Comparison of Safety and Efficacy of Exit Strategies Following Percutaneous Nephrolithotomy (PCNL) - A Prospective Randomised Study in a Tertiary Teaching Hospital
<p>Percutaneous Nephrolithotomy (PCNL) is the standard treatment for Renal Calculi more Than 2.5 cms. It involves getting access in to the renal Collecting System and then gradually the tract is dilated so that the Nephroscope can be passed in to the Collecting system to Break/remove the stones. After that various EXIT STRATEGIES are used to tamponade /drain the renal collecting system. Each exit strategy has its own pros and cons. Our Randomised, Prospective study is done to evaluate each exit strategy and to derive working guidelines in our Daily practice.</p>
Introduction
Fernström and Johansson were the first to describe a technique for extracting renal calculi through a percutaneous nephrostomy under radiological control in 1976 [1]. Wickham in 1979 described the staged approach starting with percutaneous nephrostomy under local anesthesia, followed by the dilatation of the tract serially over the next few days, with subsequent stone removal under general anesthesia using a rigid 30° cystoscope [2]. Percutaneous nephrolithotomy (PCNL) is the recommended treatment option for large or otherwise complex renal or proximal ureteral stones [3]. The standard PCNL procedure involves gaining an access to the kidney percutaneously through the flank on the side of the stone and patient in prone position. This is followed by creating a working tract connecting the flank surface with the intrarenal collecting system through which nephroscopy is performed. The stone is disintegrated and fragments are removed. A temporary drainage tube (nephrostomy tube- NT) is usually left in place at the end of the procedure to allow urinary drainage, tamponade of tract bleeding, and to maintain access to the collecting system. Routine placement of nephrostomy tube is debatable since 1997, when Bellman, et al. [4] first demonstrated that a ‘‘tubeless’’ PCNL, whereby the NT was replaced by a double-J stent, was associated with less postoperative pain, less analgesia requirement, shorter hospital stay, and faster return to normal activities. Several randomized controlled trials (RCTs) and their meta-analyses suggests that the tubeless approach reduces postoperative pain and hospital stay and that substituting double-J stents with external ureteral catheters or no drainage at all [totally tubeless (TTL further improves patients’ compliance by eliminating stent-related symptoms and need for cystoscopic removal [5, 6, 7, 8, 9]. On the other hand, other well-designed RCTs demonstrate advantages of early NT removal or placement of small-bore NTs over the tubeless approach [10]. The optimal exit strategy after PCNL remains controversial and debatable still. Various studies have shown advantages and complications of Various exit Strategies [11, 12].
Methodology
This prospective randomised study was conducted in the Department of Urology at MGMC&RI, Pondicherry from August 2014 to August 2016. All patients who gave consent to participate in the study and had renal calculi, PUJ calculi and large upper 1/3rd ureteric calculi were included in the study. Preoperatively, Patients with Congenital anomalies, Solitary kidney, compromised renal function, patients with partial and complete Staghorn calculi, infected systems, bleeding diathesis and Patients not giving consent for study were excluded from the study. Intraoperatively, Patients undergoing concomitant ureterolithotripsy, Patients with Intraoperative uncontrolled bleeding, major renal pelvic/Infundibular Injury and Patients with retained stone fragments in Kidney or Ureter were excluded from the study. Due Permission was obtained from Institutional Research Committee and Institutional Ethical Committee. Since there were no prior studies to guide the sample size, based on the approximate case load extrapolated from Medical records data, a period of 2 years or 120 cases whichever achieved earlier was considered as the end-point of the study. 120 Sealed covers were prepared before the start of the study and opened at the end of each procedure. However during the study period we could recruit only 102 patients. Out of 102 patients, 4 patients were excluded from the study on table as 3 patients developed Intraoperative bleeding and 1 patient developed Infundibular injury due to Infundibular stenosis. Thus 98 patients of whom 76 males and 22 females with an age range 19–79 years, with majority in age group of 31 to 40 years were included in the study. After careful selection, the patients were randomized into 3 Groups - Group A - Completely Tubeless PCNL (n=32), Group B - Tubeless with DJ stent (n=31) Group C - Tubeless with Ureteric catheter (n=35). Subjective and Objective assessment of the outcomes was done by assessing the Safety and Efficacy of the Exit Strategy. Subjective and Objective assessment of Safety was done by Clavien-Dindoscore (Appendix II). Efficacy was evaluated by Post-operative pain –VAS (Appendix I), Hospital stay and Time taken to revert to daily activities. All Patients were operated in the standard prone position and under General Anaesthesia. Size of Percutaneous tract dilatation was decided on table and depended on the size of the stone and the Infundibular diameter assessed by Dynamic RGP and Check Pyeloscopy.
| Tract dilatation | Scope used | Energy used | ||||||
| < 16 f | 8/9.8 f ureteroscope | Laser | ||||||
| 18 f | 15 f mini nephroscope | Laser | ||||||
| 24-26 f | 24 f nephroscope | Pneumatic lithoclast |
Inclusion Criteria: - Renal calculi, -PUJ calculi, -Upper 1/3rd ureteric calculi Exclusion Criteria: Preoperative:-
- Congenital anomalies
- Solitary kidney
- Compromised renal function
- Partial and Complete Stag horn Calculi
- Infected systems
- Bleeding diathesis Intraoperative:-
- Patients undergoing concomitant ureterolithotripsy
- Intra-operative uncontrolled bleeding
- Major Pelvic/ Infundibular injury
- Patients with retained stone-fragments in kidney or ureter
Method of Randomization
• Sealed envelopes were prepared at the start of study using a computer generated table of random numbers by Department personnel not involved in the study and kept under the custody of Departmental Head.
- Sealed envelopes were created for 102 patients entering the serial number on the top of each envelope and the treatment arm inside the envelope.
- After enrolling the patient into the study, patient was allotted a serial number. Sealed envelope was opened after the completion of PCNL and before the Exit Strategy to allocate the patient to the treatment group.
- Patients Underwent following Exit Procedures: - Group A - underwent Completely tubeless PCNL - Group B - underwent Tubeless PCNL with DJ stent - Group C - underwent Tubeless PCNL with Ureteric catheter.
- This method ensured that there was no bias in selecting the exit strategy.
Study Parameters
1) Pre-Operative Investigation (A) Routine Pre-operative Laboratory Investigations-
- Complete blood count (Haemoglobin, Total counts, Differential counts),
- Renal function tests,
- Urine routine, microscopy and culture/ sensitivity,
- Prothrombintime, Activated partial thromboplastin time,
- Bleeding and clotting time,
- Blood sugar,
- Blood grouping and Rh compatibility
- Serum electrolytes, (B) Radiological Investigations-
- X-RAY of Kidney, Ureter, Bladder
- Intravenous Urogram
- Non Contrast Computerized Tomography of Kidney, Ureter, Bladder
- Ultrasonography of Kidney, Ureter, Bladder 2) Treatment Modality
- PCNL 3) Exit Strategy A) Completely Tubeless - Group A B) Tubeless With DJStent -Group B C) Tubeless With Ureteric Catheter - Group C
Outcomes of Treatment Comparing Safety and Efficacy of Exit Strategies
1) Post-operative pain (Visual Analogue Score- VAS) 2) Complications evaluated by Clavien-Dindo scoring system 3) Time taken to revert to daily activities 4) Hospital stay.
Investigations
All the patients underwent routine Laboratory investigations - Haematological, Biochemical, Urine and Radiological investigations - X-RAY Kidney Ureter Bladder and Ultrasound Kidney Ureter Bladder. Non Contrast Computed Tomography (NCCT) Kidney Ureter Bladder and Intravenous Urography (IVU). Post operatively; all patients underwent X-Ray of Kidney, Ureter, Bladder region on post-operative day 1 and Ultrasound of Kidney, Ureter and bladder region on post-operative day 2.
Procedure of PCNL
- The Procedure was usually done under general anaesthesia under fluoroscopic guidance.
- Ureteric catheter was passed and retrograde Pyelography was done in lithotomy position for initial assessment.
- 16F Foleys catheter was placed in the urinary bladder.
- Patient was then turned to prone position.
- Targeted calyx was accessed either by subcostal or supracostal approach (depending on location of calculus) by bulls eye or triangulation technique.
- Tract was dilated up to 14-26 F with Teflon dilators (Figure 11) or metal dilators (Figure 12).
- Size of tract dilatation was decided by size of calculus and infundibular diameter measured by Dynamic RGP and Check Pyeloscopy..
- Nephroscope was passed to survey the kidney and the calculus.
- Calculus fragmented using pneumatic lithoclast/laser and fragments evacuated.
- Nephrostomy tube was not placed in any of the cases’
- In Patients selected under Group A – Totally Tubeless PCNL was performed, Patients selected under Group B underwent Tubeless PCNL with DJ stent and Patients selected under Group C underwent Tubeless PCNL with Ureteric catheter.
- The distal end of the Ureteric catheter was secured inside the Foleys catheter by “Blitz technique” so as to maintain sterile drainage.
- Post operatively, DJ stent was removed on Post op day
7 and Ureteric catheter was removed on Post op day 1- 2. • Post operatively, X-ray KUB (Post-operative day 1) and USG KUB (Post-operative day 2) were performed to assess stone free status and rule out complications.
Post-Operative Analgesia
Post operatively all patients received a standard parenteral non-opioid analgesics on demand which was Diclofenac Sodium. The frequency of Analgesic requirements i.e. 4th hourly or 6th hourly was recorded.
Statistical Analysis
The data was first entered into an excel file and then exported into IBM SPSS 21.0 version. The analyses presented in this study were carried out using IBM SPSS software. Data cleaning process such as missing data, outlier’s detection and logical checks were performed at first level. The accuracy of the data was checked by proof reading the item in the questionnaire against the SPSS data window. In order to meet the objectives of the study, the statistical techniques like cross tabulations, Chi square test, ANOVA & Post Hoc Test were used. The significance level for all tests was set at p<0.05.
Results
Out of 98 patients, 32 (32.65%) underwent Completely
Tubeless PCNL, 31 (31.63%) underwent Tubeless with DJ stent and 35 (35.71%) underwent Tubeless with Ureteric catheter.
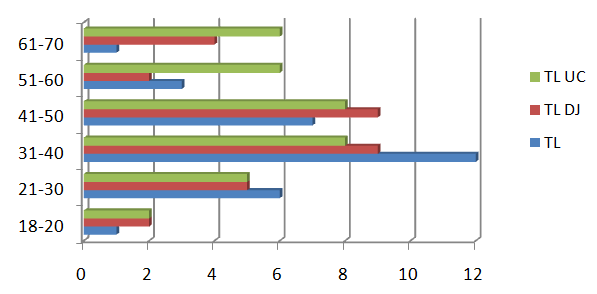
| Age | Group A (Completely Tubeless) (N=32) | Group B (Tubeless With DJ Stent)(N=31) | Group C (Tubeless With Ureteric Catheter)(N=35) | |||
| Age | Male | Female | Male | Female | Male | Female |
| 18-20 | 1 | 0 | 2 | 0 | 2 | 0 |
| 21-30 | 5 | 1 | 5 | 0 | 4 | 1 |
| 31-40 | 7 | 5 | 5 | 4 | 6 | 2 |
| 41-50 | 4 | 3 | 7 | 2 | 8 | 0 |
| 51-60 | 2 | 1 | 2 | 0 | 6 | 0 |
| 61-70 | 0 | 1 | 3 | 1 | 5 | 1 |
| 71-80 | 2 | 0 | 0 | 0 | 0 | 0 |
Table 2: Age Group.
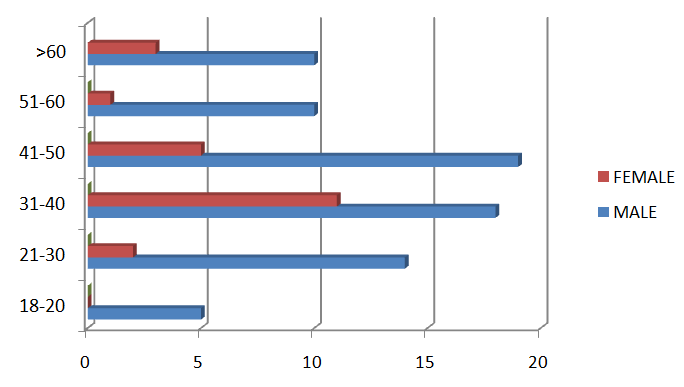
b) The Gender distribution observed as follows, 76 (77.55%) Males 22 (22.44%) females (Figure 2)
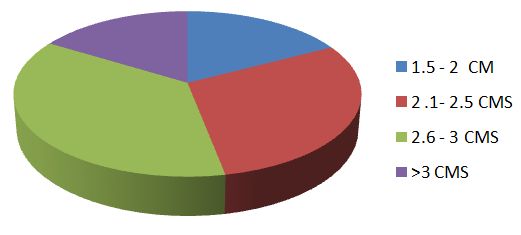
| Stone Size (Cms) | Number |
|---|---|
| 1.5-2 CM | 17 |
| 2.1-2.5 CM | 29 |
| 2.6-3 CM | 36 |
| >3 CM | 16 |
Table 3: Stone Size.
c) Majority of calculi were in the range of 2-3 centimetres. The maximum stone size was 3.8 cm. Stone size was measured with Ultrasound and NCCT KUB- (Table II and Figure 3).
Complications Score
Group A (Completely Tubeless Group)
- 5 patients had Clavien-Dindo Grade 2-3A complications whereas no significant complications were observed in other groups. - Post operatively, 1 patient in completely tubeless group required DJ stenting and peri-nephric drain placement for sepsis and peri-nephric collection (CD 3A), - 1 patient required Ureteroscopy for calculus fragment which had migrated to the ureter (CD 3A). - 1 patient had significant haemorrhage requiring blood transfusion (CD 2) - 2 patients developed post-operative fever and sepsisrequiring higher IV Antibiotics (CD 2).
| Group A | No of Patients With Complications | Description | Complication | CD Grade(2/3) |
|---|---|---|---|---|
| Completely Tubeless | 2 Patients | 40/Male, Left Upper Pole Calculus With 18f Dilatation | Post-Operative Sepsis And Perinephric Collection | CD 3a Requiring DJ Stenting And Perinephric Drain |
| Completely Tubeless | 2 Patients | 33/Female, Lt Renal Pelvic Calculus With 26 F Dilatation | Retained Calculus – Ureter | URSL |
| Completely Tubeless | 1 Patient | 36/Female, Right Lower Pole Calculus With 26 F Dilatation | Hemorrhage | CD 2 Requiring Blood Transfusion |
| 2 Patients | 31/Female, Left Lower Pole, 18 F Dilatation | Post-Operative Sepsis | CD 2 Controlled With Higher Antibiotics – (Impanel) | |
| 2 Patients | 50/Male, Left Pelvic | Post-Operative Sepsis | CD 2 Controlled With Higher Antibiotics – (Impanel) |
Table 5: Complications – Group A.
Group B: Tubeless with DJ Stent Group
1 patient had postoperative sepsis (CD 2) which was controlled with higher IV Antibiotics (Imipenem).
| No of Patients With Complications | Complication | CD Grade(2/3) | |
|---|---|---|---|
| Tubeless With DJ Stent | 1 | 62/Male, Left Lower Pole 18 F Dilatation Post-Operative Higher Antibiotics For Sepsis (Imipenem) | 2 |
Table 7: Patient’s Complications in Group B.
Group C: Tubeless with Ureteric catheter
None of the patients had CD 2/3 Complications.
| Group C | No of Patients With Complications | Complication | CD |
|---|---|---|---|
| Group C | Grade(2/3) | ||
| Tubeless With Ureteric Catheter | 0 | Nil | - |
Table 6: Patient’s Complications in Group C.
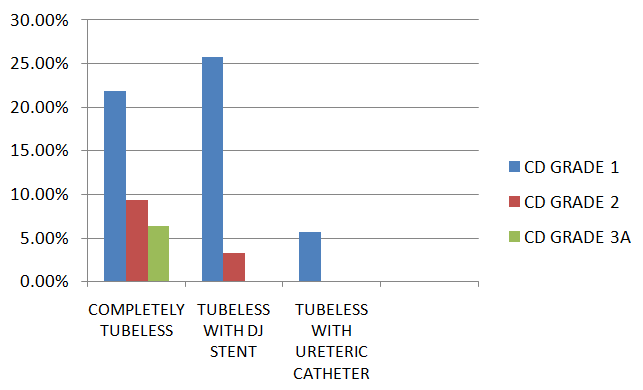
| Complications | Total | ||||||
|---|---|---|---|---|---|---|---|
| CD GRADE 1 | CD GRADE 2 | CD GRADE 3A | NIL | ||||
| Exit Strategy | CT | Count | 7 | 3 | 2 | 20 | 32 |
| Exit Strategy | CT | % within EXIT_STRATEGY | 21.90% | 9.40% | 6.30% | 62.50% | 100.00% |
| Exit Strategy | TDJ | Count | 8 | 1 | 0 | 22 | 31 |
| Exit Strategy | TDJ | % within EXIT_STRATEGY | 25.80% | 3.20% | 0.00% | 71.00% | 100.00% |
| Exit Strategy | TUC | Count | 2 | 0 | 0 | 33 | 35 |
| % within EXIT_STRATEGY | TUC | 5.70% | 0.00% | 0.00% | 94.30% | 100.00% | |
| Total | Count | 17 | 4 | 2 | 75 | 98 | |
| Total | % within | 17.30% | 4.10% | 2.00% | 76.50% | 100.00% | |
| Total | EXIT_STRATEGY | 17.30% | 4.10% | 2.00% | 76.50% | 100.00% | |
Crosstab
| Value | df | Asymp. Sig. (2-sided) | |
| Pearson Chi-Square | 14.583^{a}$ | 6 | .024 |
| Likelihood Ratio | 16.505 | 6 | .011 |
| N of Valid Cases | 98 |
Chi-Square Test
a. 6 cells (50.0%) have expected count less than 5. The minimum expected count is 63. When we compared the complications among all three Groups, it was found to be statistically significant (p value = 0.024) which means that, use of any kind of exit strategy there always exists some sort of complications and it is mostly noticed as CD grade 1. However, the overall complications were least in Group C (Tubeless with Ureteric catheter). Pain Score- Majority of the patients had Pain scores by VAS in range of 5-8. The chi-square statistic is 3.3997. The p-value is 0.4933. The result is not significant at p <0.05.
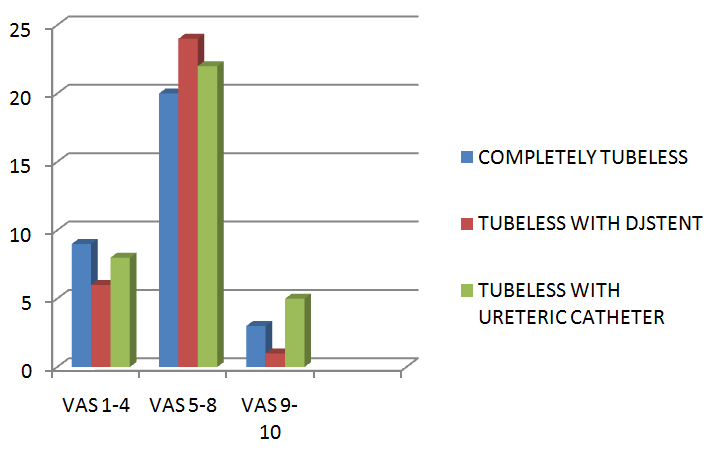
| VAS | Completely Tubeless | Tubeless With DJ Stent | Tubeless With Ureteric Catheter |
|---|---|---|---|
| 4-Jan | 9 (7.51)[0.30] | 6 (7.28)[0.22] | 8 (8.21)[0.01] |
| 8-May | 20 (21.55)[0.11] | 24 (20.88)[0.47] | 22 (23.57)[0.10] |
| 10-Sep | 3 (2.94)[0.00] | 1 (2.85)[1.20] | 5 (3.21)[0.99] |
| 32 | 31 | 35 |
Table 10: Post Operative Vas.
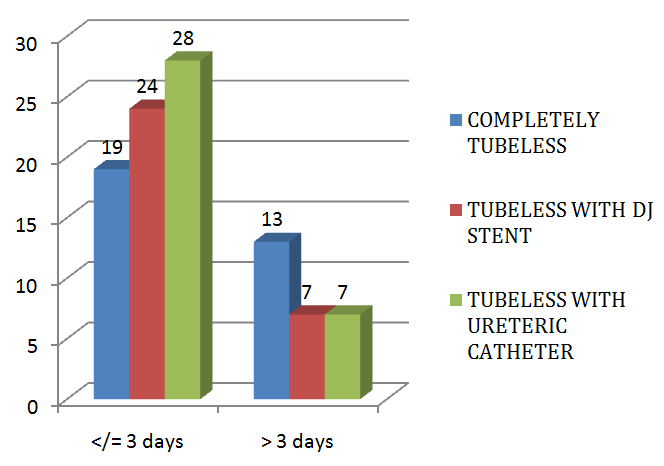
| Group | Number Of Days | Row Totals | |
|---|---|---|---|
| =< 3 Days | > 3 Days | ||
| CT | 19 (23.18)[0.75] | 13 (8.82)[1.99] | 32 |
| TDJ | 24 (22.46)[0.11] | 7 (8.54)[0.28] | 31 |
| TUC | 28 (25.36)[0.28] | 7 (9.64)[0.72] | 35 |
| Column Totals | 71 | 27 | 98 |
Table 11: Duration of Hospital Stay.
Table 7: Duration of Hospital Stay. The Time Taken To Return to Daily Activities: The time taken to return to daily activities was highest in Tubeless with DJ stent group followed by Completely Tubeless Group. The return to daily activities was fastest in Tubeless with Ureteric catheter Group. The chi-square statistic is 19.0869. The p-value is 0.000072. The result is significant at p < 0.05
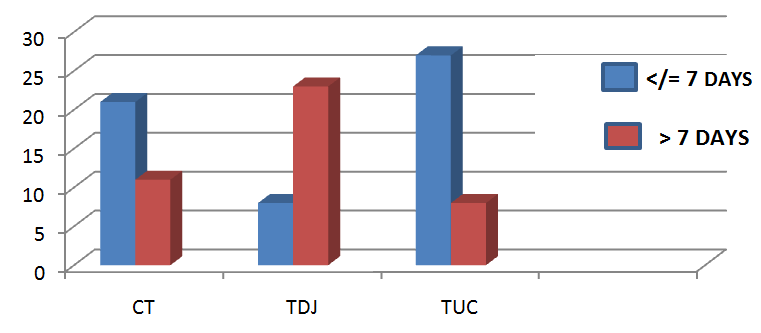
| Time Taken | Row Totals | ||
|---|---|---|---|
| Group | </= 7 Days > 7 Days | ||
| CT | 21 (18.29) [0.40] | 11 (13.71) [0.54] | 32 |
| TDJ | 8 (17.71) [5.33] | 23 (13.29) [7.10] | 31 |
| TUC | 27 (20.00) [2.45] | 8 (15.00) [3.27] | 35 |
| Column Totals | 56 | 42 | 98 (Grand Total) |
Table 13: Time Taken To Return to Daily Activities.
| Group | Stone Free | Not Stone Free | Row Totals |
|---|---|---|---|
| Ct | 31 | 1 | 32 |
| Tdj | 31 | 0 | 31 |
| Tuc | 35 | 0 | 35 |
| Column Totals | 97 | 1 | 98 (Grand Total) |
Table 12: Efficacy of the Procedure.
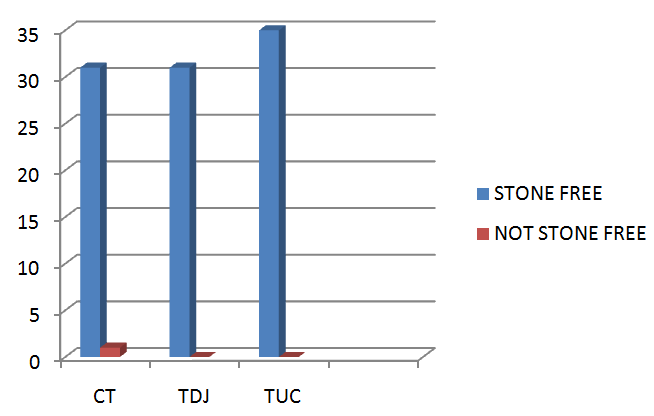
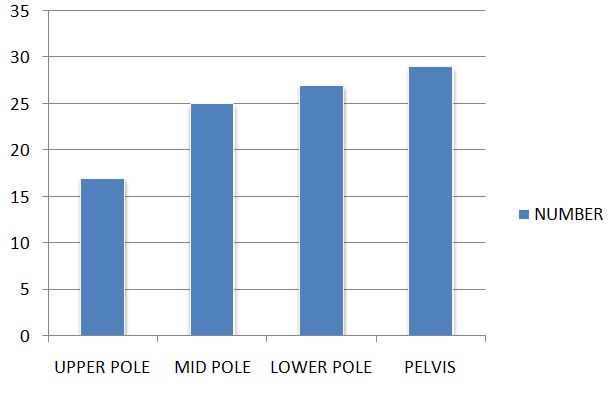
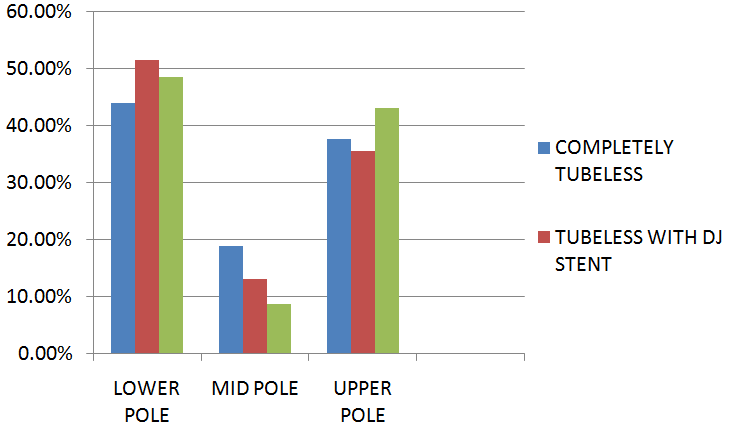
Figure10: Puncture Site.
| Puncture Site | Total | |||||
|---|---|---|---|---|---|---|
| Lower Pole | Mid Pole | Upper Pole | ||||
| Exit strategy | CT | Count | 14 | 6 | 12 | 32 |
| Exit strategy | CT | % within EXIT_STRATEGY | 43.80% | 18.80% | 37.50% | 100.00% |
| Exit strategy | TDJ | Count | 16 | 4 | 11 | 31 |
| Exit strategy | TDJ | % within EXIT_STRATEGY | 51.60% | 12.90% | 35.50% | 100.00% |
| Exit strategy | TUC | Count | 17 | 3 | 15 | 35 |
| Exit strategy | TUC | % within EXIT_STRATEGY | 48.60% | 8.60% | 42.90% | 100.00% |
| Total | Count | 47 | 13 | 38 | 98 | |
| Total | % within EXIT_STRATEGY | 48.00% | 13.30% | 38.80% | 100.00% | |
Value df Asymp. Sig. (2-sided)
Pearson Chi-Square 1.768a 4 0.778
Likelihood Ratio 1.768 4 0.778
N of Valid Cases 98
Chi-Square Tests
On comparing the Puncture site between the three Groups A, B&C, it was found to be not significant. Observationally, around 45-50% of cases were witnessed in lower pole puncture site and proportionately more in TUC strategy under Lower pole puncture site.
| Groups | N | Mean | Std. Deviation | ANOVA (F-value and p-value) | |
|---|---|---|---|---|---|
| Hospital Stay | A | 32 | 3.31a | 1.091 | 4.037 (0.021*) |
| Hospital Stay | B | 31 | 2.84a | .898 | 4.037 (0.021*) |
| Hospital Stay | C | 35 | 2.69b,a | .796 | 4.037 (0.021*) |
| Post Operative Pain Scores | A | 32 | 5.34a | 1.677 | 0.607 (0.547NS) |
| Post Operative Pain Scores | B | 31 | 5.71a | 1.419 | 0.607 (0.547NS) |
| Post Operative Pain Scores | C | 35 | 5.80a | 2.112 | 0.607 (0.547NS) |
| Time To Revert To Daily Activities | A | 32 | 6.41a | 1.739 | 24.107 (0.000*) |
| Time To Revert To Daily Activities | B | 31 | 8.16b | 1.344 | 24.107 (0.000*) |
| Time To Revert To Daily Activities | C | 35 | 5.06c | 2.209 | 24.107 (0.000*) |
Table 15: Analysis of Variance between Hospital stay, Post-operative Pain Scores and Time to revert to daily activities. "*" repre
Table 16: Analysis of Variance between Hospital stay, Post-operative Pain Scores and Time to revert to daily activities. "*" represents significance and "NS" represents Not Significance at 0.05 level. Same superscript does not differ and different superscripts differ significantly. Group A - Completely Tubeless Group B- Tubeless With Dj Stent Group C- Tubeless With Ureteric Catheter On performing ANOVA (Analysis of variance), - The comparison of Hospital stay between three groups was statistically significant. - Comparison of Time taken to revert to daily activities was statistically significant. - Comparison of Post-operative pain scores between three groups was not statistically significant. On performing the Post Hoc Tests, when we compared the Duration of Hospital stay between the three Groups, it was evident that the comparison between Group A and Group C was statistically significant with p= .022 On comparing the Post-operative Pain Scores between the three Groups A, B & C, it was found to be not significant.
On comparing the time taken to revert to daily activities between the three Groups, it was found to be significant between all three Groups with p value less than .05
Discussion
Past decade, has seen the concept of foregoing NT placement after PCNL in practice with the intent of reducing some postoperative problems like discomfort, urinary leakage from the percutaneous tract, and longer hospital stay. Many RCTs have demonstrated the efficacy and safety of tubeless PCNL. This is a safe alternative to NT placement in uncomplicated cases. In the present study, operating time and postoperative hospital stay were both significantly shorter for patients receiving the less invasive stent only exit compared with the more invasive NT. This is a valid finding that will make urologists to choose one exit strategy instead of the other. Our results therefore confirm that shorter hospital stay is indeed an advantage of less invasive exit strategies.
Conclusions
Patients who undergo PCNL and with less invasive exit strategy have shorter hospital stay than those who have postoperative NT. The main Predictor of Complications is INTRA-OPERATIVE and not the exit strategy adopted. The choice of exit strategy should be based on intraoperative course of the PCNL.
References
-
Fernström I, Johansson B (1976) Percutaneous pyelolithotomy. A new extraction technique. Scand J Urol Nephrol 10(3): 257-259.
-
Wickham JE, Kellett MJ (1981) Percutaneous nephrolithotomy. Br J Urol 53(4): 297-299.
-
Lingeman JE, lifshitz DA, Evan AP (2002) Surgical management of urinary lithiasis. In: Walsh PC, Retick AB, Vahghan ED, Campbell’s Urology.
-
Bellman GC, Davidoff R, Candela J, Gerspach J, Kurtz S, et al. (1997) Tubeless percutaneous renal surgery. J Urol 157(5): 1578-1582.
-
Shah HN, Kausik VB, Hegde SS, Shah JN, Bansal MB (2005) Tubeless percutaneous nephrolithotomy: a prospective feasibility study and review of previous reports. BJU Int 96(6): 879-883.
-
Beiko D, Lee L (2010) Outpatient tubeless percutaneous nephrolithotomy: the initial case series. Can Urol Assoc J 4(4): E86-E90.
-
Agrawal MS, Agrawal M (2010) Tubeless percutaneous nephrolithotomy. Indian J Urol 26(1): 16-24.
-
Amer T, Ahmed K, Bultitude M, Khan S, Kumar P (2012) Standard versus tubeless percutaneous nephrolithotomy: a systematic review. Urologia Internationalis 88(4): 373-382.
-
Sebaey A, Khalil MM, Soliman T, Mohey A, Elshaer W, et al. (2016) Standard versus tubeless mini- percutaneous nephrolithotomy: A randomised controlled trial. Arab Journal of Urology 14(1): 18-23.
-
Wright A, Rukin N, Smith D, De la Rosette J, Somani BK (2016) “Mini, ultra, micro” – nomenclature and cost of these new minimally invasive percutaneous nephrolithotomy (PCNL) techniques. Ther Adv Urol 8(2): 142-146.
-
de la Rosette J, Assimos D, Desai M, Gutierrez J, Lingeman J, et al. (2011) The Clinical Research Office of the Endourological Society percutaneous nephrolithotomy global study: indications, complications and out comes in 5803 patients. J Endourol 25(1): 11-17.
-
Labate G, Modi P, Timoney A, Cormio L, Zhang X, et al. (2011) The percutaneous nephrolithotomy global study: classification of complications. J Endourol 25(8): 1275-1280.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report