70% | 8.40% |
Table 2: Distribution of Time from onset of symptoms to diagnosis, by organ involved.
When the spine and other bones were involved, the time from onset of symptoms to diagnosis tended to be longer (Table 3). The median time for diagnosis of TB spine from symptom onset was 90 days with an IQR of 36 to 280
days, 22% presented within 30 days while 23.7% presented with symptoms of more than 360 days. Upon first contact to health care services, the time to start treatment was a median of 4 days with IQR of 3 to 6 days. Likewise for TB of bones other than the spine, the median time for diagnosis from onset of symptoms was 80 days with an IQR of 17 to
248 days, 45.5% presented within 30 days while 22.7% presented with symptoms of more than 360 days. Upon first contact to health care services, the time to start treatment was a median of 6.5 days with IQR of 2 to 8days. The time to diagnosis for other organs is enlisted in Table 3.
| Organ Involved | Frequency (n) | Median | Interquartile Range (25-75) |
|---|---|---|---|
| Cervical Lymph Node | 17 | 60 | 25-135 |
| Meninges | 43 | 12 | 30-May |
| Abdomen | 38 | 38 | Oct-81 |
| Ileo-caecum | 6 | 63.5 | 13-345 |
| Genito-Urinary Tract | 29 | 32 | 10-210 |
| Spine | 59 | 90 | 36-280 |
| Bones other than spine | 22 | 80 | 17-248.75 |
| Pericardium | 2 | 140 | 30-140 |
| Eye | 1 | 10 | 10 |
| Uterus | 3 | 30 | 30-Mar |
| Ovary | 1 | 7 | 7 |
| Pleura | 76 | 16.5 | Jul-32 |
| Total | 297 | 30 | Oct-90 |
Table 3: Median time from onset of symptoms to diagnosis by organ involved.
HIV positive state was seen in 11 patients (3.7%) and all were associated with either TB meningitis or spine. HCV positive status was seen in 1 (0.33%) and HBsAg positive status was seen in 3 (1.01%) patients. Other comorbidities were diabetes mellitus in 24 (8%). The notable finding in this study was relatively low prevalence of comorbidities. Initial presentation of the majority of the patients was to Internal Medicine department (24.2%) (Figure 4).
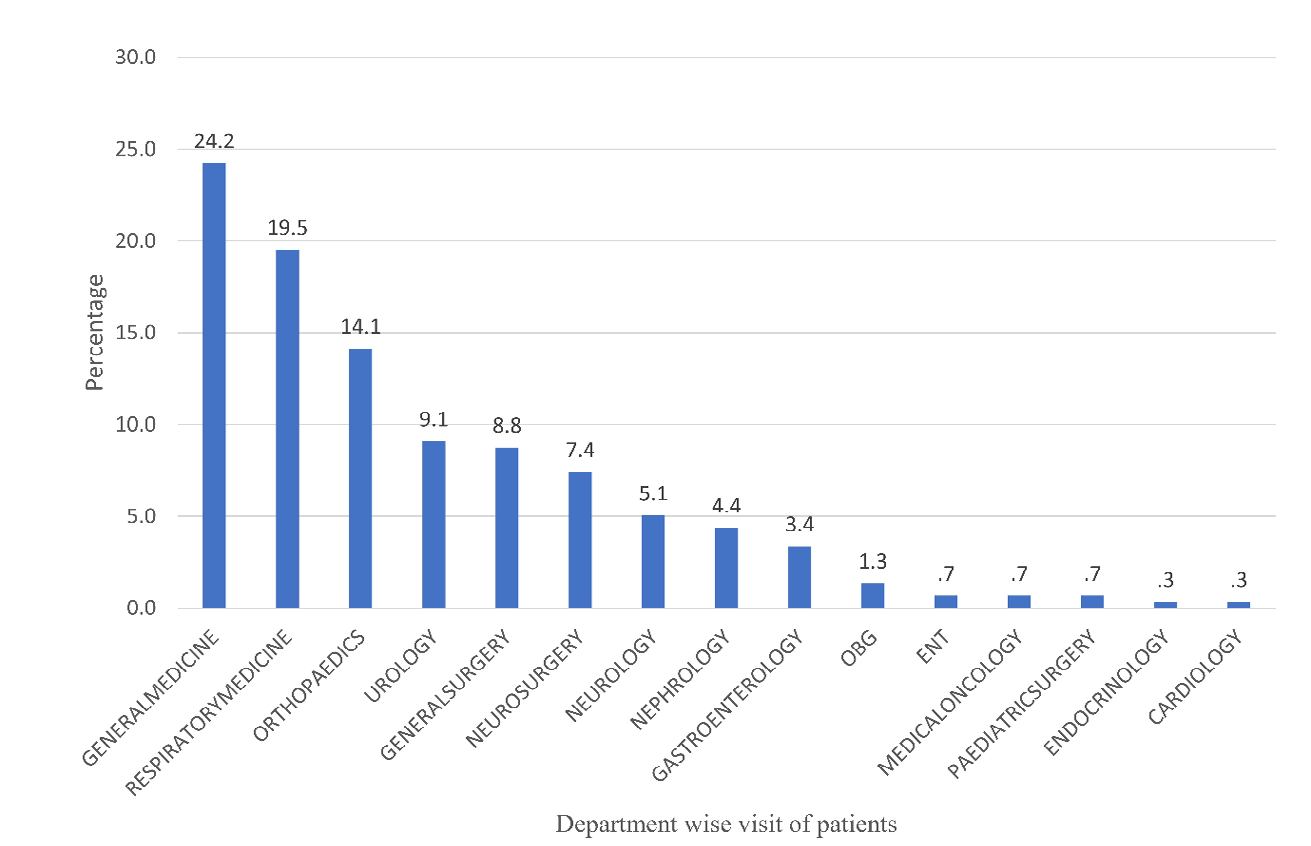
OBG- Obstetrics and Gynaecology, ENT- Ear, Nose and Throat. Figure 4: Department wise distribution of patients.
Among those who were advised treatment, 96.63% (n=287) were initiated on ATT after establishing the diagnosis. The remaining 3.36% (n=10) patients did not follow-up with their biopsy reports. From the first consultation to a tertiary health centre, the median time taken to initiate a patient on ATT was 3 days with an IQR of 2 to 6 days. 45.8% of patients (n=136) have taken drugs dispensed under the Revised National Tuberculosis Programme (RNTCP), now renamed as NTEP (National Tuberculosis Elimination Programme); the remaining 50.8% of patients opted for private drugs (n=151). Other key variables include treatment duration and cure rates (which strictly imply a bacteriological cure, difficult to estimate in EPTB cases).
Analysis of treatment duration among those who were initiated on treatment (n=287) revealed that 16.37% (n=47), 29.26% (n=84) and 32% (n=92) of patients had received treatment for<180 days, 180 days, and >180 days, respectively. The treatment duration was unknown for 22.29% of patients (n=64). Treatment was not initiated for 10 patients since they did not visit the hospital with their reports (Table 4).
| Frequency (%) | |
|---|---|
| < 180 days | 47 (16.37) |
| 180 days | 84 (29.26) |
| > 180 days | 92 (32.05) |
| Unknown | 64 (22.29) |
| Total | 287 (100) |
Table 4: Distribution of patients by duration of treatment.
When the duration of treatment was compared between those receiving government drugs and private drugs, it was observed that 63.3% [86/136] of those on government drugs received treatment for≥180 days, on the other hand 59.6% [90/151] on private drugs received treatment for ≥180 days, this difference was statistically significant (p=0.000001) pointing at better follow- up rates among those on government drugs, considering EPTB often requires longer courses of treatment. Further, 58.1% (79/136) of those who received government drugs completed treatment compared to 54.3% (82/151) among those who received private drugs, this difference was statistically significant (p=0.000001) suggesting better compliance and follow up rates in those on government-sponsored drugs. There was no preference towards choice of ATT, between government sponsored and privately obtained drugs between the different age groups, (p=0.422) nor between the genders (p=0.206).
Discussion
Tuberculosis is an infectious disease caused by the bacillus Mycobacterium tuberculosis. It typically affects the lungs but can also affect other sites (EPTB). Worldwide, TB is the ninth leading cause of death and the leading cause due to a single infectious agent, ranking above HIV/AIDS. In 2018, there were an estimated 1.2 million TB deaths among HIV-negative people. EPTB constitutes about 15-20% of all cases of TB in immunocompetent individuals in India. The incidence is more in immunocompromised individuals like HIV, DM, cancer, malnutrition, CKD, liver diseases, post organ transplant, etc. HIV epidemic in many regions of the world has led to an increase in EPTB cases in different populations accounting for 19.3% (5.8 to 44.4%) of all TB notified cases in the European Union, 18.7% in the USA and 12% in Brazil. In contrast to PTB, EPTB rates show no decline in trend. The proportion of EPTB increased from 16.4% in 2002 to 22.4% in 2011 in the European Union [4]. HIV infection is the greatest risk factor for the development of EPTB disease in persons with latent TB, due to a weakened immune system [6].
EPTB occurs as a result of contiguous spread of tubercle bacilli to adjoining structures, such as pleura or pericardium, or by lympho-hematogenous spread during primary or chronic infection. Cervical and gastrointestinal TB may also result from the ingestion of M. Bovis-infected milk particularly in the rural area where pasteurization of milk is not available [7]. Atypical presentation, lack of resources for procurement of tissue or fluid from inaccessible sites leads to considerable delay in diagnosis [8]. This study was done to analyze the clinical characteristics of various EPTB patients, in a single-centre experience. A younger age group and male preponderance have been reported as independent risk factors for EPTB. Our study did not show any significant sex predilection in contrast to other studies. A study by Ramaprakasha et al and other studies have shown male preponderance [8, 9, 10]. Clinical patterns of EPTB are diverse in different regions of the world and India. Globally women were found to be more at risk of developing EPTB [11, 12, 13, 14].
Tuberculosis of the pleura was the commonest presentation in our study, followed by TB spine and meninges. In a study by Ramaprakasha, CNS TB & TB of bones and joints was more common in females [10]. The predominant organs involved was pleura and lymph nodes in other studies [9, 10, 11, 12, 13, 15]. TB lymphadenitis was less in our study in contrast to other studies. The reason could be that the study was done in a medical college located in a metropolitan city. Tertiary care centres such as medical colleges cater to a large and varied type of population and provide an excellent place for advanced diagnostic facilities. Patients seeking advanced diagnostic facilities sought medical care in our centre. Other studies have shown that the diagnosis of EPTB can be quite challenging due to the heterogeneity of clinical manifestations and difficulties in obtaining proper specimens for necessary investigations [16]. The time to reach a diagnosis was highest among those with skeletal tuberculosis and this group represented a predominantly younger population (Table 5).
| TB of the Spine (Frequency in %) | TB of the Bones other than spine (Frequency in%) | |
|---|---|---|
| 18-29 years | 33.9 | 27.3 |
| 30-44 years | 13.6 | 45.5 |
| 45-59 years | 35.6 | 13.6 |
| >60 years | 16.9 | 13.6 |
Table 5: Agewise distribution of Skeletal Tuberculosis.
This group also had lower documented treatment completion rates, 52.5% and 77.3% for TB spine and Tb of bones other than the spine, respectively (Table 6).
| Organ Involved | Treatment Completion | ||
|---|---|---|---|
| Unknown | Incomplete | Complete | |
| Cervical Lymph Node | 35.30% | 58.80% | 5.90% |
| Meninges | 34.90% | 58.10% | 7.00% |
| Abdomen | 23.70% | 63.20% | 13.20% |
| Ileo-caecum | 16.70% | 83.30% | 0.00% |
| Genito-Urinary Tract | 48.30% | 44.80% | 6.90% |
| Spine | 32.20% | 52.50% | 15.30% |
| Bones other than spine | 22.70% | 77.30% | 0.00% |
| Pericardium | 50.00% | 50.00% | 0.00% |
| Eye | 100.00% | 0.00% | 0.00% |
| Uterus | 33.30% | 66.70% | 0.00% |
| Ovary | 100.00% | 0.00% | 0.00% |
| Pleura | 50.00% | 44.70% | 5.30% |
Table 6: Distribution of treatment completion rates by organ involved.
This sheds light on the inadequacy of contact tracing, which is largely focused on pulmonary tuberculosis. An initiative for long term symptom monitoring for contacts of pulmonary tuberculosis with focus on both pulmonary as well as extrapulmonary symptoms is required, thus enabling early identification. This calls for larger allocation of resources, training programmes and updated follow up and notification systems with a wider horizon of services to encompass extrapulmonary tuberculosis.
This study revealed that there was no health system delay upon contact with health care services, in diagnosis and initiation of ATT. A hospital-based study from Central India had reported health system delay in the diagnosis of EPTB of up to 7 weeks [17]. Other key variables analysed, include treatment duration and cure rates (which strictly implies a bacteriological cure, difficult to estimate in EPTB cases). It is difficult to label a patient with EPTB as ‘Cured’ as defined by the Guidelines for the programmatic management of tuberculosis in India [18, 19], thus treatment completion and clinical response may be the most feasible way to estimate the treatment outcome of a patient. Patients who complied with treatment duration can be assumed to have higher cure rates.
In this study, 287 out of 297 patients were initiated on treatment, 151 received private drugs and 136 drugs sponsored by the government under the RNTCP (now NTEP). The preference of choice of drugs between government sponsored and privately obtained medication were equivocal among the different age groups and genders. Yet the follow- up and treatment completion rates seemed to be higher among those on government sponsored drugs. The analysis of factors leading to these differences is an important research question. The current study being retrospective in nature was limited in its ability to analyse the factors leading to these preferences either of the prescribing doctor or of the patients themselves. The majority of our patients had follow up visits numbering 8 and 10. The reason could be a good physician-patient relationship which ensures better adherence to treatment.
TB control programmes focus more on the management of sputum smear-positive TB in endemic countries to control the disease. EPTB is not well addressed by national programmes in developing countries because of its paucibacillary state and its non-contagious nature. High incidence of patients not completing treatment emphasises the need to focus on supervised treatment as a policy for optimizing care and improve treatment outcomes.
Limitation of the study are, the outcome of treatment could not be assessed due to lack of regular follow up among patients. A significant number of patients with TB of bones have taken treatment for less than 6 months highlighting gaps in programme implementation. Owing to the retrospective design of the study, data pertaining to treatment preference between government and private medication was not entirely available for stratified analysis.
Active contact tracing and long term surveillance of contacts to look for both pulmonary and extrapulmonary symptoms is needed to achieve success in the END TB programme. Educational programmes at various levels of society to improve awareness on importance of treatment adherence and treatment completion is recommended.
Conclusion
EPTB continues to be a pressing public health problem despite being a curable disease for a significant proportion of the world. Each year millions of people are diagnosed and successfully treated for TB but there are still large gaps in early detection and treatment of extra pulmonary tuberculosis. It has not received much attention in control strategies.
The rising incidence of EPTB should be tackled through policy changes in the national programme made suitable for the management of Extrapulmonary Tuberculosis and in line with END TB strategy envisaged by the WHO. The revised RNTCP guidelines despite emphasising on EPTB have not made significant differences in diagnosis and treatment of the same.
Mortality due to TB could be prevented with early diagnosis and appropriate treatment. Prevention strategies must include bovine tuberculosis which is caused by Mycobacterium Bovis that spreads from animals to humans and results in TB cervical lymphadenitis. EPTB is prevalent even among those without immunocompromising conditions, thus the scope of proposed policies must be aimed at the general population.
In the era of End TB strategy, TB monitoring needs to be expanded to reduce the disease burden. EPTB should be given equal priority like pulmonary tuberculosis under the national programme. Reinforcement of the guidelines regularly to all the medical practitioners and students is required to reduce the morbidity and mortality associated with the disease.
Improved case finding, notification and reporting systems, as in PTB forms the basis for the optimal management of EPTB. Additionally, including private practitioners and pharmacists under the ambit of the National Programme Reporting System, may provide a larger data base and thus improve treatment outcomes.
References
-
World Health Organization (2019) Global tuberculosis report 2019. World Health Organization, Geneva.
-
Adada H, Valley MA, Nour SA, Mehta J, Byrd RP, et al. (2014) Epidemiology of extra-pulmonary tuberculosis in the United States: high rates persist in the post-HIV era. The International Journal of Tuberculosis and Lung Disease 18(12): 1516-1521.
-
Sharma SK, Mohan A (2004) Extrapulmonary tuberculosis. Indian J Med Res 120(4): 316-353.
-
Pang Y, An J, Shu W, Huo F, Chu N, et al. (2019) Epidemiology of Extrapulmonary Tuberculosis among Inpatients, China, 2008-2017. Emerging Infectious Diseases 25(3): 457-464.
-
Sharma SK, Ryan H, Khaparde S, Sachdeva KS, Singh AD, et al. (2017) Index-TB guidelines: Guidelines on extrapulmonary tuberculosis for India. The Indian journal of medical research 145(4): 448-463.
-
Houda BA, Makram K, Chakib M, Khaoula R, Fatma H, et al. (2018) Extrapulmonary Tuberculosis: Update on the Epidemiology, Risk Factors and Prevention Strategies. International Journal of Tropical Diseases 1(1).
-
Schaaf H, Zumla A, Grange J (2009) Tuberculosis [Philadelphia]: Saunders Elsevier.
-
Shrivastava AK, Brahmachari S, Pathak P, Kumar R, Sainia T, et al. (2015) Clinico-Epidemiological Profile of Extra- pulmonary Tuberculosis in Central India. International Journal of Medical Research and Review 3(2): 222-230.
-
Velingker A, Lawande D, Dcosta L (2018) Clinico- epidemiological profile of extra pulmonary tuberculosis in Western India. International Journal of Contemporary Medical Research 5(2): 1-4.
-
Prakasha SR, Suresh G, Shetty S, Peter D’sa I, Kumar SG (2013) Mapping the pattern and trends of extrapulmonary tuberculosis. Journal of Global Infectious Diseases 5(2): 54-59.
-
Varghese B, Hajoj SA (2015) Mapping the epidemiology and trends of extra-pulmonary tuberculosis in Saudi Arabia. International Journal of Mycobacteriology 4(4): 261-269.
-
Heather MP, Robert HP, Theresa HA, Philip AL, Lori RA (2009) Epidemiology of Extrapulmonary Tuberculosis in the United States, 1993-2006. Clinical Infectious Diseases 49(9): 1350-1357.
-
Gomes T, Santos BR, Bertolde A, Johnson JL, Riley LW, et al. (2014) Epidemiology of extrapulmonary tuberculosis in Brazil: a hierarchical model. BMC Infectious Diseases 14(1): 9.
-
Ohene SA, Bakker MI, Ojo J, Toonstra A, Awudi D, et al. (2019) Extra-pulmonary tuberculosis: A retrospective study of patients in Accra, Ghana. Plos One 14(1): e0209650.
-
Hajoj SA, Shoukri M, Memish Z, AlHakeem R, AlRabiah F, et al. (2015) Exploring the Sociodemographic and Clinical Features of Extrapulmonary Tuberculosis in Saudi Arabia. Plos One 10(2): e0101667.
-
Tahseen S, Khanzada FM, Baloch AQ, Abbas Q, Bhutto MM, et al. (2020) Extrapulmonary tuberculosis in Pakistan- A nation-wide multicenter retrospective study. Plos One 15(4): e0232134.
-
Purohit MR, Purohit R, Mustafa T (2021) Patient Health Seeking and Diagnostic Delay in Extrapulmonary Tuberculosis: A Hospital Based Study from Central India. Tuberculosis Research and Treatment 2019: 1-8.
-
(2021) Guidelines for Programmatic Management of Drug Resistant Tuberculosis in India-2021. Ministry of Health and Family Welfare.
-
(2015) World Health Organization. Implementing the end TB strategy: the essentials. Geneva: World Health Organization.
- Bedside Pulmonary Rehabilitation – Mandatory and Cost- Effective Tools
- The Role of Chest Radiology in Traumatic Injuries: A Comprehensive Narrative Review
- Pseudosepsis in Acute Inflammation of the Lung
- An Overview of Lung Injury in Covid-19: Evaluating the Impact of Re-Exposure and Emerging Variants
- Fibreoptic Bronchoscopy-its Role in Pulmonary Medicine-Current Trends in Intensive Care Unit
- Retrospective Study on the Efficacy of Homoeopathic Medicines in the Treatment of Acute Rhinitis