Decrease in Quality of Life and Functional Assessment in Elder Patients with End-Stage Renal Disease after Two Years of Hemodialysis Therapy
Introduction: Hemodialysis improves survival rates of Chronic Kidney Disease (CKD) patients but not Quality of Life (QoL) which decreases in a more aggressive way in the elderly population. We describe the reduction and impact in QoL and functional assessment at 6 months, 1 and 2-years of treatment in hemodialysis. Methods: We performed a single center prospective study, applying the Kidney Disease Quality of Life (KDOQOL-36 TM) in Spanish, Katz Index, Barthel Index, Lawton and Brody Scale and Karnofsky Performance Status to patients with CKD KDIGO 5D, aged 65 years or older at our hemodialysis center on October 2016. During the study, patients received hemodialytic and pharmacological treatment. We applied the surveys again on May 2017, October 2017 and October 2018 to the same population. Results were presented using mean and standard deviation and were analyzed using a Student’s t-test. Results: At the beginning of the study 22 elder patients in hemodialysis were included, 59% of them were men with an average age of 72.9 (±5.9) years, and an average time in hemodialysis of 27.1 (±24.1) months. After a two-year follow up 36% of the patients died, 9% changed their residency and 55% remained active at our center. We compared the media of each subscale after six months, one and two years with Student’s t-test, finding a significant decrease only at the 2-years evaluation in Effects and Burden of kidney disease subscales compared with the previous ones (p
Introduction
Chronic Kidney Disease (CKD) is a global public health problem with high morbidity and mortality [1]. In Mexico it has progressed as a cause of mortality and frequently appears as a comorbidity accompanying other causes of death [2]. The epidemiologic changes of the population modify the panorama of this disease; the number el adults over 65 is increasing worldwide, [3] in addition, these patients have a higher prevalence of diabetes mellitus or hypertension, which are the most common causes of CKD [4]. Other studies such as the BEST Kidney Collaboration Study had a median age of patients with Acute Renal Failure of 67 years [5] and in the REIN registry where ~40% of the incident dialysis patients were older than 75 years [6]. As the general population ages, the susceptibility for the development of renal alteration increases, with the consequent increases in cost for health-systems (4), especially in patients that require Renal Replacement Therapy [7].
For elderly patients reaching end-stage renal disease (ESRD) there are different outcomes and therapeutic options [8]. Specifically in this group, RRT can improve survival rates, but not necessarily Quality-of-Life (QoL); which needs to be considered by the poor prognosis that confers starting dialysis [9, 10].
QoL evaluation has become an independent predictor for clinic targets and quality indicator for therapies and results, especially in ESRD patients [11, 12]. With the future ESRD incidence in mind and the scarce parameters for this vulnerable population, we decided to describe the reduction in QoL and functional assessment in elderly patients during a 2-year follow-up in hemodialysis.
Methods
We performed a single center prospective study at the Hemodialysis Unit at the Hospital Central Sur de Alta Especialidad PEMEX (Mexico City). We included patients with CKD KDIGO 5D who were in the chronic hemodialysis program, aged 65 years or older, who were able to answer the interviewer and excluded those who were disabled and could not answer the survey. In October 2016 an interviewer applied the Kidney Disease Quality of Life (KDOQOL-36 TM) in Spanish verbally, and the Functional Assessment (FA) panel which consisted of the Katz Index, Barthel Index, Lawton and Brody Scale and Karnofsky Performance Status.
The same surveys were applied again on May 2017, October 2017 and October 2018 to the same patients that were still at the hemodialysis center. During the two years of follow-up the patients received dialytic and pharmacological treatment according to the KDIGO guidelines.
For the Katz Index we presented the information using a percentage of the best score (A) and for the subscales of KDOQOL-36TM and for the rest of the FA panel we used mean values with Standard Deviation (SD). We compared the 4 measurements done for each scale with t-Student test and P values <0.05 were considered statistically significant. SPSS software (version 20.0) was used to compare results.
Results
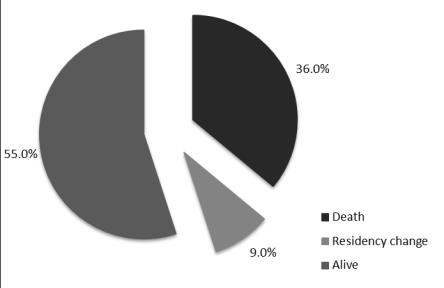
At the beginning of the study 22 elder patients in hemodialysis were included with an average age of 72.9 (+5.9) years, 59% of were men with an average time on hemodialysis of 27.1 (+24.1) months. After a two-year follow up 36% of the patients died, 9% changed their residency and 55% remained active at our center (Figure 1).
In this group of patients 66.6% were men and had an average age of 72.0 (+2.8) years.
Mean values from KDOQOL-36TM subscales and FA panel at baseline, 6-months, 1-year and 2-year are presented in Table 1 & Figures 2,3 respectively.
| Basal | 6 Months | 1 Year | 2 Years | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Scale | ||||||||||||||
| Mean (SD) / Mode | Mean (SD) / Mode | Mean (SD) / Mode | Mean (SD) / Mode | |||||||||||
| Symptom/problem list | 84.6 (±10.5) | 80.4 (±17.2) | 79.2 (±17.2) | 81.8 (±1.3) | ||||||||||
| Effects of kidney disease | 84.9 (±17.9) | 75.2 (±23.6) | 70.1 (±27.6) | 40.6 (±15.6) | ||||||||||
| Burden of kidney disease | 61.6 (±25.6) | 49.2 (±18.4) | 52.2 (±30.0) | 22.4 (±10.8) | ||||||||||
| SF-12 Physical Composite | 41.5 (±8.7) | 39.1 (±8.4) | 39.2 (±8.3) | 38.3 (±6.8) | ||||||||||
| SF-12 Mental Composite | 49.8 (±11) | 45.7 (±12.1) | 47.1 (±13.4) | 43.4 (±4.7) | ||||||||||
| Karnofsky Performance Status | 78.6 (±17.2) | 76.2 (±16.2) | 77.1 (±16.4) | 76.7 (±15.6) | ||||||||||
| Barthel Index | 85.2 (±18.8) | 80.9 (±17.9) | 87.9 (±11.7) | 84.6 (±20.4) | ||||||||||
| Katz Index | A (77%) | A (62%) | A (78%) | A (58%) | ||||||||||
| Lawton and Brody Scale | 5.1 (±2.7) | 5.0 (±3.0) | 6.4 (±2.0) | 6.3 (±1.6) |
Table 1: Mean values from KDOQOL-36TM Scale and Functional Assessment Panel.
SD: Standard Deviation Table 1: Mean values from KDOQOL-36TM Scale and Functional Assessment Panel.
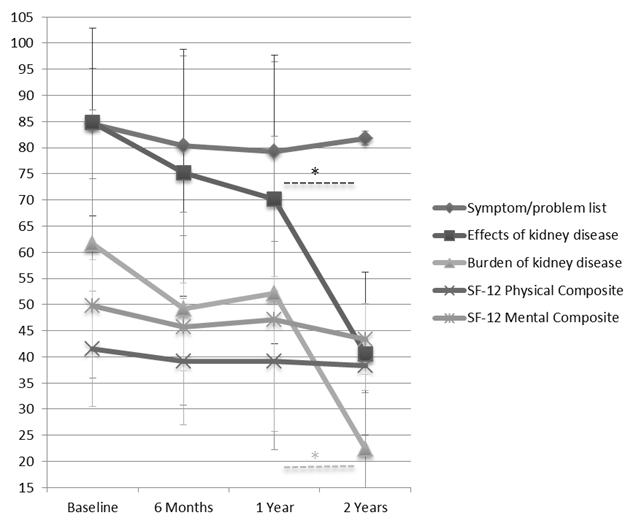
(* p<0.01) Effects and Burden of kidney disease subscales Figure 2: Mean values from KDOQOL-36TM Scale.
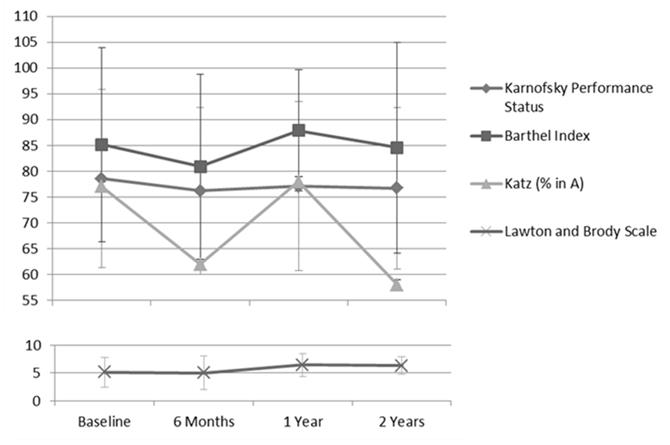
We compared the media of each subscale and FA panel finding a significant decrease only at the 2-year evaluation in Effects and Burden of kidney disease subscales of KDOQOL-36TM, (p<0.01) but no difference was found in the rest of subscales or the FA panel.
Discussion
Multiple studies have shown that ESRD and its treatment produce a negative impact in the QoL of patients. QoL is a construct based on the perception of each patient on how the disease or treatment allows them to have a satisfactory life, and is a concept that is acquiring relevance as a quality indicator of treatments in different fields [13]. The KDOQOL-SF36TM is the disease- specific QoL questionnaire that is widely used in clinical settings as well as in several studies for CKD, [14] it was adapted and validated in Mexico by Dehesa-López, et al. [15] allowing us to use this questionnaire reliably for this study.
Patients with ESRD have consistently had a lower QoL than the general population [16]. We confirmed this observation by comparing the results we obtained from the Physical and Mental Composite with the geriatric population reported in the Quality of Life Mexican normative standard, [17] observing a significant reduction in QoL in our population.
The study published by Dehesa-López in 2017 also reported QoL in a Mexican hemodialysis population, it had a younger population (median age of 55 years) as compared to our study, however it shared similar results regarding the Symptom/ Problem list, Physical and Mental Composite subscales being similar in all 4 measurements, with a small reduction during the time of follow up. On the Effects and Burden of Kidney Disease subscales the first measurement was higher in our study, similar at 6 months and at the first year, but it was lower at the second year, being the most affected areas in the QoL by hemodialysis. In our study, the decrease in the scores was not as pronounced as expected, a possible explanation is because the patients that died had probably the lowest values, and the patients that were able to complete the study had higher scores at the beginning.
Our study shows the fall in QoL with hemodialysis treatment, however it is important to note that in order to make a proper comparison with other populations or with treatment efficacy we would need to evaluate other factors such as comorbidities, treatment data, among other factors that allows to objectively evaluate and correlate with other markers as shown in other papers [18].
We also made the evaluation of FA panel, this shows a gradual decrease for the evaluated activities; nevertheless we should seek to evaluate the condition of the elderly in a multidimensional and clinical pathway as the fragility syndrome. Frailty has been reported in about 30% of patients with ESRD [19] and is associated with increased risk of fall, fractures, and mortality [20].
In a systematic review there were no difference on QoL by the modality of dialysis (either hemodialysis or peritoneal dialysis), but we should be cautious in translating our information to peritoneal dialysis because the needs and response to treatment vary between patients and modality.
In the cultural environment in which we develop, we often neglect the QoL. At an interview exploring palliative care, although most Latinos wanted to discuss their QoL, symptom management, prognosis and end-of-life care, few reported a previous end-of-life conversation with their nephrologist [21]. It is important that we begin to establish communication links with these patients so that the QoL effectively becomes a quality indicator of the given treatment.
The poor prognosis that CKD confers to elder people, confirms the need to consider other perspectives such as QoL and patients’ end-of life wishes. We could open the debate around the ideal treatment for this specific population, which is not the object of this study, but the reality is that we will see the aging of the hemodialysis population, specifically in countries like ours.
The limitations for this study are the small population and that it was obtained from one single hemodialysis center, that it is not representative of the elder Mexican population. Another important limitation comes from the fact that we do not know the bias of applying the same survey.
Conclusion
Rayner’s editorial starts with this sentence: “Wise clinicians know the value of asking the right question” [22]. Therefore it is important that we take a minute to ask and asess if the hemodialysis we are offering is being effective and improving the conditions of the elderly patient, or on the contrary we are prolonging life in unfavorable conditions. In this study we show a decrease in all subscales of KDOQOL-36TM and functional assessment evaluation with statistical difference in the Effects and Burden of kidney disease subscales at the second year in elder patients, and we urge to continue studying this growing specific population.
References
-
Jha V, García-García G, Iseki K, Li Z, Naicker S, et al. (2013) Chronic kidney disease: global dimension and perspective. Lancet 382(9888): 260-272.
-
López-Cervantes M, Rojas-Russell ME, Tirado-Gómez LL, Arenas DL, Pacheco Dominguez RL, et al. (2009) Enfermedad renal crónica y su atención mediante tratamiento sustitutivo en México. Facultad de Medicina, Universidad Nacional Autónoma de México. México DF.
-
European Commission (2015) The 2015 ageing report. Eur Econ 3: 424.
-
Sociedad Latinoamericana de Nefrología e Hipertensión (2012) Guías Latinoamericanas de Práctica Clínica sobre la Prevención, Diagnóstico y Tratamiento de los Estadios 1-5 de la Enfermedad Renal Crónica.
-
Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, et al. (2005) Acute Renal Faliure in Critically Ill Patients: A Multinational, Multicenter Study. JAMA 294(7): 813-818.
-
Couchoud C, Stengel B, Landais P, Aldigier JC, de Cornelissen F, et al. (2006) The Renal Epidemiology and Information Network (REIN): a new registry for end-stage renal disease in France. Nephrol Dial Transplant 21(2): 411-418.
-
Rosner MH, La Manna G, Ronco C (2018) Acute Kidney Injury in the Geriatric Population. Contrib Nephrol 193: 149-160.
-
Moranne O, Fafin C, Roche S, Francois M, Allot V, et al. (2018) Treatment Plans and Outcomes in Elderly Patients Reaching Advanced Chronic Kidney Disease. Nephrol Dial Transplant 33(12): 2181-2191.
-
Boateng EA, East L (2011) The Impact of Dialysis Modality on Quality of Life: A Systematic Review. J Ren Care 37(4): 190-200.
-
Iyasere O, Brown EA (2015) Mortality in the elderly on dialysis; is this the right debate?. Clin J Am Soc Nephrol 10(6): 920-922.
-
Zuñiga C, Dapueto J, Müller H, Kristen L, Alid R, et al. (2009) Evaluación de la calidad de vida en pacientes en hemodiálisis crónica mediante el cuestionario “Kidney Disease Quality of Life (KDQOL-36)”. Rev Méd Chile 137: 200-207.
-
Dehesa-López E, Correa-Rotter R, Olvera-Castillo D, González-Parra C, Baizabal-Olarte R (2016) Clinical, Dialytic and Laboratory Factors Associated with Poor Health-Related Quality of Life in Mexican Patients on Hemodialysis. Rev Inves Clin 68(4): 192-200.
-
Velarde-Jurado E, Avila-Figueroa C (2002) Assesment of the quality of life. Salud Publica Mex 44: 349-361.
-
Cagney KA, Wu AW, Fink NE, Jenckes MW, Meyer KB, et al. (2000) Formal literature review of quality-of- life instruments used in end-stage renal disease. Am J Kidney Dis 36(2): 327-336.
-
Dehesa-López E, Correa-Rotter R, Olvera-Castillo D, González-Parra C, Baizabal-Olarte R, et al. (2017) Transcultural adpatation and validation of the Mexican versión of the kidney disease questionnaire KDOQOL-SF36 version 1.3. Qual Life Res 26(1): 193- 198.
-
Cleary J, Drennan J (2005) Quality of life of patients on haemodialysis for end-stage renal disease. J Adv Nurs 51(6): 577-586.
-
Durán-Arenas L, Gallegos-Carrillo K, Salinas-Escudero G, Martínez-Salgado H (2004) Hacia una base normativa mexicana en la medición de calidad de vida relacionada con la salud, mediante el Formato Corto 36. Salud Publica Mex 46(4): 306-315.
-
Saad MM, El Douaihy Y, Boumitri C, Rondla C, Moussaly E, et al. (2015) Predictor of quality of life in patients with end-stage renal disease on hemodialysis. Int J Nephrol Renovasc Dis 8: 119-123.
-
Johansen KL (2015) The frail dialysis population: a growing burden for the dialysis community. Blood Purif 40(4): 288-292.
-
Lee SW, Lee A, Yu MY, Kim SW, Kim KI, et al. (2017) Is Frailty a Modifiable Risk Factor of Future Adverse Outcomes in Elderly Patients with Incident End-Stage Renal Disease?. J Korean Med Sci 32(11): 1800-1806.
-
Cervantes L, Lina S, Keniston A, Fischer S (2016) Latinos with chronic kidney failure treated by dialysis: Understanding their palliative care perspectives. Am J Kindey Dis 67(2): 344-347.
-
Rayner HC (2017) How Do We Improve the Quality of Life of Haemodialysis Patients? Now that’s a Good Question. Am J Nephrol 46(1): 1-2.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report