Residual Urine Measurement in Children with Voiding Disorders: Comparison between Ultrasonographic Bladder Scanning and Catheterization
Postvoid residual urine (PVR) measurement with a bladder scanning portable ultrasonographic device is an easy and non invasive method. Its use has been wide spread in men and women however its accuracy and reliability in children is still under debate. The aim of this study was to investigate the reliability of PVR measurement with real time bladder scanning in comparison with catheterization in children with voiding disorders. Postvoid residual urine measurements were routinely undertaken in patients to whom urodynamics were done, prospectively. Urinary catheterization was routinely done in all patients for cystometry. After uroflowmetry, residual urine was measured with a portable ultrasound device which readily measured the amount of PVR. After this measurement, bladder was emptied via the cystometry catheter and the drainage was noted. The age, sex and the diagnosis of the patients were also noted. The comparison between two measurements were done with paired sample t test. A total of 114 measurements were done in 89 patients. Mean age was 9±0,4 years (between 5 months to 21 years). There were 54 girls and 35 boys. The indication for urodynamics was nonneurogenic causes in 55 and neurogenic, in 34 patients. Mean PVR with ultrasonographic measurement was 56,6±6,6 ml and 56,7±7,4 ml with catheter. The difference between two measurements was statistically insignificant. Real time ultrasonographıc measurement with a bladder scanning device may be an easy, feasible, and reliable method to detect PVR in children with voiding disorders. This method may be preferred in appropriate indications like residual urine measurement in uroflowmetry+EMG studies where urinary catheterization is not necessary.
Özel ŞK1*, Tunç T2, Alataş İ3 and Güvenç Ü4
Istanbul, Turkey
Istanbul, Turkey, Tel: +90 5336279058; Email: keremozel@yahoo.com scanning in comparison with catheterization in children with voiding disorders.
test.
between two measurements was statistically insignificant.
urine measurement in uroflowmetry+EMG studies where urinary catheterization is not necessary.
Keywords: bladder dysfunction; bladder scan; post-void residual; children
Introduction
The initial evaluation of lower urinary tract dysfunction in children is comprised of history, physical examination, urinalysis, voiding diary, basic urodynamic tests such as uroflowmetry and/or electromyography and residual urine measurement. Postvoiding residual (PVR) urine measurement is an important part of this evaluation as elevated PVR may predict recurrent urinary tract infection in children [1]. PVR measurement is also important in the follow up of treatment success in nonneuropathic bladder dysfunction [2] and determination of incomplete emptying may make the indication of clean intermittent catheterization clear so that kidney functions can be protected in children with neuropathic bladder dysfunction [3]. PVR measurement can be successfully achieved with either urinary catheterization or ultrasonographic methods. Ultrasonographic PVR measurement was first described in 1967 but this method was first defined in children in 1976 [4, 5]. Although this method gained enthusiasm in late 80’s and well documented in adult studies, there are very limited information in pediatric practice. The aim of this study was to establish the practicability and accuracy of PVR measurement with portable ultrasonographic bladder scanning in comparison with urinary catheterization in a group of children with both neuropatic and nonneuropathic bladder dysfunction.
Patients and Methods
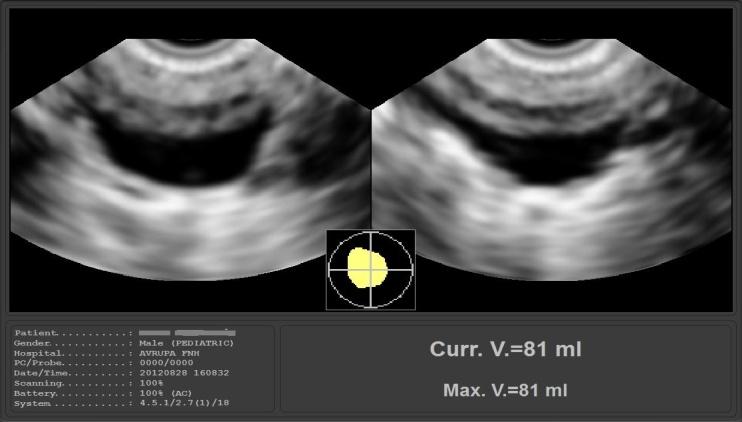
Patients who had indication for urodynamic study either for nonneurogenic or neurogenic bladder dysfunction were included in the study. PVR urine measurement was done after completion of voiding in nonneurogenic bladder dysfunction patients and after cessation of leaking in neurogenic group patients. For each measurement, at the end of the voiding phase during the urodynamic study, first PVR was measured with a portable USB ultrasonographic probe (Scanmaster®, MMS, USA)and PVR was calculated automatically with the computer software of the device (Figure 1). Correct positioning of the bladder was required for optimal volume measurement. Just after this measurement, PVR was again measured while the residual urine was withdrawed via the urodynamic catheter which was readily inserted for the urodynamic study. Thus the measurements are consecutive values reflecting the same actual PVR. Age, gender and the cause of bladder dysfuntion were also noted. Two groups of values were formed; Group 1, ultrasonographic PVR values and Group 2, PVR measured with urodynamic catheter. The values were first compared with paired samples t test and then the correlation between the two values were analyzed using Pearson correlation and R value of the correlation was found. p<0, 05 is considered to be statistically significant. A computer program (SPSS v.16) was used for the statistical analysis.
Results
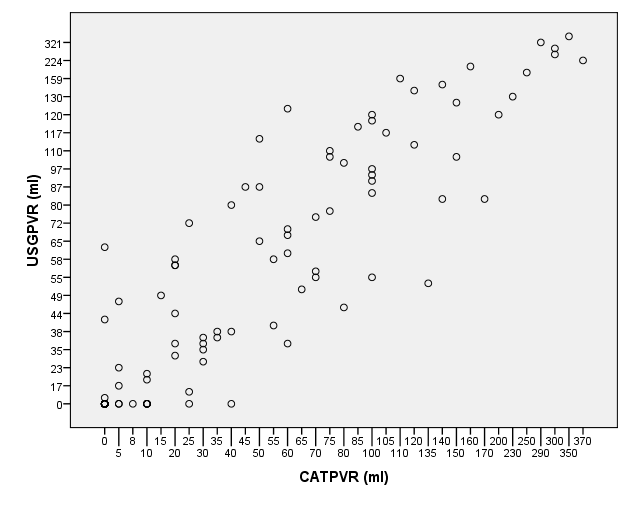
A total of 114 measurements were done in 89 patients. Mean age of the patients was 9±0,4 years (between 5 months and 21 years of age). There were 54 girls and 35 boys. The indication for urodynamics was nonneurogenic causes in 55 and neurogenic, in 34 patients. Mean PVR with ultrasonographic measurement was 56,6±6,6 ml and 56,7±7,4 ml with catheter (p=0,97). There was a direct correlation between ultrasonographic and conventional PVR measurement with catheter (R=0,916) (Figure 2).
Discussion
Complete bladder emptying is an important physiological activity in the genitourinary system. Bladder emptying can be affected due to pathologies of neurogenic or nonneurogenic origin. Elevated PVR may be a cause of urinary tract infection as well [1]. Incomplete emptying can be diagnosed with the detection of PVR. Ultrasonographic PVR determination was first described in 1967 [4]. This modality was reported in children in 1976 [5]. There is very limited information about the efficacy and accuracy of ultrasonograhic PVR measurement in children in the literature. Our current information comes mostly from adult studies. Pediatric studies were limited as the lowest limit of urine detected ultrasonograhically was shown to be approximately 42 ml in earlier studies [6]. Thus the reliability of ultrasonographic measurement in children may be regarded as a technical issue related with the bladder volume as anatomically pediatric bladder volume is lower than adult bladder volume. In most of the studies, ultrasonographic PVR measurement with an automated real-time calculation is found to be as affective as catheterization [7, 8, 9, 10]. However other studies found this modality to be limited and less accurate than catheterization [6, 11]. In the studies that are against the use of ultrasonographic PVR measurement, we see that conventional ultrasonograhy was used to measure PVR. In the studies that are in favor of this technique, bladder scanners specially designed for this purpose are observed to be used instead. Ultrasonography is operator dependant and bladder scanners may give a better and a more accurate calculation for PVR. In children however, as mentioned above, the experience is limited. After the initial reports, in 1989, Erasmie and Lidefelt showed that ultrasonograhic PVR measurement has a correlation value of R=0,96 when compared to catheterization in children [12, 13]. In 1990, Massagli et al. concluded, in their study with neurogenic bladder patients, that ultrasound scanner is as accurate as catheterization and is inexpensive and easy as well [14]. In 2009, Chang and Yang did a study about the normal values of PVR in healthy children. In their study, they measured the PVR ultrasonographically and found that a PVR value of over 20 ml to be more significant for the definition of abnormal PVR [15]. In this study, we measured the same PVR, one with an ultrasound bladder scanner and the other with a bladder catheter. As the same PVR was measured and compared, this method is a practical way to test the accuracy of the technique. We observed that almost the same values were found with the bladder scan and there was a high correlation between the two results. The graph of the results shows the linear correlation (Figure 2). These results are not age dependant or related with other factors like obesity or sedentery life and readily shows the accuracy of ultrasonographic measurement. The gender or the diagnosis of the patients are not regarded as a determinant factor for the results as correct measurement is purely related with the volume of PVR, only. In conclusion, real-time ultrasonographic measurement of PVR with a portable bladder scanning device is as accurate as catheterization in children. This technique is easy, feasible and reliable. It is also recommended to avoid the discomfort and risk of urinary tract infection as well as potential urethral injury due to urethral catheterization. This modality can also be preferred in children and can be safely used during clinical decision making.
References
-
Chang SJ, Tsai LP, Hsu CK, Yang SS (2015) Elevated postvoid residual urine volume predicting recurrence of urinary tract infections in toilet-trained children. Pediatr Nephrol 30(7): 1131-1137.
-
Kibar Y, Piskin M, Irkılata HC, Aydur E, Gok F, et al. (2010) Management of abnormal postvoid residual urine in children with dysfunctional voiding. Urology 75(6): 1472-1475.
-
Özel ŞK, Ulman I (2016) Contemporary urological management of spina bifida. J Pediatr Res 3(4): 168- 174.
-
Holmes JH (1967) Ultrasonic studies of the bladder. J Urol 97(4): 654-663.
-
Harrison NW, Parks C, Sherwood T (1976) Ultrasound assessment of residual urine in children. Brit J Urol 47(7): 805-814.
-
Mainprize TC, Drutz HP (1989) Accuracy of total bladder volume and residual urine measurements: comparison between real-time ultrasonography and catheterization. Am J Obstet Gynecol 160(4): 1013- 1016.
-
Al-Shaikh G, Larochelle A, Campbell CE, Schachter J, Baker K, et al. (2009) Accuracy of bladder scanning in the assessment of postvoid residual volume. J Obstet Gynecol Can 31(6): 526-532.
-
Choe JH, Lee JY, Lee KS (2007) Accuracy and precision of a new portable ultrasound scanner, the BME_150A, in residual urine volume measurement: a comparison with the Bladder Scan BVI 3000. Int Urogynecol J Pelvic Floor Dysfunct 18(6): 641-644.
-
Coombes GM, Millard RJ (1994) The accuracy of portable ultrasound scanning in the measurement of residual urine volume. J Urol 152 (6): 2083-2085.
-
Ding YY, Sahadevan S, Pang WS, Choo PW (1996) Clinical utility of a portable ultrasound scanner in the measurement of residual urine volume. Singapore Med J 37(4): 365-368.
-
Abdelwahab HA, Abdalla HM, Sherief MN, Ibrahim MB, Shamaa MA (2014) The reliability and reproducibility of ultrasonography for measuring the residual urine volume in men with lower urinary tract symptoms. Arab J Urol 12(4): 285-289.
-
Erasmie U, Lidefelt KJ (1989) Accuracy of ultrasonic assessment of residual urine in children. Pediatr Radiol 19(6-7): 388-390.
-
Lidefelt KJ, Erasmie U, Ballgren I (1989) Residual urine in children with acute cystitis and in healthy children: assessment by sonography. J Urol 141(4):916-917.
-
Massagli TL, Jaffe KM, Cardenas DD (1990) Ultrasound measurement of urine volume of children with neurogenic bladder. Dev Med Child Neurol 32(4): 314-318.
-
Chang SJ, Yang SS (2009) Variability, related factors and normal reference value of post-void residual urine in healthy kindergarteners. J Urol 184(4): 1933- 1938.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report