Penile Self-Mutilation: Cause and Management
Self-mutilation of the penis is an unusual situation, which occurs in the majority of cases in a psychotic illness. The diagnosis is clinical and the management is multidisciplinary. We present a case of penile self-mutilation in a 36-year-old patient who was being treated for schizophrenia and had poor adherence to medication. The family went to the emergency room after seeing blood on his clothes by mistake. A severed penis with à 3 cm stump, a massive blood clot, and an amputation of part of the right hemi scrotum were discovered during the urogenital examination. A urethrostomy was performed, followed by suturing of the various plants of the residual stump and the scrotum. The postoperative follow-up was simple. The patient is followed up with his psychiatrist at the same time. The management of genital self-mutilation requires coordination between urologists and psychiatrists.
Introduction
The penis is a male organ that serves two purposes (urinary and copulation). Self-injurious behaviour, self- mutilative behaviour or self-harming behaviour are defined as deliberate destruction of body tissue without conscious suicidal inten [1]. It is a rare occurrence [2]. Emasculation is a more unusual and complicated kind of self-injury, both in terms of psychopathology and symbolism.
It can be a recurring behaviour aiming at alleviating pain, as well as a solitary, impulsive act in a delirious environment. Penis self-mutilation causes three issues: urinary, sexual, and cosmetic. The re-implantation of the penis is possible, but it necessitates a set of circumstances that might be difficult to come across [3].
We describe a case of entire penis self-mutilation. The seriousness of the self-mutilating act, its clinical and psychopathological context, and its frequently permanent repercussions are the focus of this study.
Mr. A.M., 36, followed for schizophrenia for two years on neuroleptics treatments but had poor compliance. The patient was admitted to our department three days prior to his arrival after having his penis amputated. The family went to the emergency room after seeing blood on his clothes by mistake. The patient said that his penis was a devil’s source, prompting him to amputate it. A severed penis, replaced by a blood clot, with amputation of part of the right hemi scrotum, is discovered during a urogenital examination (Figure 1).

The patient was transferred to the operating room, where a surgical exploration revealed a 3cm penis stump with necrotic tissues (Figure 2).
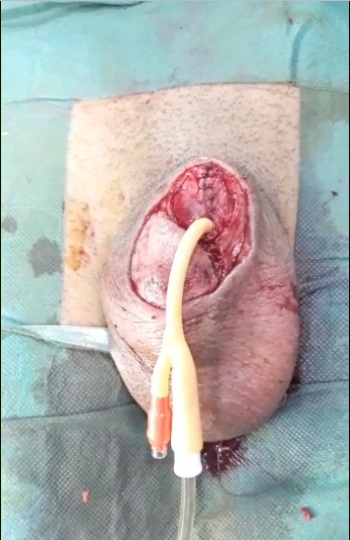
We performed a necrosectomy of these tissues, followed by cleaning and remodelling of the remaining penis. A foley catheter was used to catheterize the bladder, and the gesture was finished by a urethrostomy at the same surgical period, followed by suturing of the various plants (Figure 3).

The postoperative follow-up was simple. At the same time, the patient is followed up with by his psychiatrist.
Discussion
Self-injury is extremely uncommon, with an incidence of 1-4 percent in the general population of the United States and 4.6-6.6 percent in the United Kingdom [2]. The procedure of sectioning the penis is uncommon in the literature, and it is exceedingly rarer when combined with the excision of the testicles. The patient merely submitted a whole portion of the penis in our situation, and the testicles were intact.
Self-injury is not a pathognomonic symptom of any disease. Self-mutilation explanations rely on neurohormonal processes of self-preservation [4].
Self-injurious behaviour is most common in psychotic individuals, with schizophrenics accounting for the bulk of cases. Depressive illnesses, mental retardation, and personality disorders are all capable of these behaviour [5].
Apart from psychotic substance abuse, individuals may be at risk of self-harm due to extreme sexual uncertainty, remorse, loss of bodily integrity, penis rejection, or the sensation of being a woman [6].
The diagnosis of self-mutilation is clinical and patients often consult the same day, in contrast to our case, when the consultation duration surpassed 48 hours.
The patient is usually notified by the bleeding, and his entourage goes to the hospital with him. In other cases, the patient only seeks medical advice after experiencing symptoms such as penile edoema, dysuria, or acute urinary retention [7].
When feasible, re-implantation of the penis should be done after ensuring that the patient is not insane, because it will surely return [8]. This recurrence of penile self- amputation in schizophrenic individuals has also been brought to attention [9].
To ensure a good result, the reimplantation technique must follow certain strict rules: disinfection and preservation of the distal amputated stump in cold sterile physiological serum, disinfection and encirclement of the proximal end with a compression dressing, and the technique of choice is microsurgical reimplantation with vascular and nerve anastomosis.
Conclusion
Total section self-mutilation of the penis is a rare case in urology, occurring frequently in the context of psychiatric illness. It puts at risk the vital prognosis, as well as the urological and sexual functioning prognosis, in the event of significant bleeding.
The management must be multidisciplinary, involving a variety of specialists: Urologist, psychiatrist, plastic surgeon.
References
-
Favazza A (1998) The coming of age of self-mutilation. J Nerv Mental Dis 186(5): 259-268
-
Gicquel L, Corcos M, Richar DB, Guelfi JD (2007) Automutilations à l’adolescence EMC Traité de Psychiatrie Paris. Elsevier Masson SAS 37: 216.
-
Odzébé AWS, Bouya PA, Otiobanda GF, Banga Mouss R, Nzaka Moukala C, et al. (2015) Auto-amputation de verge traitée par réparation d’emblée: à propos d’un cas et revue de la littérature. Prog Urol 25(16): 1173-1177.
-
Khan MK, Usmani MA, Hanif SA (2012) A case of self amputation of penis by cannabis induced psychosis. Journal of Forensic and Legal Medicine 19(6): 355-357.
-
Hendershot E, Stutson AC, Adair TW (2010) A case of extreme sexual self-mutilation. Journal of forensic sciences 55(1): 245-247.
-
Hicks KM, Hinck SM (2008) Concept analysis of self- mutilation. Journal of advanced nursing 64(4): 408-413.
-
Sarr A, Sow Y, Ndiaye B, Koldimadji M, Ouedraogo B, et al. (2015) Male genital self-mutilation: about two cases. Sexologies 24(2):65-68.
-
Prunet D, Bouchot O (1996) Traumatisme du pénis. Progrès en Urologie 6 : 987-993.
-
Kabore FA, Fall PA, Diao B, Fall B, Odzebe A, et al. (2008) Autoamputation récidivante du pénis sur un terrain schizophrène: à propos d’un cas. Andrologie 18(3): 224- 226.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report