Testicular Metastasis: Uncommon Prostate Cancer Case Report
Introduction: Prostate cancer is the second most frequent neoplasm in men, and despite being frequently diagnosed, testicular metastases are rarely described. Objective: to report a case of prostate cancer with testicular metastasis in a patient with more than 15 years of follow-up. Case Report: Caucasian male patient diagnosed with prostate cancer in 2003 and bone metastasis in 2005. After years of follow-up and hormonal treatment, evolved with urinary retention. He underwent transvesical prostatectomy and bilateral orchiectomy. The anatomopathological examination indicated metastatic adenocarcinoma in the right testis. Conclusion: This case demonstrates that prostate cancer can metastasize to rare sites, such as the testis. The presence of these reports helps clinical practice and adds to the literature, encouraging further studies on diagnostic approaches and treatment.
Abbreviations
ROS: Reactive Oxygen Species; PSA: Prostate Specific Antigen; ADT: Androgen Deprivation Therapy.
Introduction
Prostate cancer is the second most frequent cancer among men (after non-melanoma skin cancer) in Brazil. In developed countries, the incidence rate is higher as compared to developing countries [1]. Epidemiological studies show that the risk of diagnosis of prostate cancer has a strong familial componente [2], being twice as high for patients with affected parents at any age, and four times when two or more first-degree relatives had the disease [3].
Age is the main risk factor, starting at 50 years, with an average of 72 years [4]. Genetic alterations such as BRCA-2 mutation and increased reactive oxygen species (ROS) and reactive nitrogen species released by immune cells have also been evidenced as risk factors, causing direct damage to DNA and genetic instability [5].
The evolution of prostate cancer occurs in a continuum process, from the appearance of a pre-neoplastic and invasive lesion located in the prostate to a metastatic lesion. Usual acinar adenocarcinoma accounts for more than 95% of identified tumors [6]. The most typical locations for metastasis are the pelvic lymph nodes, bones, lungs and liver, rarely metastasize to testis. The objective of this work is to report a case of prostate cancer with subsequent diagnosis of testicular metastasis [7].
F.J,G, 78 years old, male, seeks medical attention due to a urinary retention caused by hematuria and constipation. History of prostate câncer, acquired 17 years ago, bone metastasis diagnosed 2 years later, under hormonal treatment with Leuprorelin and Pamidronate, remaining asymptomatic until medical check. Last check-up with oncology, presented a serum prostate-specific antigen (PSA) level of 13 ng/ml. He also had a history of alcoholism, sedentary lifestyle and stroke 8 years ago, with neurological and motor sequelae.
On physical examination, there were no palpable masses; digital rectal examination showing a large, irregular, stony prostate, smooth mucous membranes and no tumors, clinically stable.
- Ultrasonography: 148 g prostate and alterations suggesting chronic nephropathy.
- Colonoscopy: presence of non-malignant polyp. Because of the condition, tunneling of the prostate (transvesical prostatectomy) and bilateral orchiectomy were chosen, with no complications in the procedure. Last control of total PSA level: 12,39 ng/dl.
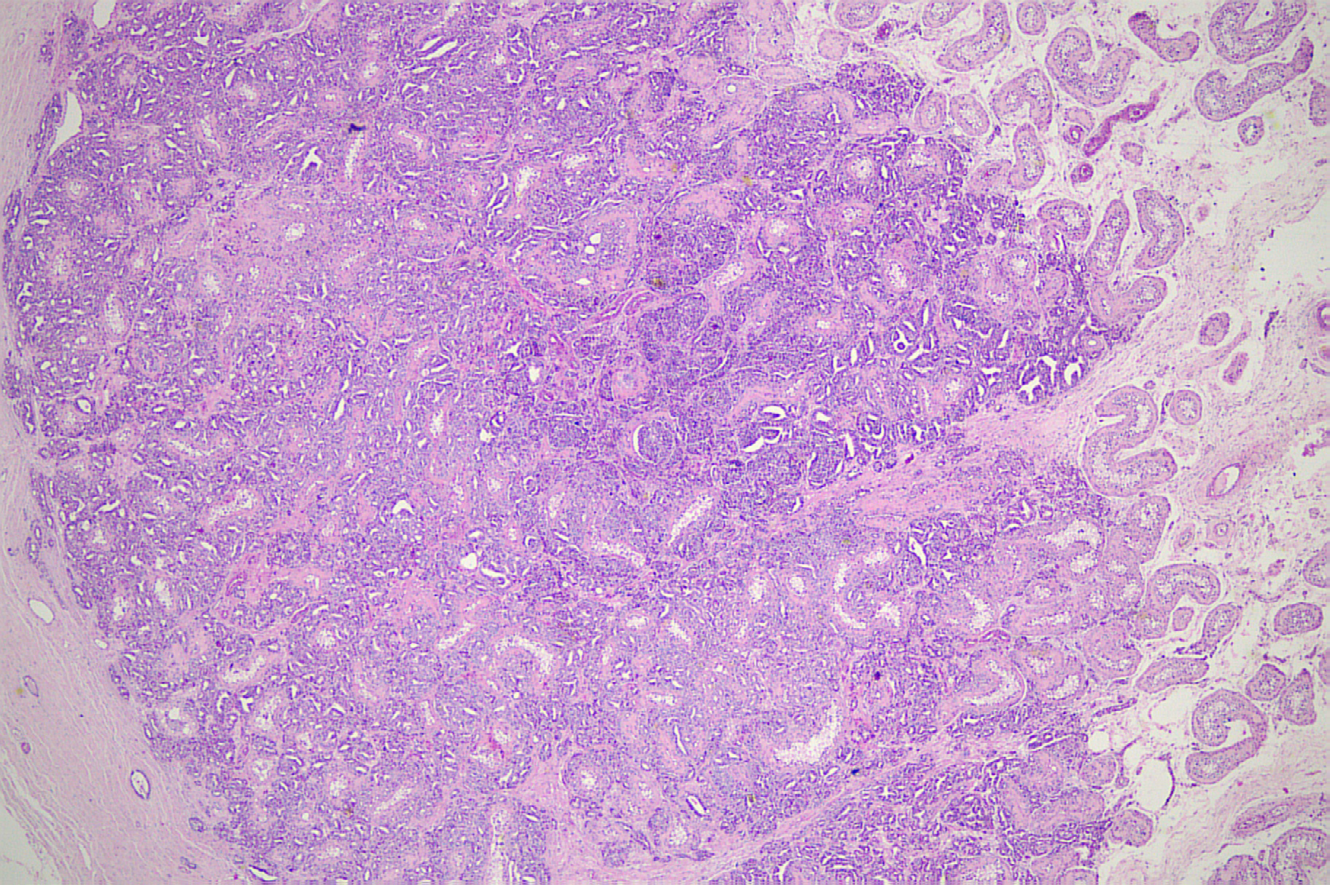
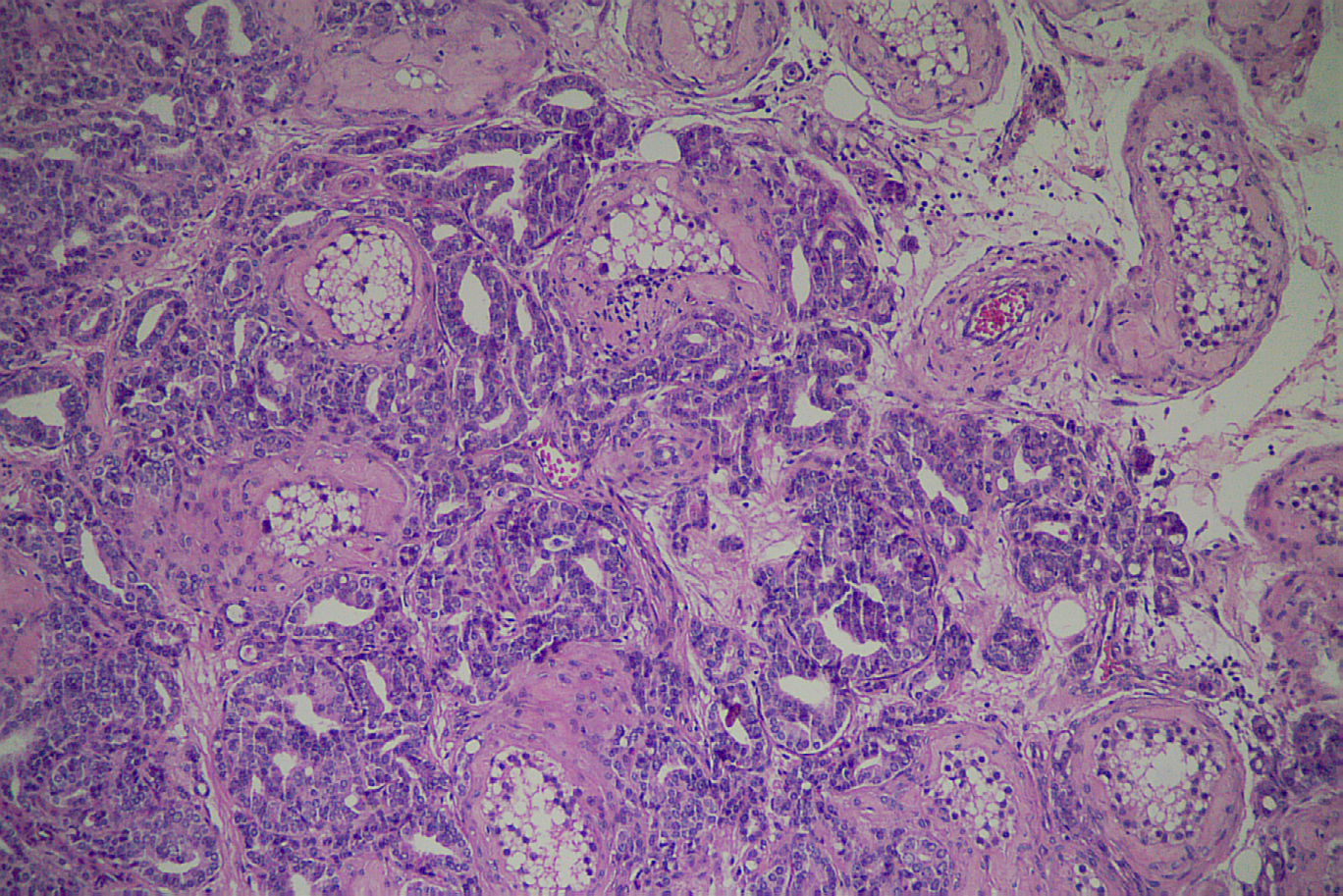
- Anatomopathological: Orchiectomy: metastatic adenocarcinoma in the right testis. Prostate with usual acinar adenocarcinoma gleason 9 (5+4) Figures 1& 2.
Discussion
In advanced prostatic neoplastic disease, local extension often affects the periprostatic tissue, the seminal vesicles and the base of the urinary bladder, and may even cause ureteral obstruction. Metastases spread via the lymphatics, to the obturator lymph nodes, and subsequently to the paraaortic lymph nodes. The hematogenous dissemination occurs to the bones, mainly to the axial skeleton, rarely some lesions disseminate to the viscera, affecting the lungs, liver and brain [8]. With the exception of leukemia and lymphoma infiltration, secondary testicular neoplasia is rare, with an overall incidence of 0.06% [9].
Testicular metastases are usually asymptomatic and detected incidentally during an autopsy or after bilateral orchiectomy for hormonal tumor suppression in advanced prostate câncer [9]. There are rare cases of patients who present edema, pain or testicular masses [10]. Metastases can progress through four possible mechanisms: arterial embolism, via the vas deferens lumen, venous route, and retrograde lymphatic pathway [11].
In the treatment of metastatic disease, radical prostatectomy has no therapeutic value in this phase of the disease, as tunneling may be indicated in cases with obstructive urinary symptoms [12]. However, the main objective in metastatic cases is systemic treatment aimed at reducing symptoms and prolonging survival with quality of life. The main form of systemic treatment for metastatic prostate carcinoma is Androgen Deprivation Therapy (ADT), which in this case started with the use of an LHRH agonist (Leuprorelin) and was replaced by orchiectomy when the patient was submitted to tunneling. The finding of metastasis to the testis was an incidental finding in this case.
Normally, after diagnosis of testicular metastasis, the prognosis is unfavorable, as the disease already has systemic dissemination [13]. In the absence of treatment, the survival of these patients can be only 6 to 18 months [10].
Our patient was treated by bilateral orchiectomy and tunneling for the treatment of obstructive symptoms, the patient died due to his advanced metastatic disease six months after the intervention.
Conclusion
Testicular metastases secondary to prostate cancer are very rare. In our case, the patient did not have symptoms, but it is important to consider this differential diagnosis for those with prostate cancer and painless nodules or swelling of the testicles that may require additional interventions.
References
-
INCA (2022) Prostate cancer. Gov.br Ministry of Health, Brazil.
-
Hjelmborg JB, Scheike T, Holst K, Skytthe A, Penney KL, et al. (2014) The heritability of prostate cancer in the Nordic Twin Study of Cancer. Cancer epidemiology, biomarkers & prevention 23(11): 2303-2310.
-
Michał K, Vangronsveld J, Nawrotet TS (2011) An epidemiological reappraisal of the familial aggregation of prostate cancer: a meta-analysis. PloS one 6(10): e27130.
-
Daniyal M, Siddiqui ZA, Akram M, Asif HM, Sultana S, et al. (2014) Epidemiologia, Etiologia, Diagnóstico e Tratamento do Câncer de Próstata. Asian Pacific Journal of Cancer Prevention 15(22): 9575-9578.
-
Bono JSD, Guo C, Gurel B, Marzo AMD, Sfanos KS, et al. (2020) Prostate carcinogenesis: inflammatory storms. Nat Rev Cancer 20: 455-469.
-
Paner GP, Jimenez RE, MacKenney JK, Amin MB (2010) Prostate Neoplasms. In: Amin MB, et al. (Eds.), Diagnostic Pathology Genitourinary. 1st (Edn.), Amirsys, Los Angeles, California, USA, pp: 64-169.
-
Kusaka A, Koie T, Yamamoto H, Hamano I, Yoneyama T (2014) Testicular Metastasis of Prostate Cancer: A Case Report Case Rep Oncol 7(3): 643-647.
-
Zoran C, Dejan S, Predrag A, Spasic A (2016) Milicevic S Metastasis of Prostate Adenocarcinoma to the Testis. Med Arch 70(4): 318-320.
-
Kollitsch L, Hamann C, Knüpfer S, Meyer D, Kneissl P, et al. (2020) Symptomatic testicular metastasis of an acinar adenocarcinoma of the prostate. Urologia A 59(9): 1092- 1094.
-
Bonfim LR, Lara RC, Guimarães LC, Santos CC, Braga SQP, et al. (2019) Carcinoma de Próstata com Metástase testicular: Case Report. Uromines 7(5).
-
Connelly ZM, Azzawe A, Flowers A, Fazili A, Craighead C, et al. (2021) Prostate cancer metastatic to bilateral testicles: case report and literature review. Am J Clin Exp Urol 9(2): 182-188.
-
Teo MY, Rathkopf DE, Kantoff P (2019) Treatment of Advanced Prostate Cancer. Annual review of medicine 70: 479-499.
-
Andrew T, Graff JM, Mark M (2019) Case report of metastatic prostate cancer to testicles: An ominous sign of advanced disease. Urology Case Reports 26: 100935.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Ischemic Gangrene of the Penis: A Rare Case Report