Surgical Aspects and Infection Prevention for Urological Procedures: A Review during 2020 COVID-19 Pandemic
This review has as its goals to highlight the best literature to help urologists to have better clinical decisions as well as means of protection during surgery during the COVID-19 pandemic. It is described which surgeries should be prioritized in the current scenario and the possible risks of COVID-19 contamination in the postoperative period. Furthermore, it is discussed that surgical trauma in asymptomatic patients can compromise the immunity and predispose to Coronavirus infection. The ideal balance between disease severity, comorbidities and risk of COVID-19 development will be important to ideal decision making. Finally we describe important aspects related to PPE and aerosolization protection for minimize infection to surgical team.
Luisa S Machado1 and Marcos Tobias Machado2
Keywords: COVID-19; Pandemic; Surgery; Urology; Laparoscopy; Robotic; Prevention
Introduction
The pandemic Coronavirus diseases (COVID-19) is deeply affecting the healthcare system all over the world. By now, April 5th 2020, it has more than 1 million confirmed cases, and 62.955 total deaths worldwide [1]. The virus, which was named SARS-CoV-2, is known to have a RNA size length of 0.06 to 0.14 microns [2]. The virus was present in the upper and lower respiratory tract, nasopharynx, as well as in the entire gastrointestinal tract. It has been found in nasal and throat swabs, saliva, sputum, blood, bile and feces. Preliminary studies haven’t found the virus in urine or cerebrospinal fluid [3]. Yet, new evidences shows the SARS-coV-2 nucleic acid in urine samples in a percentage of 6.9 [4]. SARS-CoV-2 is known to be transmitted in different ways, as fluids, such as droplets in a cough and direct contact. Aerosolization during endoscopy and surgery could also be a potential mode of COVID-19 transmission.
Urological Concerns during COVID-19 Pandemic
Urology is a vast area which encompasses diseases affecting all ages, with surgical and non-surgical clinical entities. The most prevalent are urinary tract infections (UTIs), kidney stones, urological cancer (prostate cancer and bladder cancer the most prevalent), benign prostatic hyperplasia (BPH), urinary incontinence, erectile dysfunction. All of these conditions are prevalent in patients older than 60 years. In this age group there is more frequency of hypertension, diabetes and pulmonary and cardiovascular diseases; which are the risk factors for Coronavirus infection. In addition, about 50% of Coronavirus transmitters are totally asymptomatic.
Urologists will often face scenarios where they will be in contact with either carriers of the virus or COVID-19 patients. Thus, it is important to educate urologists on this topic.
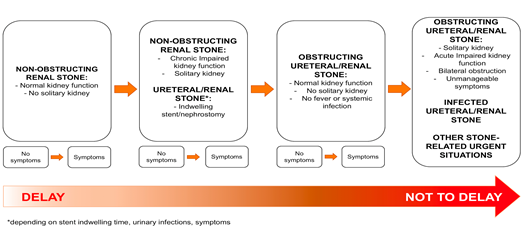
The increasing demand for ventilators-level care in hospitals for COVID-19 cases is causing cancellation of many surgeries [5]. These will be delayed and happen when the healthcare system is normalized and the pandemic is over. Majority of surgeries in the urology field have been postponed due to high risk of COVID-19 contamination/transmission in hospitals. Patients are especially more vulnerable during postoperative period. There are recommendations from different departments from the US and European Urological Association in regards of surgery cases that should be priorities [6]. Is the global pandemic changing the short term progression and/or mortality rates for aggressive cancers?. The balance between disease severity and risk for develop
- coronavirus contamination should be evaluate to better decision making. The boxes below is given as a guide of surgeries that should not be postponed during the COVID-19 pandemic (Tables 1,2 & Figure 1).
- Priorities: Urgencies and Elective Oncological
- Procedures
- Acute obstructive renal insufficiency
- Obstructive pyelonephritis, kidney abscess and pyonephrosis
- Ureteral obstruction (stones and other causes)
- Acute urinary retention (BPH, urethral stenosis, bladder clots, etc)
- Testicular torsion
- Penile fracture
- Priapism refractory to clinical management
- Urogenital trauma with surgical indication
Table 1: Emergencies.
- Transurethral resection for high grade or extensive bladder cancer
- Radical cystectomy
- Radical orchiectomy
- Retroperitoneal lymphadenectomy for residual mass after chemotherapy
- Adrenal mass suspect for malignancy
- Radical nephrectomy for pT3-4 and/or caval thrombus
- Radical nephroureterectomy for high grade TCC
- Radical prostatectomy for high risk prostate cancer
- Penile cancer stage 2 or more (penectomy and inguinal lymphadenectomy)
Table 2: Oncologic Surgeries.
necessary to maintain the surgical field, in order to minimize the side effects to patient and gas leak.
• It’s recommended for the surgeon to use the electric scalpel as low as possible to avoid surgical smoke and aerosol dispersion.
Other recent study described clinical outcomes of 34 patients who underwent surgeries during the COVID-19 period of incubation. Symptoms of viral contamination were suspected only after surgery. It was observed that 44.1% of the patients needed admission to intensive care unit (ICU) and 20.5% died after going to ICU [8]. The researchers claimed that it is essential to carefully select cases that require surgery, in order to reduce risk of COVID-19 infection. The described risk factor for mortality in these series were more complex surgeries with longer operative time, presence of perioperative complications and previous comorbidities.
Risk of Surgical Smoke Contamination by Pathogens
It is acknowledged for a long time that surgical smoke contains chemicals and biological hazards. Among the mutagenic toxins, it is observed large amounts of hydrocarbons, nitriles, fatty acids, and phenols [9]. It is also given that living viruses and bacteria can be transmitted from patient to operator. A recent study published at Cancer Management and Research suggests that human papillomavirus DNA is present in smoke plume generated by LEEP and there is a high risk of the patient to be contaminated [10]. The potential of aerosolization as a mode of transmission during endoscopy or minimally invasive surgery is an actual Society of American Gastrointestinal Endoscopic Surgeons (SAGES) have recently published a guideline for surgeons concerning the use of laparoscopy during the current COVID-19 pandemic that include filtration means and smoke protection - presented on Table 3 [11].
- 1. All pneumoperitoneum should be safely evacuated from the port attached to the filtration device before closure, trocar removal, specimen extraction or conversion to open.
- 2. Once placed, ports should not be vented if possible. If movement of the insufflating port is required, the port should be closed prior to disconnecting the tubing and the new port should be closed until the insufflator tubing is connected. The insufflator should be “on” before the new port valve is opened to prevent gas from back-flowing into the insufflator.
- 3. During desufflation, all escaping CO2 gas and smoke should be captured with an ultra-filtration system and desufflation mode should be used on your insufflator if available.
- 4. If the insufflator being used does not have a desufflation feature, be sure to close the valve on the working port that is being used for insufflation before the flow of CO2 on the insufflator is turned of to prevent reflux of contaminated abdominal CO2 into the insufflator.
- 5. The patient should be flat and the least dependent port should be utilized for desufflation.
- 6. Specimens should be removed once all the CO2 gas and smoke is evacuated.
- 7. Surgical drains should be utilized only if absolutely necessary.
- 8. Suture closure devices that allow for leakage of insufflation should be avoided. The fascia should be closed after desufflation.
- 9. Hand-assisted surgery can lead to significant leakage of insufflated CO2 and smoke from ports and should be avoided. If used to remove larger specimens and protect the wound, it can be placed after desufflation and specimen can then be removed.
Table 3: Recommendations of SAGE concerning laparoscopic procedures.
There are suction devices available to prevent contamination. There is a positive association between the distances of the suction device from the surgical site: The shorter the distance from the suction to the site, less smoke will be produced, thus the lower risk of contamination.
Filtration Means
In order to mitigate infectious transmissions during open laparoscopic and endoscopic procedures it is recommended the use of proper room filtration, ventilation and smoke evacuation device with good suction and filtration apparatus [12]. When operating, surgeons should utilize suitable personal protective equipment (PPE). That includes gloves, medical masks, goggles or face shield, gowns, respirators and aprons [13]. Filtration is an efficient method to prevent the virus from releasing during minimally invasive surgery (MIS) and endoscopy. Masks such as N95 respirators are designed to filter out 95% of particles that are 0.3 microns and larger [14]. Powered Air Purifying Respirators (PAPR) may be positive for intubation, extubation, endoscopy. Intraoperatively, filters are used to eliminate smoke and particulate matter including viruses. Filtration is also essential on a larger level in the positive pressure operative suites [15].
There are two filters that may be efficient. Ultra-Low Particulate Air (ULPA) filters, which remove from a minimum of 99.999% of airborne particles with a minimum particle penetration size of 0.05 microns [15]; and High-Efficiency Particulate Air (HEPA) filters have a minimum 99.97% efficiency rating for removing particles greater than or equal to 0.3 microns in diameter [16] (Table 4).
| Factor | HPV Infection in Surgical Smoke | X2 Value | P-Value | |
|---|---|---|---|---|
| Positive (Positive Rate) | Negative | |||
| Distance of Suction Device from the surgical site (cm) | ||||
| d<3 | 1(9.1%) | 10 | 17.5 | 0.001 |
| 3≤d≤5 | 9 (15.3%) | 50 | ||
| 6≤d≤5 | 23 (45.1%) | 28 | ||
| d>7 | 7 (53.9%) | 6 | ||
| Surgical Time (cm) | ||||
| 1≤t<2.5 | 0 (0) | 4 | 1.4 | 0.833 |
| 2.5≤t<5 | 9 (26.5%) | 25 | ||
| 5≤t<7.5 | 24 (32.9%) | 49 | ||
| 7.5≤t<10 | 3 (30.0%) | 7 | ||
| t≥10 | 4 (30.8%) | 9 | ||
| Cervical patho-logical grade | ||||
| Chronic cervicitis | 0 (0) | 4 | 2.3 | 0.489 |
| CIN І | 14 (37.8%) | 23 | ||
| CIN ІІ | 23 (28.0%) | 59 | ||
| CIN ІІІ | 3 (27.3%0 | 8 |
Table 4: Risk of HPV smoke contamination is directly correlated with distance of suction device and surgical field.
Conclusion
As COVID-19 pandemic is rapidly spreading and affecting the healthcare system all over the world, this paper aims to guide medical societies on two main topics. The schedule of surgeries was changed due to numerous surgeries postponation. Thus, the recommendation for surgery priorities should be only for patients with aggressive tumors or in urgent cases. Second, during urological procedures, it is crucial to make use of proper aspiration devices to prevent surgical smoke contamination. Also, surgeons and all healthcare staff must make rational use of personal protective equipment.
References
-
World Health Organization. Coronavirus disease (COVID-19) Pandemic. April 2020.
-
Zhu N, Zhang D, Wang W, Li X, Yang B, et al. (2020) A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med 382(8): 727-733.
-
Society of American Gastrointestinal and Endoscopic Surgeons. Resources for smoke and gas evaluation during open, laparoscopic and endoscopic procedures.
-
Ling Y, Xu SB, Lin YX, Tian D, Zhu ZQ, et al. (2020) The persistence and clearance of viral RNA in 2019 novel coronavirus disease rehabilitation patients. Chin Med J.
-
American College of Surgeons. COVID-19: Recommendations for Management of Elective Surgical Procedures 2020.
-
Proietti S, Gaboardi F, Giusti G (2020) Endourological stone management in the era of the COVID-19. Eur Urol.
-
Zheng MH, Boni L, Fingerhut A (2020) Minimally invasive surgery and the novel coronavirus outbreak: lessons learned in China and Italy. Ann Surg.
-
Lei S, Jiang F, Su W, Chen C, Chen J, et al. (2020) Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. E Clinical Medicine.
-
Ha HI, Choi MC, Jung SG, Joo WD, Lee C, et al. (2019) Chemicals in surgical smoke and the efficiency of built- in-filter Ports. JSLS.
-
Zhou Q, Hu X, Zhou J, Zhao M, Zhu X, et al. (2019) Human papillomavirus DNA in surgical smoke during cervical loop electrosurgical excision procedures and its impact on the surgeon. Cancer Manag Res.
-
Webmaster S (2020) Resources for Smoke & Gas Evacuation during Open, Laparoscopic, and Endoscopic Procedures. SAGES.
-
Parsa RS, Dirig NF, Eck IN, Payne WK (2015) Surgical Smoke and the Orthopedic Implications. The Internet Journal of Orthopedic Surgery 24(1).
-
World Health Organization. Rational use of personal protective equipment (PPE) for Coronavirus disease (COVID-19).
-
Wiwanitkit V (2006) N-95 face mask for prevention of bird flu virus: an appraisal of nanostructure and implication for infectious control. Lung 184(6): 373-374.
-
High Efficiency Filters and Filter Media for Removing Particles from Air-Part 1: Classification, Performance, Testing, and Marking.
-
Medical Advisory Secretariat (2005) Air cleaning technologies: an evidence-based analysis. Ont Health Technol Assess Ser 5(17): 1-52.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report