Coagulum, Tumor, Pyonephrosis?
Letter to Editor
Dear Sir, Pyonephrosis is the accumulation of pus in the renal pelvis and calyces [1, 2]. It represents a medical emergency and usually develops as a complication of infected hydronephrosis. If clinically suspected, pyonephrosis can be detected using imaging methods [ultrasound, computed tomography and/or MRI of the abdomen). The routine clinical-laboratory investigations point at severe inflammatory process (increased white blood cell count, ESR and CRP levels), impaired renal function [1, 2, 3]. The differential diagnosis should be made with coagulum, urotelioma, foreign body in the renal pelvis, hydronephrosis. The differential diagnosis in patients with inveterate hydronephrosis and pyonephrosis is very difficult due to the lack of typical clinical symptoms [fever, malaise, fatigue, flank pain] and acute inflammation markers and normal urine findings. Infrequently, no causative bacteria are isolated due to obstruction of the Therefore, the lack of acute inflammatory markers and the normal urine findings do not rule out the presence of pyonephrosis [1, 2]. In 2017 we admitted a 79 years-old female patient with erythrocyturia, leukocyturia and positive protein in the urine on dipsticks examination. The patients had no history of renal disease. At the admission the patient was in impaired general condition, subfebrile (37.20C). The routine clinical-laboratory investigations revealed mild anemia (Hb 119 g/l), normal ESR (24 mm/I h.) and moderate increase in CRP (80 mg/l), normal leukocyte count (7.6 G/l) with normal differential count, normal serum creatinine 81 mkmol/l), urinalysis: рН 5, specific gravity 1030, protein 3+, blood 2+, urinary sediment:
Letter to Editor
mass leukocytes. Urinary microbiological investigation: sterile. The abdominal ultrasound examination revealed normal image of the right kidney–112 mm, renal parenchymal zone 17 mm, several cortical calcifications. The left kidney was increased in size (figure 1) – 160 mm, parenchymal zone 8.8 mm, inveterate hydronephrosis 3 gr., 45 mm hyperechogenic formation in the renal pelvis showing no Doppler signals. The blood flow to the left kidney showed marked decrease on Doppler ultrasound. The presence of coagulum, pyonephrosis or tumor in the left renal pelvis at the background of inveterate hydronephrosis was suspected.
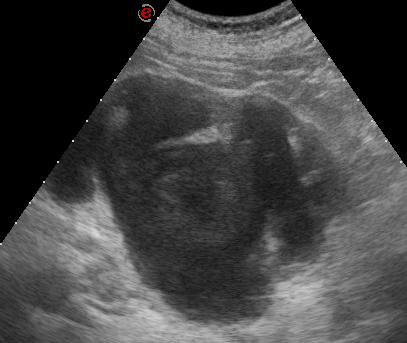
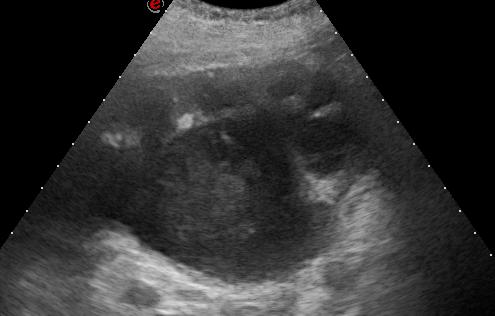

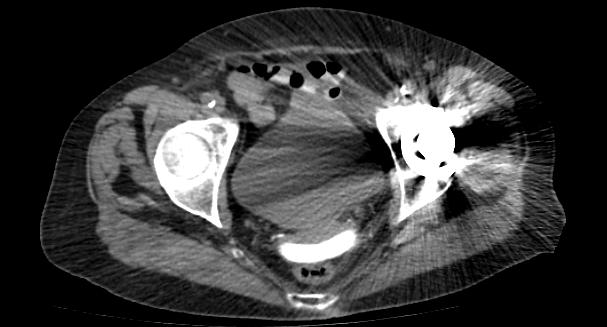
Figure 2: Abdominal ultrasound before (A) and after (B) antibacterial treatment, left kidney. Abdominal computed tomography (CT) was performed (figure 3): Native CT – left-sided hydronephrosis, vaginal pessary. On contrast-enhanced CT - the left kidney is significantly enlarged in size, with marked dilation of the renal pelvis and calyces, no excretion of contrast media

from the left kidney. Mild accumulation of the contrast media in the crtical zone of the left kidney. The coagulum in the pyeloureteral segment on ultrasound has migrated to the urinary bladder. The coagulum is mobile.

A. B.

C. D.
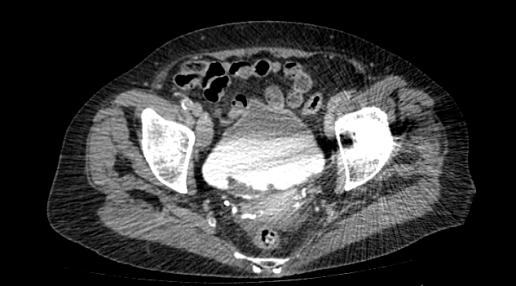
E. Figure 3: Contrast-enhanced abdominal CT. (A) Native scan – left-sided hydronephrosis. (B) Contrast-enhanced CT – left- sided hydromephosis, no excretion of the contrast medium by the left kidney, mild accumulation of the contrast medium in the cortex of the left kidney. (C) Intravaginal pessary. (D) and (E) Coagulum in the urinary bladder – mobile when body position is changed.
After the CT scan the patient was referred to Urology Clinic. The vaginal pessary was removed, Double J ureteral stent was inserted in the left pelvis and approximately 300 ml of purulent urine were evacuated. This clinical case demonstrates inveterate hydronephrosis due to intravaginal pessary causing obstruction of the left ureteral outflow. The left-sided hydronephrosis was complicated with pyonephrosis and coagulum. The patient lacked the typical clinical symptoms and laboratory markers characteristics of pyonephrosis due to the long duration of the condition. The differential diagnosis with coagulum and tumor was made using CT of the abdomen and during the urological intervention for desobstruction. We would like to emphasize that pyonephrosis could have protean clinical course wild mild or moderate increase of inflammatory markers and normal renal function and the lack of urinary abnormalities, especially in patients with long-standing inflamed hydronephrosis. Usually no causative bacteria are isolated due to obstruction of the urine flow.
References
-
Cox M, Momah I, Dong H, Selvarajan S (2005) Urinalysis in Pyonephrosis: does a normal result rule out pyonephrosis?. Austin J Radiol 2(5): 1030- 1032.
-
Yoder I, Pfister R, Lindofors K, Newhouse J (1983) Pyonephrosis: imaging and intervention. American Journal of Roentgenology 141: 735-740.
-
Androulakakis PA (1982) Pyonephrosis: a critical review of 131 cases. Br J Urol 54(2): 89-92.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report