Hepcidin, Selenium and Superoxide Dismutase in Oxidative Stress and in Dialysis Patients
Chronic kidney diseases (CKDs) are characterized by complex changes in cellular metabolism, leading to oxidative stress (OS), i.e. increased production of oxidative radicals (OR), which can play a key role in a number of clinical complications of this pathology. Trace elements selenium (Se), copper (Cu) and zinc (Zn) play a major role in the antioxidant defense system. The antioxidant enzymes are superoxide dismutases (SODs), catalases (CATs) and glutathione peroxidases (GSH-Pxs). We evaluated serum hepcidin, plasma selenium concentrations and the superoxide dismutase activity in 59 CKD patients on hemodialysis. Patients were monitored at University Hospital “Aleksandrovskaâ€, Clinic of Dialysis Treatment and Clinic of Nephrology. The results were compared with a matched by sex and age control group. Serum hepcidin and SOD activity were determined by ELISA method.Plasma selenium concentration was examined with the help of AAS (Perkin-Elmer). We determined CBC (using hematology analyzer ADVIA 2120, Siemens Healthcare) and biochemical parameters (on automatic analyzer Dimension RxL MAX, Siemens Healthcare) of all participants. The serum iron and TIBC levels were determined by AAS (Perkin-Elmer). For statistical analysis of the results we used Student's paired t-test and Pearson's correlation. We found a statistically significant higher serum hepcidin levels in CKD patients on chronic dialysis (356.6 μg/L ± 52.5 μg/L) compared to the control group (19.4 μg/L ± 2.7 μg/L; P
Introduction
Chronic kidney diseases (CKDs) are characterized by complex changes in cellular metabolism, leading to oxidative stress (OS), i.e. increased production of oxidative radicals (OR), which can play a key role in a number of clinical complications of this pathology. In recent years, a significant amount of evidence has been collected for the key role of OR in many fundamental cellular reactions; such evidence implies that oxidative stress (OS) can play an important role in the pathophysiology of generalized diseases including arteriosclerosis, CKD, diabetes mellitus, malignant diseases and in the process of ageing [1]. Trace elements selenium (Se), copper (Cu) and zinc (Zn) play a major role in the antioxidant defense system. The antioxidant enzymes are superoxide dismutases (SODs), catalases (CATs) and glutathione peroxidases (GSH-Pxs). Numerous studies show that the formation of compounds containing trace elements (mainly enzymes), and not the elements themselves are critical for the biological activities. Trace elements Se, Cu and Zn play a major role in the antioxidant defense system. They perform antioxidative functions through the proteins in which they are included [2]. Serum is a component of about 25 enzymes, including the GSH-Px family, thioredoxin reductases and selenoprotein P which provides antioxidant activity against the occurrence and development of carcinogenicity caused by OR, as well as some other enzymes [3]. In healthy people, the kidneys play an important role in the homeostasis of several trace elements, including Se [4]. Where Se is consumed in quantities close to the human dietary needs, its highest levels are found in the kidneys, followed by the liver [5]. The selenium level in tissues depends on its daily intake and the chemical form in which it is taken. There are scarce publications on the effects of selenium supplementation in CKD patients undergoing conservative and dialysis treatment, as well as on the impact of selenium deficit on the formation and degradation of red blood cells and the influence on the anemic syndrome.
Hepcidin is a key regulatory protein which controls the gut absorption of iron and its distribution in the body [6]. It is a peptide hormone that is generated in the liver in response to a number of signals, including the iron levels in the body. Hepcidin functions by linking and initiating degradation of the ferroportin molecule, the only known iron exporter. Ferroportin is located transmembranously in the duodenal enterocytes, macrophages and hepatocytes. It regulates the transfer of cellular iron into the plasma from these cells [7]. Inflammatory cytokines appear to be powerful stimulators for the synthesis of hepcidin, which play a major pathogenic role in the functional iron deficiency in the case of anemia of chronic diseases (ACD). ACD is a well known clinical unit which is frequently observed in patients with different diseases: anemia of infection, anemia of malignant disease, anemia of rheumatoid arthritis and anemia of chronic renal disease. The hematological characteristics of ACD differ from the typical iron-deficiency anemia (IDA) without inflammation. In the case of IDA, erythropoiesis is stimulated by maintaining a sufficient level of oxygen as mycrocytic and hypochromic red blood cells are observed. Unlike IDA, ACD is usually normochromic and normocytic anemia and there is usually no microcytosis, unless iron deficiency is not present simultaneously [7].
Materials and Methods
We evaluated serum hepcidin, plasma selenium concentrations and the superoxide dismutase activity in 59 CKD patients on hemodialysis. Patients were monitored at University Hospital “Aleksandrovska”, Clinic of Dialysis Treatment and Clinic of Nephrology. The results were compared with a matched by sex and age control group. Serum hepcidin and SOD activity were determined by ELISA method. Plasma selenium concentration was examined with the help of AAS (Perkin-Elmer). We determined CBC (using hematology analyzer ADVIA 2120, Siemens Healthcare) and biochemical parameters (on automatic analyzer Dimension RxL MAX, Siemens Healthcare) of all participants. The serum iron and TIBC levels were determined by AAS (Perkin-Elmer). The
soluble transferrin receptors are determined with the aid of nephelometer BN ProSpec (Siemens Healthcare). For statistical analysis of the results we used Student's paired t-test and Pearson's correlation. The data collection form for patients with pathological condition in the exchange of iron has been developed by V. Manolov, M. Velizarova and V. Vassilev on the basis of the recommendations of the Nordic Committee on reference values and their own considerations. Patients with thalassemia, included in the study, signed an informed consent in accordance with the Declaration of Helsinki (Directive 2001/20/EC).
Results
Table 1 presents demographic indicators of included patients with thalassemia.
| CKD patients, on dialysis | ||
|---|---|---|
| Age | Male | Female |
| Age | ||
| Number | 25 | 24 |
| Minimum age (in years) | 35.6 | 37.8 |
| Maximum age (in years) | 51.7 | 52.4 |
| Average age (in years) | 47.1 | 42.8 |
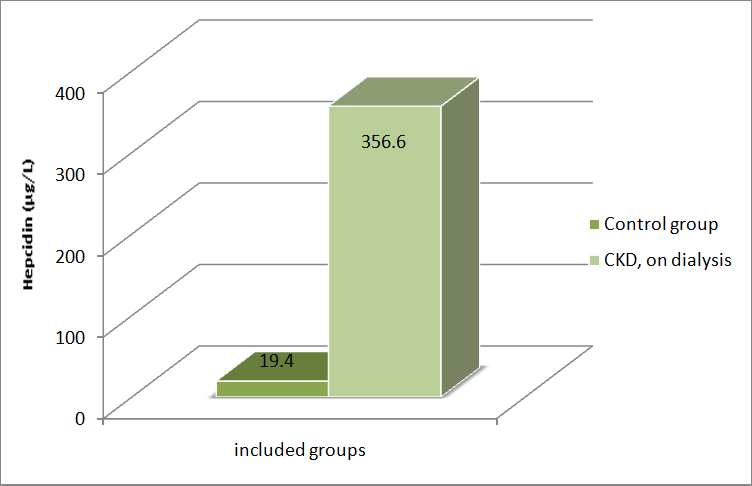
We found a statistically significant higher serum hepcidin levels in CKD patients on chronic dialysis (356.6 μg/L ± 52.5 μg/L) compared to the control group (19.4 μg/L ± 2.7 μg/L; P<0.001). Table 2 presents a comparative assessment of serum concentration of hepcidin in healthy persons and in CKD patients, on dialysis.
| Healthy | CKD | |
|---|---|---|
| n | 59 | 59 |
| X̄ | 19.4 μg/L | 256.6 μg/L |
| min | 5.1 μg/L | 101.4 μg/L |
| max | 25.3 μg/L | 409.7 μg/L |
Table 3: Comparative assessment of serum concentration of hepcidin in healthy volunteers and in CKD patients on dialysis.
The serum level of hepcidin is statistically significantly increased in CKD patients, on dialysis; P < 0.001. (Figure 1).
Plasma selenium levels and SOD activity were decreased in CKD patients on chronic dialysis (422.6 nmol/L ± 51.1 nmol/L; 45.3 μg/mL ± 6.8 μg/mL) compared to the control group (847.5 nmol/L ± 75.4 nmol/L; 101.6 μg/mL ± 10.9 μg/mL; P<0.001). Table 3 presents a comparative assessment of selenium (Se) concentration in healthy persons and in CKD patients.
| Group | Healthy | CKD |
|---|---|---|
| n | 59 | 59 |
| X̄ | 847.5 nmol/L | 422.6 nmol/L |
| min | 511.1 nmol/L | 201.0 nmol/L |
| max | 1099.7 nmol/L | 713.0 nmol/L |
Table 2: Comparative assessment of selenium (Se) concentration in healthy volunteers and in CKD patients, on dialysis.
The level of hepcidin is statistically significantly decreased in CKD patients, on dialysis; P < 0.001 (Figure 2).
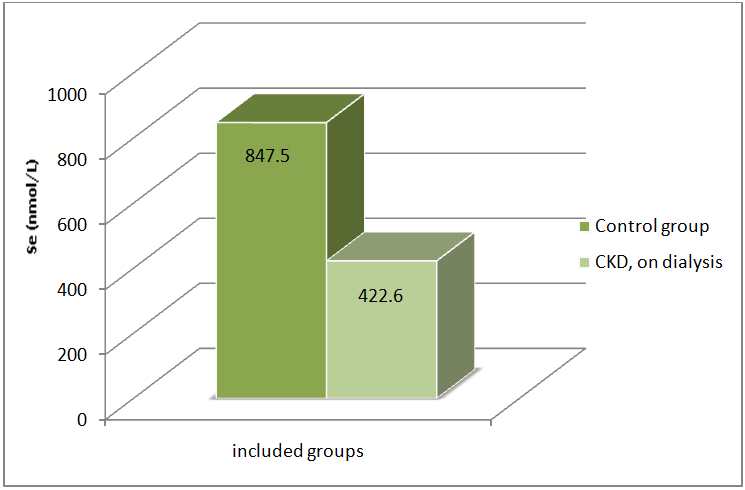
Table 4 presents a comparative assessment of superoxide dismutase (SOD) concentration in healthy persons and in CKD patients.
| Fe (μmol/l) | $\bar{X}$ ± SD | 18.98 ± 7.1 | 12.2 ± 5.96 | |
|---|---|---|---|---|
| n | 59 | 59 | 64.0 ± 8.2 | 45.0 ± 6.5 |
| $\bar{X}$ | 101.6 μg/mL | 45.3 μg/mL | 2.91 ± 0.5 | 1.87 ± 0.4 |
| min | 87.5 μg/mL | 21.1 μg/mL | 2.05 ± 0.9 | 2.11 ± 0.3 |
| max | 135.9 μg/mL | 59.9 μg/mL | 191.6 ± 24.4 | 536.3 ± 96.1 |
| TSAT (%) $\bar{X}$ ± SD 26.2 ± 4.9 27.3 ± 14.1 | ||||
The level of superoxide dismutase is statistically significantly decreased in CKD patients, on dialysis; P < 0.001 (Figure 3).
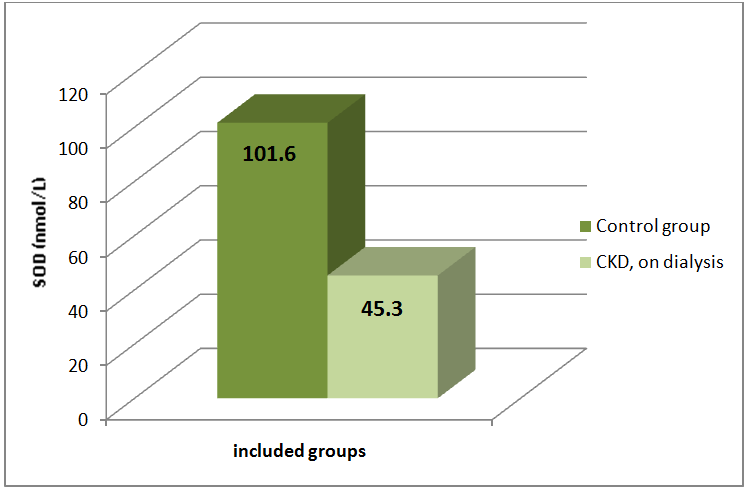
Table 5 presents the results of the determined hematological indicators in the study of healthy volunteers and of CKD patients, on dialysis.
| Group | Healthy | CKD | |
|---|---|---|---|
| Index | Statistics | ||
| RBC (x10*12/l) | $\bar{X}$ ± SD | 4.88 ± 0.5 | 3.34 ± 0.5 |
| Hgb (g/l) | $\bar{X}$ ± SD | 143.4 ± 10.4 | 100.9 ± 12.6 |
| Hct (l/l) | $\bar{X}$ ± SD | 0.429 ± 0.04 | 0.313 ± 0.04 |
| Retic (%) | $\bar{X}$ ± SD | 1.54 ± 0.5 | 1.37 ± 0.5 |
| CHr (pg) | $\bar{X}$ ± SD | 32.6 ± 2.4 | 35.9 ± 3.1 |
| Group | Healthy | CKD | ||
|---|---|---|---|---|
| Group | Healthy | CKD | ||
| n | 59 | 59 | 18.98 ± 7.1 | 12.2 ± 5.96 |
| $\bar{X}$ | 101.6 μg/mL | 45.3 μg/mL | 64.0 ± 8.2 | 45.0 ± 6.5 |
| min | 87.5 μg/mL | 21.1 μg/mL | 2.91 ± 0.5 | 1.87 ± 0.4 |
| max | 135.9 μg/mL | 59.9 μg/mL | 2.05 ± 0.9 | 2.11 ± 0.3 |
| 191.6 ± 24.4 | 536.3 ± 96.1 | |||
| 26.2 ± 4.9 | 27.3 ± 14.1 | |||
Table 7 presents the results of other biochemical and immunological indicators determined in healthy volunteers and in CKD patients, on dialysis.
| Group | Healthy | CKD | |
|---|---|---|---|
| Index | Statistics | ||
| ASAT (U/l) | $\bar{X}$ ± SD | 3.1 ± 0.5 | 48.9 ± 9.9 |
| ALAT (U/l) | $\bar{X}$ ± SD | 20.1 ± 3.2 | 257.8 ± 31.7 |
| CRP (mg/l) | $\bar{X}$ ± SD | 1.12 ± 0.2 | 11.6 ± 7.2 |
| Creatinine (μmol/l) | $\bar{X}$ ± SD | 61.1 ± 1.9 | 716.03 ± 182.2 |
| eGFR (ml/min)* | $\bar{X}$ ± SD | 104.1 ± 12.4 | 6.46 ± 3.7 |
| Glucose (mmol/L) | $\bar{X}$ ± SD | 4.81 ± 0.6 | 5.12 ± 0.5 |
Table 7: Average values and standard deviation of other biochemical and immunological indicators in the control group and in the
*- according to CKD EPI-creatinine equation (2009) Table 7: Average values and standard deviation of other biochemical and immunological indicators in the control group and in the CKD patients, on dialysis.
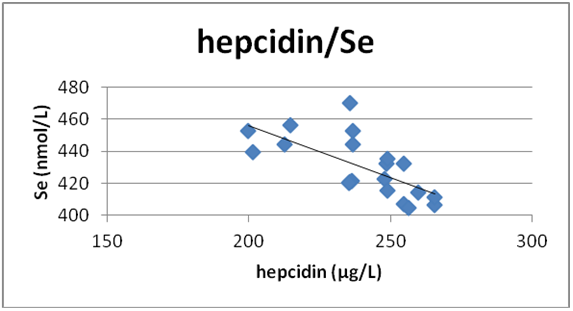
Determination of correlation relationships between hepcidin and different clinico-chemical indicators in CKD patients, on dialysis. 1) Correlation between serum hepcidin and selenium - level of correlation r = -0.659; degree of significance P < 0.001 (Figure 4).
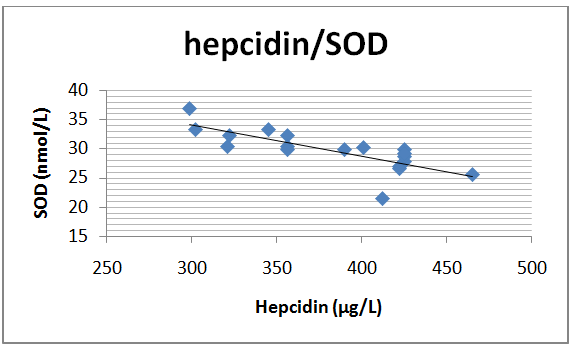
2) Correlation between serum hepcidin and superoxide dismutase - level of correlation r = -0.618; degree of significance P < 0.001 (Figure 5).
Discussion
Chronic kidney diseases (CKDs) are characterized by complex changes in cellular metabolism, leading to oxidative stress (OS), i.e. increased production of oxidative radicals (OR), which can play a key role in a number of clinical complications of this pathology. Free radicals damage different tissues or organs, therefore trace elements and toxic elements enter different organs. The available information shows that in CKD patients in terminal stages the levels of cadmium, chromium, copper, lead and vanadium are higher and the levels of selenium, zinc and magnesium are lower than the levels of the same elements in healthy people. Although some authors do not find difference in the selenium concentration in blood components of CKD patients and of the controls [8], many find significantly lower values [5]. Several authors reveal gradual decrease of the selenium level as the disease progresses [9]. Some authors indicate that in CKD patients who are not on dialysis, the plasma selenium concentration, from the beginning to the final stage of the disease, is by 12.5% to 44% lower than that in healthy people [10]. In the early stages of CKD, the selenium concentration in the blood and in the plasma does not differ materially from the values found in the control group [10]. As the kidney disorder progresses, the selenium concentration in the blood and in the plasma drops. This is especially expressed in the final stage of the disease where the selenium concentration in the blood and in the plasma is by 47 and 50% lower, respectively (P < 0.0001), in comparison with the control group [10]. Examine 34 patients with different degree of renal damage and find higher opposite correlation between the plasma levels of selenium and the values of creatinine (r = -0.55; P < 0.001) [11]. Opposite relationship between the concentration of plasma selenium and the creatinine clearance (r = -0.47, P < 0.001) has been found by Ceballos-Picot et al. [12]. They state that the plasma levels of selenium in dialysis patients are by over 50% lower compared to CKD patients in an advanced stage. Many other authors find similarity in the degree of selenium reduction in dialysis patients and in patients who are in an advanced stage of the disease but are not on dialysis [5]. The question arises on the reason for the lower concentration of selenium in CKD patients. Selenium levels in blood components are also influenced by food which is the main source of this element. The low level of selenium in whole blood and plasma in uremic patients may be associated with decreased intake of proteins and increased protein losses with the urine. As a small peptide that does not seem to be connected to a large extent to the plasma proteins, hepcidin is eliminated from the plasma through the kidneys by ferroportin-mediated endocytosis and proteolysis. Accordingly, concentrations of plasma levels of hepcidin may be increased in disease processes that reduce the hepcidin clearance from the kidneys [13]. High levels of iron in the circulation stimulate the synthesis of hepcidin in the liver. The increased hepcidin reduces the gut absorption of iron and blocks its export from the tissue depots - excessive accumulation of iron in the body is thus avoided. On the other hand, reduced levels of iron suppress the synthesis of hepcidin thus stimulating the absorption of iron through the duodenal enterocytes and its release from the tissue depots. Erythrocytic stimulators and hypoxia [7] also negatively regulate hepcidin in order to increase the availability of iron for erythropoesis. In addition to the increased circulating levels of iron, inflammatory cytokines appear to be powerful stimulators for the synthesis of hepcidin, which play a major pathogenic role in the functional iron deficiency in the case of anemia of chronic diseases (ACD). ACD is a well known clinical unit which is frequently observed in patients with different diseases: anemia of infection, anemia of malignant disease, anemia of rheumatoid arthritis and anemia of chronic renal disease. The hematological characteristics of ACD differ from the typical iron-deficiency anemia (IDA) without inflammation. It is important to note that key characteristics of ACD are the accumulation of iron in the cells of the reticulo - macrophage system, despite the reduced serum levels of iron. In this way, the required level of circulating iron for the synthesis of hemoglobin is not achieved, even in the presence of adequate or high levels of iron in the body's depots. This is probably a protective mechanism for isolation of iron as prevention against certain pathogenic invaders, many of which require iron to develop [7]. However, the diversion of iron from the blood circulation in the macrophages effectively causes functional shortage of iron and restriction of the erythropoiesis, which ultimately, if not corrected, leads to anemia. Anemia is a frequent complication in patients on supporting hemodialysis and contributes to decreasing the quality of life [14]. Despite the great success of recombinant human erythropoietin (EPO) in the clinical practice for treatment of anemia in dialysis patients (chronic kidney disease), the sustainability of this therapy is about 10 - 20% [15]. The shortage of iron is a frequent reason for the resistance to EPO [16]. It is important to make an accurate evaluation of the status of iron, because both anemia and overdosing on erythropoietin- stimulating agents (ESA) are associated with adverse clinical effects [17]. The definition of the status of iron deficiency in dialysis patients, however, is more complicated than in the general population and does not characterize reliably the exchange of iron [18]. The serum ferritin, marker for tissue depots of iron, continues to be useful. The isolated interpretation of serum levels of ferritin is difficult because ferritin also plays a role in the acute phase; it is often increased regardless of the tissue levels of iron depots in patients on supporting hemodialysis [15]. Furthermore, analytical and individual variations of serum ferritin restrict the usefulness as a test for characterisation of the iron status [17]. This leads to the search for more reliable markers for characterisation of the iron homeostatis in these patients. Serum hepcidin seems a promising candidate.
Conclusion
The measurement of hepcidin in CKD, in dialysis patients is necessary to determine whether the application of erythropoietin or erythropoietin stimulating preparations is effective in respect of inefficient erythropoisis. Quantitative determination of SOD, selenium in CKD, dialysis patients is necessary to establish the presence and severity of the accompanying oxidative stress which additionally aggregates the condition of the patients.
- The hepcidin levels determine the redistribution of iron between the macrophages and the parenchyma cells and therefore may have significance for the extent and the speed of progression of the organ damages.
- The concentration of hepcidin is important to personalize the EPO treatment.
- Hepcidin levels determine the effectiveness of the EPO treatment.
- The determination of SOD, selenium in CKD patients on dialysis helps choose the proper approach to compensate the impaired antioxidant protection of the body.
The presence of anemic syndrome and oxidative stress are indisputable pathological conditions accompanying chronic kidney diseases, especially in their terminal stages and in patients on dialysis treatment. A significant percentage of patients on dialysis are with abnormal levels of certain important trace elements - Zn, Se, Cu, magnesium, and one recently discovered regulator of iron metabolism - hepcidin, and between all of the following conditions are found or suspected interconnections and influences. This gives us grounds to realize the project we have proposed in order to clarify the still unclear ratios between the impaired balances and the possibility to influence them therapeutically in dialysis patients.
References
-
Young IS, Woodside JV (2001) Antioxidants in health and disease. J Clin Pathol 54(3): 176-186.
-
El-Bayoumy K (2001) The protective role of selenium on genetic damage and on cancer. Mutat Res 475(1- 2): 123-139.
-
Brozmanova J, Manikova D, Vickova V, Chovanec M (2010) Selenium: a double-edged sword for defense and offence in cancer. Arch Toxicol 84(12): 919-938.
-
Wasowicz W, Zachara B (1987) Selenium concentration in the blood and in urine of a healthy Polish sub-population. J Clin Chem Clin Biochem 25(7): 409-412.
-
Zachara BA, Gromadzinska J, Wasowicz W, Zbrog Z (2006) Red blood cell and plasma glutathione peroxidase activities and selenium concentration in patients with chronic kidney disease: A review. Acta Biochim Pol 53(4): 663-677.
-
Ganz T (2011) Hepcidin and iron regulation, 10 years later. Blood 117(17): 4425-4433.
-
Sun CC, Vaja V, Babitt JL, Lin HY (2012) Targeting the hepcidin-ferroportin axis to develop new treatment strategies for anemia of chronic disease and anemia of inflammation. Am J Hematol 87(4): 392-400.
-
Milly K, Wit L, Diskin C, Tulley R (1992) Selenium in renal failure patients. Nephron 61(2):139-144.
-
Zachara BA, Salak A, Koterska D, Manitius J, Wasowicz W (2004) Selenium and glutathione peroxidases in blood of patients with different stages of chronic renal failure. J Trace Elem Med Biol 17(4): 291-299.
-
Zachara BA, Adamowicz A, Trafikowska U, Trafikowska A, Manitius J, et al. (2001) Selenium and glutathione levels, and glutathione peroxidase activities in blood components of uremic patients on hemodialysis supplemented with selenium and treated with erythropoietin. J Trace Elem Med Biol 15(4): 201-208.
-
Schiavon R, Biasioli S, De Fanti E, Petrosino L, Cavallini L, et al. (1994) The plasma glutathione peroxidase enzyme in hemodialyzed subjects. ASAIO J 40(4): 968-971.
-
Ceballos-Picot I, Witko-Sarsat V, Merad-Boudia M, Nguyen AT, Thevenin M, et al. (1996) Glutathione antioxidant system as a marker of oxidative stress in chronic renal failure. Free Rad Biol Med 21: 845-853.
-
Zaritsky J, Young B, Wang HJ, Westerman M, Olbina G, et al. (2009) Hepcidin–a potential novel biomarker for iron status in chronic kidney disease. Clin J Am Soc Nephrol 4(6): 1051-1056.
-
Eleftheriadis T, Liakopoulos V, Antoniadi G, Kartsios C, Stefanidis I (2009) The role of hepcidin in iron homeostasis and anemia in hemodialysis patients. Semin Dial 22(1): 70-77.
-
Hasuike Y, Nonoguchi H, Tokuyama M, Ohue M, Nagai T, et al. (2010) Serum ferritin predicts prognosis in haemodialysis patients: the Nishinomiya study. Clin Exp Nephrol 14(4): 349-355.
-
Lankhorst CE, Wish JB (2010) Anaemia in renal disease: diagnosis and management. Blood Rev 24(1): 39-47.
-
Ford BA, Coyne DW, Eby CS, Scott MG (2009) Variability of ferritin measurements in chronic kidney disease; implications for iron management. Kidney Int 75(1): 104-110.
-
Wessling-Resnick M (2010) Iron homeostasis and the inflammatory response. Annu Rev Nutr 30: 105-122.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report