Laser Lithotripsy Fundamentals: From the Physics to Optimal Fragmentation
Purpose: Laser Lithotripsy has remained the cornerstone for the management of urolithiasis for more than thirty years. Miniaturization of endoscopic equipment, digital vision, improvement of laser lithotripters, laser fibers has made endourology a field of growing interest, immersed in a technologic revolution. The aim of this article is to do an extense review on laser lithotripsy starting from the physics of the lasers, to translational science apply to lithotripsy fundamentals in order to make lithotripsy safer and more efficient. Methods: We performed a review of the literature in four different databases (PubMed, Embase, Ovid®, and Scopus®,) on any information concerning laser lithotripsy in February 2020 independently by three authors, a total of 186 articles were reviewed and 38 of the most influential articles were selected and a detailed reviewed on this topic is presented. Results: We aim to make a reference paper for all urologists and health personal involved in laser lithotripsy, starting from the physics to answer practical questions as how to set the parameters in my laser system, how to improve lithotripsy efficiency, should we dust or bust? and finally discussing new technologies such as the Holmium: Ytrium-aluminium-garnet (Ho:YAG) Moses technology, the revolutionary thulium laser fiber (TLF) and discussing the future of laser lithotripsy. Conclusions: Laser lithotripsy must offer higher ablative efficiency, wider range of laser parameters and comprehensive combinations, reduce retropulsion and fiber burn-back, scope miniaturization capabilities, smaller fiber sizes, increased safety, lower environmental impact, reduced maintenance costs Ho: YAG has remained the unquestioned gold standard for laser lithotripsy, but the recently launched Thulium fiber laser has all the above mentioned features and outruns without no doubt the current gold standard and is set to gradually replace.
Introduction
Laser Lithotripsy has remained the cornerstone for the management of urolithiasis for more than thirty years. Miniaturization of endoscopic equipment, digital vision, improvement of laser lithotripters, laser fibers has made endourology a field of growing interest, immersed in a technologic revolution that obliged us to know, fundamental basis, basic concepts starting from the physics of laser systems, laser fibers, top-notch instruments, laser parameters, to fragmentation techniques, new technologies in order to correctly apply these fundamentals in our clinical practice and improve lithotripsy efficiency which translates in less operative time, less harm to the patient and the surgeon, improve ergonomics and last but not least stone free rate (SFR).
We aim to make a reference paper for all urologists and health personal involved in laser lithotripsy, starting from the physics of laser lithotripsy to answer practical questions as how to set the parameters in my laser system, how to improve lithotripsy efficiency, dusting or basketing and finally discussing new technologies such as the Ho:YAG Moses technology, the revolutionary thulium laser fiber (TLF) and giving hints to what should we expect from the laser of the future.
Materials and Methods
We performed a review of the literature in four different databases (PubMed, Embase, Ovid®, and Scopus®,) on any information concerning laser lithotripsy in February 2020 independently by three authors. (J.C, H.L, N.F.).
The search criteria were established in the form of free text. We used the free terms “laser”, “lithotripsy”, “holmium laser”, “thulium laser”, “diode laser”, “dusting”, “fragmentation”, “basketing”, “physics” amongst others. The search was limited to publications in the last 50 years.
A grey literature search was also performed on the pages of The National Technical Information Service (NTIS) and the European Association for Grey Literature Exploitation (EAGLE), however, no additional relevant information was found. The articles were all original studies. References were reviewed by title and abstract by three independent reviewers. From the initial selection of articles, references were reviewed full text, ensuring they provided the aforementioned information on all the topics. Duplicate studies were removed, and studies written in any language different from English were discarded.
The authors are performing at least 300-500 laser lithotripsies each year. We aim to report our surgical experience, clinical, and basics knowledge in this topic.
Discussion
History and Laser Physical Principles
Light amplification by the stimulated emission of radiation, used as its acronym (LASER), has been used in medical procedures by many specialties since its discovery in the past century. The fundamentals of its nature were first described by Albert Einstein using Max Planck’s law of radiation, but it was until 1960 that Theodore Maiman developed a rubidium laser being used for the first time in New York’s Presbiterian Hospital in 1961 during an ophthalmologic procedure. Later on, Parsons uses the rubidium laser to experiment in canine bladders, and Mulvany in 1968 tries to fragment bladder stones with it [1].
In the 1980s lasers became of interest of clinicians in urology, and nowadays are an everyday tool in the armamentarium of our specialty, and the gold standard for lithotripsy. Its emission of a beam of energy from an electromagnetic radiation can vary in the electromagnetic spectrum, belonging in either the visible, the infrared or the ultraviolet range [1].
All laser generators must be composed of an energy source, an active medium and a resonant cavity. The latter has a mirror in each opposite end: a completely reflective mirror, and a partially reflective mirror, by which the laser beam will leave the resonant cavity [1].
Within the resonant cavity, an active medium contains the atoms that produce electromagnetic radiation. There are many types of active mediums; the most commonly used being semi conductive, solid, gas or dye. The atoms in this active medium are stimulated by an electric current, in which the electrons surrounding the nucleus increase their movement around the nucleus. Once these electrons return to its elemental state, then the energy is liberated in form of photons [2].
These photons begin to stimulate one another within the resonant cavity, banging again the mirrors containing them until a physic phenomenon called “population inversion” occurs, in which the stimulated photons within the resonant cavity outnumber the non-stimulated ones, thus producing the laser beam [1, 2].
The three classical properties attributed to lasers are as follows: a) Monochromatic: The same wavelength, it allows a high proportion of energy to be delivered in the point of interest. b) Coherence: Its photons travel forward with no dispersion, have minimal divergence, and maintain its brightness over long distances c) Collimation: Photons travel in parallel nature, allowing its use in laser fiber within an endoscope [1].
The effect created on a target depends on several characteristics:
- Power: The rate (frequency, expressed in Hertz - Hz) at which energy (expressed in Joules - K) is delivered, expressed in watts (W).
- Power density: Watts/cm2 (at target surface).
Besides those, how far or close the delivery device is to the target can affect its response [1].
Solid-state lasers are composed of a crystalline host material doped with ions, which are excited after exposure to an electric current. A common crystal is the yttrium aluminum garnet (YAG), usually doped with neodymium, erbium, thulium and holmium, the latter being, with its long- pulse characteristics, the dominant laser currently used for lithotripsy (Ho:YAG) [1].
Lasers can release its energy beam in a pulsed fashion, with pulsed durations varying from femtoseconds (10-15 s) to microseconds (10-6 s). One example is the Q-switched, which uses a “shutter” mechanism to intermittently release light. Another kind is the mode-locked or phase-locked laser; this method takes advantage of wave interference (the phenomenon in which two waves superpose to form a second wave) within the resonant cavity, being able to release short pulses in femtoseconds. Classically, lasers in lithotripsy are generally classified as ultra-short(less than 500 ns), short (1- 10 μs) and long pulse (greater than 250 μs) [2].
Laser Tissue Interactions
How a laser can be used in medicine have its basis in laser tissue interactions. When laser energy strikes tissue, or a kidney stone, three kinds of interactions exist: photochemical, photothermal and photomechanical. Photomechanical is mainly present when using dye lasers, taking advantage of its particular ability to produce singlet oxygen which can react with any nearby molecules. These are not currently used in lithotripsy [1].
Photomechanical, also called photodisruptive interactions are the main mechanisms by which lasers can be used in lithotripsy. They take advantage of the transient stress forces that occur from the deposition of laser energy within and around the stone. It requires shorter pulses with an extremily high spatial density of photons, which have to be coherent in its travel.
Typically less than 10 μs, transient stress waves can be used to produce thermoelastic expansion (the heat inflicted by the laser can cause mechanical disruption, known as spallation), recoil (due to ejection of ablated material) among others, the most important being the production of plasma, often called the “fourth state of matter”, produced by the vaporization of ions existing in a cloud of free electrons. Due to its rapid instability, plasma produces stress fractures with extremely short pulse durations (less than 500 ns), such as in Q-switched lasers. Another example is cavitations bubbles, which occur within 500-1000 ns. The cavitation bubble occurs due to the rapid spherical expansion of water vapor at the laser fiber tip. When this bubble collapses it releases energy, creating very strong pressure waves which shear the stone matrix [3].
Photothermal processes occur due to direct irradiation of energy in the tissue, in this case, a stone. It can be induced through absorption in either endogenous chromophores (aminoacid, NADH, collagens, flavins, porphyrins, hemoglobin, melanin, etc.) or in externally added dyes [4].
Direct irradiation of the laser light produces vaporization, ablation or fragmentation of tissues [5] (Table 1). Lithotripsy can happen either by direct absorption of photons by the stone structure, therefore producing disruption, or by water itself, causing heating and rapidly producing vapor flow, also called explosive vaporization. This is the main mechanism by which the long-pulse laser (2-500 ms) is applied (eg Ho:YAG and erbium:YAG lasers [5, 6, 7].
| Molecular and tissue reactions | |
|---|---|
| 42-45ºC | Hyperthermia leading to protein structural changes, hydrogen bond breaking, retraction |
| 45-50ºC | More drastic conformational changes, enzyme inactivation, changes in membrane permeabilization, edema |
| 50-60ºC | Coagulation, protein denaturation |
| 80ºC | Collagen denaturation |
| 80-100ºC | Dehydration |
| >100ºC | Boling, steaming |
| 100-300ºC | Vaporization, tissue ablation |
| >300ºC | Carbonization |
Table 1: Photothermal effects.
Laser Fibers
Laser fibers are available in many forms, sizes and shapes. Because of the increasing use of laser procedures in endourology, optical fibers form part of the daily armamentarium of the urologist [8, 9, 10, 11]. In order to achieve optimal lithotripsy, the fiber must ensure that the light will travel within the fiber from the proximal to the distal end, smooth insertion and travel in the endoscope, with minimal energy loss within it and low burn-back phenomenon. This “perfect fiber” has been the effort of many manufacturers, but advances are yet being made [12, 15].
The surgical laser device must be lightweight and susceptible of easy transportation, must sustain long operating times with multiple on-off cycles. From its interface, the laser device must ensure correct alignment to the laser fiber. Any interference between them can translate into higher order rays and laser failure. The fiber is usually composed of a low hydroxyl fused-silica core and multiple layers of cladding, since its placing is absolutely necessary to avoid loss of energy during transmission and to ensure delivery at the tip of the fiber [13, 14, 15].
The connector to the laser power source is called “subminiature version A connector” (SMA). Its consists of a central reinforced channel surrounding the optical fiber, the former being covered by a threaded connector shell [12, 15].
Many layers of coating ensure safety against bending, prevents vaporization and heat failure of the fiber. The physics that explains the fact of “sending” a laser beam in one end of the fiber and delivering in the other end have it basis in the physical laws of reflection and refraction. A lens is used to focus the laser beam within the face of the fiber. Some light will be reflected, and some will be refracted. The speed of light traveling within the fiber depends on its index or refraction. The index of refraction of air is 1, and of silica is 1.4572 [12, 13, 15].
Laser Fiber Materials
Cladding in a laser fiber must be as safe and as durable as possible. Many cladding materials have been used in covering these fibers. A fluoroacrylate (TECS, a type of Teflon®) will absorb more of the 2100nm wavelength of a Ho:YAG laser than fluorine-doped silica. This material coats the primary fused-silica glass core of the fiber. That is why it is the primary choice when Ho:YAG laser is used. When using other lasers with shorter wavelengths, TECS could the first choice [8, 9, 13, 16] (Figure 1).
The deleterious effect of fiber bending lies its principle in that if the angle exceeds the maximum propagation angle of the fiber, then power is transmitted into the cladding material, thus damaging it. If sufficient laser leaks into the jacket material, the laser fiber will suffer thermal damage because of the excessive absorption of energy in the cladding layers themselves [8, 9, 13, 16].
Fiber Tips
Historically, laser fibers were manufactured with flat tips. To optimize its use and sterilization, a wide variety of laser tips have been developed. Recently, the round or ball tip was introduced. It allows for smooth insertion through the flexible ureteroscopy, being less likely to perforate its inner lining, even when it is deflected, and also requiring less force of insertion. This protective property is loss once the laser burns back the round tip, making it flat or irregular [17].
Burn-back is a common phenomenon seen in laser lithotripsy and refers to the damage in the tip and cladding of the distal tip of the laser fiber, making it necessary to pause the procedure and prepare the tip to ensure efficient ablation of the stone. Many factors can influence burn-back, including lower fiber diameters, pulse energy, pulse duration and density and composition of the stone [8, 16, 18].
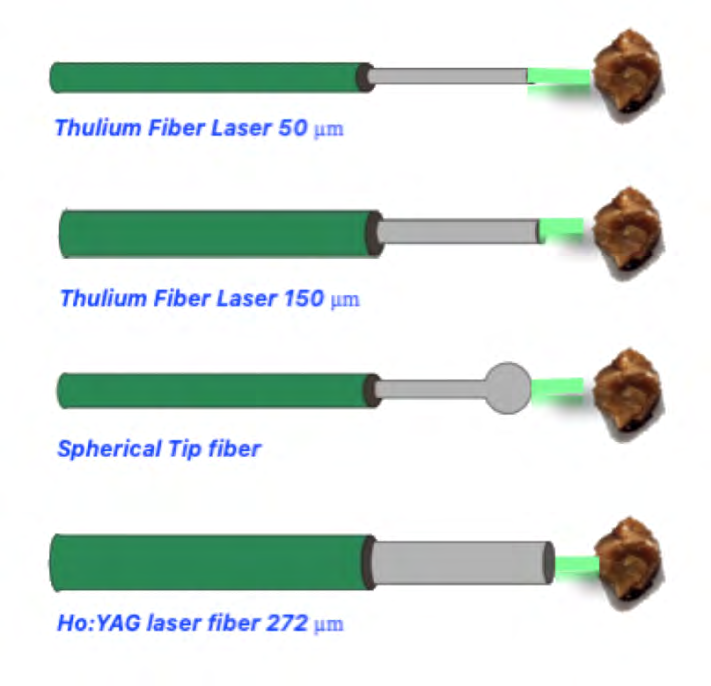
Many fiber tips have been studied in order to minimize burn-back, always having in mind that smaller diameters mean more burn-back. When using TFL one can take advantage of its Gaussian beam profile. This property implies that the majority of the light rays that are transmitted on- axis are low order rays, thus enabling the TFL to use smaller fiber diameters. Hollow-steel tips can experience minimal retropulsion and burn-back while not compromising ablation volumes when using thulium fiber laser lithotripsy [19] (Figure 2).
A tapered fiber consists of a funnel-shaped core, with the longer diameter being proximal and the stepper end lying in the distal end of the fiber. This type of fiber was developed to more easily couple a larger laser beam in the proximal end and reduce the fiber diameter distally to add more flexibility. One study inversed the ends of the fiber, leaving the wider end at the distal tip, showing less damage without compromising fiber bending, stone vaporization or irrigation rates [20].
Laser Parameters Calibration
Laser photo thermal lithotripsy mechanism is effective to treat any stone composition, laser energy is absorbed, and the stone temperature rises until a critical thermal threshold is reached and the result is dehydration, vaporization, carbonization of the stone surface and subsequently crater formation.(3,16,21) Photoacoustic effects from laser have minimal effect on the fragmentation process nonetheless play a role in optical breakdown and plasma initiation which creates shockwaves and cavitational bubbles which finally breaks the stones [21, 22, 23]. Calculus fragmentation depends on two main variants, which are the physical properties of the calculi and laser parameters. Laser parameters pertain to wavelength, pulse energy and pulse duration [3].
Laser parameter calibration varies according to the technique the urologist is planning to perform (dusting or basketing), stone composition and stone size and location.
Laser parameters that could be calibrated are frequency (Hz), optical wavelength (λ), laser pulse duration (Tp), laser pulse energy (Qo), Radiant exposure (Ho) (optical energy per unit area delivered), radiant exposure (Hth) (vaporization, chemical breakdown), fluence (Ψ) (distribution of optical energy per unit area within water or tissue, laser irradiance (Eo) (optical energy per unit area delivered per unit time), threshold irradiance (Eth), laser output power (Po) and laser beam radius (⍵L) [3].
Three main parameters are most used in clinical practice, these are frequency, laser pulse duration (Tp) and laser pulse energy (Qo). Pulse energy is the total optical energy content of a pulse in Joules (J), frequency is defined as the number of pulses emitted per second in Hertz (Hz) and pulse duration is the time during which the laser output pulse power remains continuously above half its maximum value in microseconds (μs). According to the chosen technique laser parameters are usually set up in this fashion: for stone fragmentation and basketing, the frequency is low (5-10 Hz) and laser pulse energy (Qo) its high (0.8-1.5 J), for dusting regimes the frequency is set between 50-80 Hz) and laser pulse energy (0.2-0.6 J) [3, 6, 16, 21, 23, 24, 25]. Laser pulse duration is a mechanical parameter that has gained popularity recently, given that stone retropulsion, fragmentation efficiency and fiber burn back could be related to this parameter [24] (Figure 3).
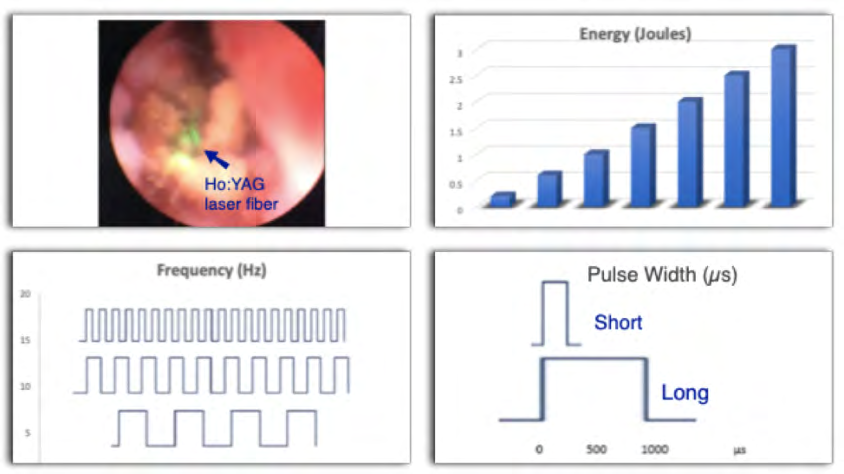
A study by Sroka comparing short laser pulse duration (300-700 μs) and long pulse duration ( 600-1500 μs) found that using the long-pulse mode, the fiber burn-back was negligible, retropulsion measured by the pendulum test was higher in the short-pulse but fragmentation rate did not differ significantly [24]. Another “parameter” that could affect lithotripsy is the Moses effect, this is known as delivering a short, low-energy pulse to create a cavitational bubble before delivery of a longer, high-energy pulse, which has shown to reduce stone retropulsion and increase ablation rates. This technology has been provided as an option on commercial high-power laser systems since 2017 [23].
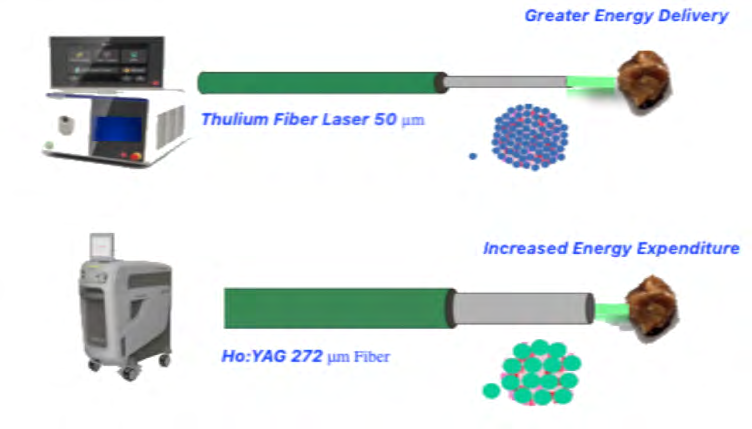
It has been described that crater size during lithotripsy correlates with energy density and multiple pulses, confirming a positive correlation between laser energy and fragmentation rate. Most people could think that the size of the fiber is associated with greater energy delivery to the stone; on the contrary, larger laser fibers are associated with increased energy expenditure to achieve stone fragmentation without improving the fragmentation efficiency [2]. In a study conducted by Marchini, et al. stone size and volume had a significant positive correlation with laser energy expenditure and laser time [22] (Figure4).
Dusting or Busting, the Eternal Dilemma
Laser lithotripsy strategies could be divided in two major categories, the first one is fragmentation with active basket retrieval of the stones and the other one is dusting, which as it sounds aims to make the stone dust (fragments smaller than 2 mm) and left in situ for spontaneous passage [26, 27].
Current Ho:YAG laser systems are able to achieve wavelengths as high as 80 Hz in higher watt systems (60-120 W). In vitro studies have shown that high frequencies lead to more fragmentation at the same pulse energy setting, it could also increase retropulsion but not at the same extent as when increasing the pulse energy [18, 26, 27].
The dusting technique as mentioned before uses low pulse energy and high frequencies, it has two phases. The first stage is the contact laser lithotripsy which aims to break the stones into dust and smaller fragments Second stage is the non-contact laser lithotripsy which is hypothesized to have two action mechanisms, the first one is, after the stone is debulked in numerous fragments, the fiber laser is activated in bursts resulting in a “whirlpool” effect which causes fragments to collide and fragment further; the other mechanism perhaps the most popular was described by Chawla et al, and it is known as the “popcorn” effect which aims to cause laser vaporization of the fragments swirling around. It has been shown that using a long pulse has a protective effect on laser tip degradation, known as burn- back [18, 26, 27].
Aldoukhi, et al. recommend to set the laser system parameter accordingly to the stone density and stone location, in the dusting technique, if the stone is in the ureter and has low density the recommended parameters are 0.2 J x 40 Hz and if the stone has high density the recommended setting are 0.3 J x 40 Hz. If the stone is in the kidney they recommend 0.2 J x 70 Hz if low density and 0.3 J x 70 Hz if high density, if the stone is located in a calyx they preferred to perform a “pop-dusting” technique with a laser configuration with 0.5 J x 80 Hz. All the above with a long pulse duration preferably [26, 27].
The fragmentation and active basket retrieval technique aims to create fragments between 3-4 mm to retrieve them with a stone basket, leaving the patient stone free. If the stone is in the ureter and has low density the recommended parameters are 0.8 J x 6 Hz and if the stone has high density the recommended setting are 1.2 J x 6 Hz. If the stone is in the kidney 1.0 J x 6 Hz if low density and 1.4 J x 6 Hz if high density, all with a long pulse duration [26, 27].
Clinical studies comparing dusting to retrieval techniques are scarce. Chat off et al presented a randomized clinical trial in patients with ureteral stones treated with dusting or active retrieval techniques utilizing an 80-W system [28]. They found the rate for emergency department visits were much higher (30%) in patients treated with dusting technique than when active retrieval was performed (3%), SFR were not statistically significant between both groups [28]. Humphreys and colleagues reported on a prospective multicenter trial comparing dusting vs. basketing, they recruited 84 patients in the basketing group and 75 in the dusting group, they found no difference in complication rates, hospital readmissions, they found a statistically significant difference in basketing operative time, taking 37.7 minutes longer than in the dusting procedure and a lower SFR in the univariate analysis (74.3% vs 58.2%, p=0.04) in the latter group, the SFR was equivalent on multivariate analysis [29].
The question of which surgical technique is optimal remains unanswered and should be determined on a case- by-case basis. Advantages of dusting are that this technique produces smaller fragments, avoids routine use of ureteral access sheath (UAS), and thus reduces the risk of ureteral trauma, has a shorter operation time, could avoid routine postoperative stenting, disadvantages are that it requires next-generation laser systems, SFR may vary according to surgeon skill, there are concerns for fragment drainage in patients with spinal cord injury or clean intermittent catheterization (CIC) and usually results in no fragment for analysis. Fragmentation and active basket retrieval has the advantages that it could be performed with a low power laser system, can extract stone fragments for analysis, the disadvantages are longer operation times, requires a UAS, risk of ureteral injury from UAS and routine stenting is necessary when using UAS [18, 26, 27].
Safety and Complications of Laser Lithotripsy
Regardless of the type of laser or the technique used, there are principles for doing laser lithotripsy safe and avoid harming the patient or damaging the equipment [30, 31, 32]. These principles are: avoid shooting the laser fiber near or inside the tip of the scope, keep in mind the tip of the fiber should always be kept away from the mucosa, be aware of intrarenal temperature (IRT), injury of the human tissues can occur indirectly through elevation of the temperature of the irrigation fluid, absence of high rate irrigation rate (< 30 ml/m) can result in potential harm to the tissue, long laser activation could also raise the IRT above 84.8ªC (without irrigation), 63.9 ªC (medium irrigation) and 43.6 ªC (high irrigation), but IRT cools down rapidly after cessation of laser activation [30, 31].
Harmful corneal effects extending from superficial corneal abrasions to full-thickness corneal loss from exposure to Ho:YAG laser has been reported in an ex-vivo pig model by Villa et al, they found lesions were directly related to pulse energy and time of exposure and inversely related to the distance from the eye. When the laser was placed 5 cm away from the unprotected eye, no corneal damage was observed [33]. The current recommendation is to wear laser protective googles even when wearing eyeglasses. [31, 32, 33].
Complications of laser lithotripsy are rare, but when present they could be catastrophic. Althunayan, et al. reviewed the Manufacturer and User Facility Device Experience (MAUDE) database and the Rockwell Laser Industries (RLI) Laser Accident Database they found a total of 433 adverse events (AEs), 46% resulted from laser generator failure or fiber tip breakage. AEs harming medical operators were 37%, most were eye injuries, none by the Ho:YAG laser. There were 8.3% AEs resulting in patients harm, 1.6% mortality rate, 3 deaths from ureteral perforation with the Ho:YAG and 4 deaths from air emboli Nd: YAG, other complications were bladder perforation, minor skin burns, internal burns, and bleeding [32].
Fundamentals of Holmium Laser
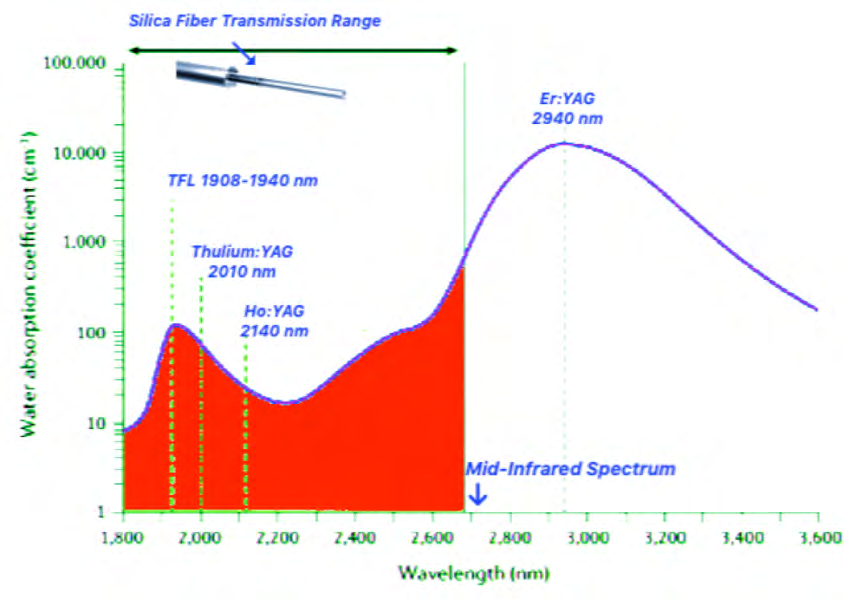
Holmium laser is currently the most popular laser lithotripter, it is a solid-state flashlamp-pumped pulsed laser, it uses a yttrium-aluminum-garnet (YAG) crystal rod to which a flash lamp powered by a high-voltage power supply injects photons and holmium ions within the crystal rod emits new photons at a 2,120 nm wavelength. Water is the dominant absorber of this laser. It has a very low penetration depth (0.4 mm) limiting the amount of energy reaching the mucosa, which gives us a remarkable safety profile and it has been proven to have the ability to fragment stones of any composition [9, 10, 14, 18, 19, 20] (Figure 5).
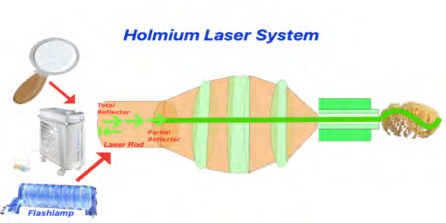
Figure 5: TFL generates the energy through electronically- modulated chemically doped small diode laser. fibers and is then transferred to a 10-20 µm Thulium-doped laser fiber which finally delivers this energy to the small laser fibers of 50-150 µm. TFL offers the most comprehensive range of laser parameters in the market, better absorption coefficient and water optical penetration depth.
Ho:YAG laser activation causes the release of energy from the fiber tip which initially creates a vapor channel, leading to a photothermal reaction causing chemical decomposition of the stones. It also has a photoacoustic effect producing a cavitational bubble that when collapsed generates shockwaves, although this effect does not contribute significantly to calculus fragmentation. It comes in single-use and reusable laser fibers in varying sizes, 200µm, 272µm, 365µm, 550µm and 1000µm, the sizes reflect the true core diameter of each fiber and are mainly made of silica. Ho:YAG system power is available from 20 W to 120 W (High- power novel systems comes with the Moses technology) [9, 26, 27, 30, 33, 34].
A novel feature of the Ho:YAG for further reduction of stone retropulsion and increase in ablation rates was termed as the “Moses effect” which consists in delivering a short, low energy pulse to create a vapor bubble followed by a high energy pulse which acts as the actual ablative energy pulse. This technology has shown to improve significantly ablation rates, improves SFR and reduce retropulsion and fiber burn- back [9, 16, 27].
Fundamentals of Thulium Laser
Opposite to Ho:YAG the thulium fiber laser (TFL) generates the energy through chemically doped small diode laser fibers and is then transferred to another laser fiber which finally delivers this energy to the stone [9, 20, 26, 27, 34, 35, 36]. TFL operates at a wavelength between 1908 and 1940 nm, these wavelengths has the advantage to have a higher absorption peak in water than the Ho:YAG laser, meaning it has a four-time shorter optical penetration. Thulium laser uses small laser fibers of 100 µm. Fibers as small as 50 µm had been tested with comparable stone ablation rates as larger ones, this is possible given that the energy for TFL is generated in a small diode fiber so it can be coupled to laser fibers with small core diameter which allows more space for higher irrigation rates and better ureteroscope maneuverability. TFL has a very different set of parameters than its predecessor, it could be calibrated with pulse energies as low as 33 mJ, and up to 6 J, frequencies as high as 2200 Hz, pulse width could range between 200-1200 µs, maximum system output power at the market is 55 W [9, 20, 26, 27, 34, 36]. TFL could easily be confused with the Thulium: YAG laser which has a wavelength of 2000 nm and it is used exclusively for prostate vaporization and enucleation and is unsuitable for lithotripsy.
Suggested settings for TFL according to several patient cohorts are 0.1–0.2 J/15–30 Hz for dusting of kidney stones, 0.2–0.5 J/10–15 Hz for the dusting and fragmentation of ureteric stones, 2–5 J/30–50 Hz for the fragmentation of large bladder stones and 1–1.5J/15–30Hz for Percutaneous nephrolithotomy PCNL fragmentation and 0.1-0.3 J/50-100 Hz for PCNL dusting [9, 20, 26, 27, 34, 36].
The Laser of the Future
Ho:YAG has been the laser of election for lithotripsy over the last 20 years, but it could be true that time for a change has come [9, 27]. Great interest had come with the development of a new laser technology for laser lithotripsy, this is the TFL which as explains earlier has many advantages over its predecessor, main advantages are the TFL uses electronically-modulated laser diodes which offers the most comprehensive range of laser parameters in the market which translates in a stone ablation efficiency four-times greater than Ho:YAG which has implications in operation time and efficiency for dusting or fragmentation of the stones [9, 27]. TFL is highly absorbed by water and has an absorption coefficient of α=129.2 cm−1 which is four-times greater than Ho:YAG, it has a water optical penetration depth of 0.077 mm which curiously is also 4 times lower than holmium laser (0.314 mm), this means TFL energy pulse will have been reduced only 1.7% of its initial energy after traveling the distance corresponding to its optical penetration depth. (9) Not only the wide range of parameters are the feature of this new laser, also the retropulsion rate is almost negligible with TFL, the laser fibers are as small as 50 µm-core with advantages in irrigation rate, visibility, ability to use other endoscopic instruments simultaneously, maneuverability of the scopes and offering future miniaturization capabilities of the endoscopic instruments [9, 20, 27, 34, 36, 37]. Another advantage of the TFL is that its system generator machine that consumes over nine times less energy and is approximately seven times smaller and eight times lighter than a high- power Ho:YAG system. The TFL produces three to four times more dust, resulting in higher dust particle quantity and smaller particle sizes than with a Ho:YAG laser, which has been recognized as a desirable feature for a lithotripter, this could be explained to a micro-explosive water vapor mechanism which is explained as the water trapped in inter- microcrystal spaces, pores and fissures inside the stone vaporizes suddenly with the TFL and creates very high pressures in the stone surface causing an explosive fashion [9, 20, 27, 34].
In summary, the laser of the future should have the following features: higher ablative efficiency, a wider range of laser parameters and comprehensive combinations, reduce retropulsion and fiber burn-back, scope miniaturization capabilities, smaller fiber sizes which allows simultaneous use of endoscopic instruments, has an increased safety, lower environmental impact, reduced maintenance costs and improve durability and better dusting capabilities than its predecessors. The Thulium fiber laser has all the above mentioned features and outruns without no doubt the current gold standard Ho:YAG [9, 19, 20, 27, 34, 38].
Conclusions
Laser lithotripsy remains the gold standard for the surgical management of urolithiasis. It is imperative to understand the physics of the lasers, interactions with the tissues, their mechanisms of action and mechanical properties of all equipment involved in laser lithotripsy before attempting to improve stone ablation rates. Current clinical gold standard Ho:YAG laser is efficient in treating all stone compositions, the output power has dramatically increased over the past two decades from 20 to 120 W and the parameters including pulse rate, pulse width and energy output has dynamically been increase and allows us to have a broader range of parameter maneuverability enabling increased flexibility, especially for stone dusting approaches which translates in reduced stone retropulsion, and more efficient stone ablation. Despite of this reinvention it has not had a serious competitor since it started its clinical use 30 years ago. Development of a new type of laser technology, has been a field of growing interest in the last decade, at the moment of the experimental laser systems, the TFL is the one who might replace the HoYAG as the gold standard given that it have been demonstrated that the TFL is more efficient for lithotripsy in both dusting and fragmentation modes, providing up to four times faster stone ablation, increasing irrigation rates through the working channel due to smaller fiber size (50–150 μm core), allowing miniaturization of the scopes and finally reduced burnback and stone retropulsion which provides increased stone ablation, and has recently received Conformité Européenne (CE) approval for commercial use. Thus, said at this moment of endourological history we may have the future in our hands but we must rest assure that this is not the only laser lithotripsy technology under development and more is yet to come.
Acknowledgment
Authors have no acknowledgements to make. Author’s disclosure Statement. No competing financial interests exist.
Authors Disclosure Statement
No competing financial interests exist.
Statement of Ethics
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding Sources
Authors have no funding sources to report.
References
-
Gassol JMB (2008) Física Del Láser. Arch Esp Urol 61(9): 961–964.
-
Talati J, Moazzam F, Ahmed M, Sutton RAL (1997) The Management of Lithiasis, Kluwer Academic Publishers.
-
Chan KF, Pfefer TJ, Teichman JMH, Welch AJ (2001) A perspective on laser lithotripsy: The fragmentation processes. J Endourol 15(3): 257-73.
-
G Jori, JD Spikes (1990) Photothermal sensitizers: possible use in tumor therapy J Photochem Photobiol B 6(1-2): 93-101.
-
Peng Q, Juzeniene A, Chen J, Svaasand LO, Warloe T, et al. (2008) Lasers in medicine. Reports on Progress in Physics 71(5).
-
Lee H, Ryan RT, Kim J, Choi B, Arakeri N V, et al. (2004) Dependence of calculus retropulsion dynamics on fiber size and radiant exposure during Ho:YAG lithotripsy. J Biomech Eng 126(4): 506-515.
-
Vassar GJ, Chan KF, Teichman JMH, Glickman RD, Weintraub ST, et al. (1999) Holmium: YAG Lithotripsy: Photothermal Mechanism 13(3): 181-190.
-
Welch AJ (2004) Review of Laser Fibers : A Practical Guide for Urologist. J Endourol 18(9): 818-829
-
Kronenberg P, Traxer O (2019) The laser of the future: Reality and expectations about the new thulium fiber laser-a systematic review. Transl Androl Urol 8(Suppl 4): S398–S417.
-
Wezel F, Michel MS, Bach T, Häcker A, Gross AJ (2010) Effect of Pulse Energy, Frequency and Length on Holmium: Yttrium-aluminum-garnet laser fragmentation Efficiency in non-floating artificial urinary calculi. J Endourol 24(7): 1135-1140.
-
Abhishek P Patel, Bodo E Knudsen (2014) Optimizing Use of the Holmium : YAG Laser for Surgical Management of Urinary Lithiasis. Curr Urol Rep 15(4): 397.
-
Glickman RD. CME Article Efficiency Varies With Stone Composition, 4295(98).
-
Kronenberg P, Traxer O(2015) Update on lasers in urology: current assessment on holmium : yttrium – aluminum – garnet ( Ho : YAG ) laser lithotripter settings and laser fibers.World Urol 33(4): 463–9.
-
Kronenberg P, Traxer O (2014) In vitro fragmentation efficiency of holmium: yttrium-aluminum-garnet (YAG) laser lithotripsy–a comprehensive study encompassing different frequencies , pulse energies , total power levels and laser fibre diameters. Bju Int 114(2): 261–267.
-
Bodo E Knudsen (2019) Laser Fibers for Holimum : YAG Litotripsy : What Is Important and What Is New. Urol Clin North Am 46(2): 185-191.
-
Fried NM, Irby PB (2018) Advances in laser technology and fibre-optic delivery systems in lithotripsy. Nat Rev Urol 15(9): 563-573.
-
Nguyen A, Jain R, Rose E, Monga M, Knudsen B (2018) Pd45-06 Mechanical, Physical And Performance Characteristics Of Holmium:Yag Optical Fibers For Flexible Ureteroscopy. J Urol 199(4s): e888.
-
Matlaga BR, Chew B, Eisner B, Humphreys M, Knudsen B, et al. (2018) Ureteroscopic Laser Lithotripsy: A Review of Dusting vs Fragmentation with Extraction. J Endourol 32(1): 1-6.
-
Hutchens TC, Blackmon RL, Irby PB, Fried NM (2013) Hollow steel tips for reducing distal fiber burn-back during thulium fiber laser lithotripsy. J Biomed Opt 18(7): 078001.
-
Blackmon RL, Irby PB, Fried NM (2010) Thulium fiber laser lithotripsy using tapered fibers. Lasers Surg Med 42(1): 45-50.
-
Li R, Ruckle D, Keheila M, Maldonado J, Lightfoot M, et al. (2017) High-Frequency Dusting Versus Conventional Holmium Laser Lithotripsy for Intrarenal and Ureteral Calculi. J Endourol 31(3): 272-277.
-
Molina WR, Marchini GS, Pompeo A, Sehrt D, Kim FJ, et al. (2014) Determinants of Holmium:Yttrium-aluminum- garnet laser time and energy during ureteroscopic laser lithotripsy. Urology 83(4): 738-744
-
Elhilali MM, Badaan S, Ibrahim A, Andonian S (2017) Use of the Moses Technology to Improve Holmium Laser Lithotripsy Outcomes: A Preclinical Study. J Endourol 31(6): 598-604.
-
Sroka R, Pongratz T, Scheib G, Khoder W, Stief CG, et al. (2015) Impact of pulse duration on Ho:YAG laser lithotripsy: treatment aspects on the single-pulse level. World J Urol 33(4): 479-485.
-
Aldoukhi AH, Ghani KR, Hall TL, Roberts WW Thermal ( 2017) Response to High-Power Holmium Laser Lithotripsy. J Endourol 31(12): 1308-1312.
-
Aldoukhi AH, Roberts WW, Hall TL, Ghani KR (2017) Holmium Laser Lithotripsy in the New Stone Age: Dust or Bust? Front Surg 29(4): 57.
-
Aldoukhi AH, Black KM, Ghani KR (2019) Emerging Laser Techniques for the Management of Stones. Urol Clin North Am 46(2): 193-205.
-
Schatloff O, Lindner U, Ramon J, Winkler HZ (2010) Randomized Trial of Stone Fragment Active Retrieval Versus Spontaneous Passage During Holmium Laser Lithotripsy for Ureteral Stones. J Urol 183(3): 1031- 1035.
-
Humphreys MR, Shah OD, Monga M, Chang YH, Krambeck AE, et al. (2018) Dusting versus Basketing during Ureteroscopy–Which Technique is More Efficacious? A Prospective Multicenter Trial from the EDGE Research Consortium. J Urol 199(5): 1272-1276.
-
Khoder WY, Bader M, Sroka R, Stief C, Waidelich R (2014) Efficacy and safety of Ho:YAG Laser Lithotripsy for ureteroscopic removal of proximal and distal ureteral calculi BMC Urol 14: 62.
-
Noureldin YA, Kallidonis P, Liatsikos EN (2020) Lasers for stone treatment: How safe are they? Curr Opin Urol 30(2): 130-134.
-
Althunayan AM, Elkoushy MA, Elhilali MM, Andonian S (2014) Adverse events resulting from lasers used in urology. J Endourol 28(2): 256-260.
-
Villa L, Cloutier J, Compérat E, Kronemberg P, Charlotte F, et al. (2016) Do We Really Need to Wear Proper Eye Protection When Using Holmium:YAG Laser during Endourologic Procedures? Results from an Ex Vivo Animal Model on Pig Eyes. J Endourol 30(3): 332-337.
-
Blackmon RL, Irby PB, Fried NM (2011) Comparison of holmium:YAG and thulium fiber laser lithotripsy: ablation thresholds, ablation rates, and retropulsion effects. J Biomed Opt 16(7): 071403.
-
Blackmon RL, Irby PB, Fried NM (2010) Holmium:YAG (lambda=2,120 nm) versus thulium fiber (lambda = 1,908 nm) laser lithotripsy. Lasers Surg Med 42(3): 232- 236.
-
Wilson CR, Hardy LA, Kennedy JD, Irby PB, Fried NM (2016) Thulium fiber laser lithotripsy using small spherical distal fiber tips. Photonic Ther Diagnostics XII: 96891G.
-
Hardy LA, Kennedy JD, Wilson CR, Irby PB, Fried NM (2016) Cavitation bubble dynamics during thulium fiber laser lithotripsy. Photonic Ther Diagnostics XII: 96891B.
-
Blackmon RL, Hutchens TC, Hardy LA, Wilson CR, Irby PB, Fried NM (2014) Thulium fiber laser ablation of kidney stones using a 50-μm-core silica optical fiber. Opt Eng 54(1): 011004.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report