Hyponatremia in Chronic Kidney Disease
Introduction: There is adequate literature written on hyponatremia, but not much seen in context of Chronic Kidney Disease (CKD). Patients become prone for this electrolyte derangement when they are afflicted with organ failure especially CKD. This vulnerability becomes even worse in ageing due to impaired sensitivity to fluid intake and often burdened with multiple comorbid. For the adequate management of hyponatremia, knowledge of volume status, age of patients and associated comorbid, and duration of hyponatremia are very important. Patients and Methods: This observational study was conducted in adult CKD admitted patients. Demographic information, history, and examination finding were noted. Then each patient underwent investigation i.e., serum sodium, urea, creatinine, spot urine sodium, chloride, potassium, urine and serum osmolality, random blood sugar and echocardiography and noted in questionnaire. CKD staging was done with the help of Modified of diet and Renal disease (MDRD) equation. Diagnosis/ Impression of patient and need of hypertonic saline (3%saline) were all noted along with final outcome whether sodium improved/unimproved, discharge/expired were noted in pre-formed questionnaire. Results: Analysis was done on 171 CKD patients with female to male ratio: 1.19/1 and mean age 55.8 ± 15.16. Hypertension was most prevalent comorbid. Hypovolemia was the most common volume status seen along with moderate hyponatremia and hypertonicity were frequently observed features. 23 out of 171 patients were symptomatic, 44(25.7%) had low Left Ventricular function. Mortality was noted at 9.4%. Conclusion: Overall outcome of patient remained satisfactory despite of presence of CKD and significant number of patients were severe hyponatremic. Predominant management for hyponatremia remained conservative along with treatment for primary disease. Symptomatic hyponatremia and low LV function were found to be contributing to bad outcomes while severity of hyponatremia did not influence badly
Introduction
Prevalence of Hyponatremia has been documented from 6% to 44% in general population but not seen specifically in chronic kidney disease (CKD) [1, 2]. Although if we see specifically in dialysis population then hyponatremia is not uncommon [3, 4]. Lot of literature has been written on subject of Hyponatremia still it seems lot more is needed because of its clinical importance. The wide variety of its presentation, association, and outcome keep pressing clinician to write more on this subject. The most vulnerable population identified to develop hyponatremia so far is elderly population because of increased comorbidity burden in this age group and impaired excretion of salt [5]. After this, the second vulnerable population group is CKD and Congestive heart failure (CCF) patients, as there is tendency of retaining excessive water and there is also frequent use of diuretics in these patients [6, 7]. The osmotic balance maintained mainly by sodium concentration with the help of aquaporin channels, comes under risk when glomerular filtration rate (GFR) declines with progression of CKD [8, 9].
In order to manage hyponatremia patients properly, knowledge of patient’s age, comorbidity, volume status at that time, duration of hyponatremia whether acute or chronic, and drugs which patient has been taking, are required. Based on this, Clinician decides aggressiveness of management plane. Aggressive plane includes use of hypertonic saline (3%saline), opted for acute hyponatremia (<48 hour of duration), or symptoms suggestive of central nervous system (CNS) i.e. confusion, fits, coma etc. Conservative approach mainly includes plain water restriction, salt addition in water and diet, and use of isotonic saline. This is in addition of the treatment of primary disease which is usually associated in clinical setting.
Here caution must be exercised before deciding 3% saline to correct sodium rapidly as this may be proved as counterproductive if sodium corrected rapidly more than what was desired. This rapid overcorrection is manifested clinically as locked-in due to sudden change in serum osmolality in brain [10]. Danger of sodium overcorrection would also be there where patients have volume overload in background of CCF and CKD with hyponatremia and dialysis comes as a rescuer. In this circumstance, dialysis duration with low sodium conductivity is employed [11]. In both of these aggressiveness (using 3% saline and dialysis), risk of overcorrection and thus central pontine myelinosis would always be there if not handled judiciously [12]. Therefor the risk carrying therapy should only be restricted to a very selected group of patients whose neurological symptoms are not otherwise explained.
Methodology
This observational study was conducted at the Indus Hospital and Health Network, Karachi campus from July 2017 to April 2020 after the approval of ethical committee (IRB). All those (age >16 years) of either gender who were admitted under care of various specialties with Hyponatremia (serum sodium<135 meq/L) and renal impairment were enrolled in this study after getting consent. These patients were subjected to detailed history and general physical examination; their demographic were noted and relevant investigations were done. Serum sodium on day of admission, enrollment and on discharged were noted and its severity was categorized as mild (From 130 to 134), moderate (From 125 to 129) and severe (<125 meq/L). Volume status of patient was decided on basis of presence or absence of edema, jugular venous pressure, bibasilar inspiratory crepitation and gallop sound on auscultation at the time of enrollment. Based on these finding, these patients were categorized as hypovolemic, normovolemic, and hypervolemic. Laboratory parameters i.e. serum sodium, urea, creatinine, spot urine sodium, chloride, potassium, urine and serum osmolalities, random blood sugar and echocardiography finding (left ventricular function) were noted in questionnaire. Chronic kidney diseases (CKD) patients were further categorized into five CKD stages with the help of Modified of diet and Renal disease (MDRD) equation. Any surgical procedure/Operation if done was also noted. Diagnosis/Impression of patient and use of hypertonic saline (3%saline) were also noted. Final outcome of patients i.e. those who improved sodium and symptoms, discharge/expired along with total hospital stay was noted in pre-formed questionnaire.
Statistical Analysis
The data was entered and analyzed on SPSS IBM version 21. Cleaning and coding of data was done prior to analysis. Mean ± STD and Median with Interquartile range were computed for continuous variables, while frequency with percentage was calculated for categorical variables. Association between categorical variables was established by Chi square test. On the other hand, one way Anova was applied for normally distributed continuous data, while Kruskall Wallis test was executed for skewed variables. Normality of data was checked by Shapiro Wilk”s test. P value of ≤ 0.05 was set as significant level.
Results
There were a total of 262 patients enrolled in our study; out of which analysis was performed on 171 patients who are established cases of CKD. The female to male ratio was 93/78 (1.19/1). The mean age was 55.8 ± 15.16 years, with a minimum of 16 and a maximum of 86 years. The mean serum sodium and osmolality were as 125.19 ± 5.82 and 298.62 ± 38.13. The most prevalent comorbid was HTN 128 (74.9%), followed by DM 108(63.1%) and IHD 53 (31%). Mild hypernatremia was noted in 56 (32.7%), Moderate 71 (41.5), and Severe 44 (25.7%) patients. From tonicity point, Hypertonic were 81 (47.4%), Hypotonic 51 (29.8%), Normotonic 39 (22.9%). Normovolemic were 44 (25.7%), hypovolemic 80 (46.8%) and hypervolemic 47 (27.5). Total symptomatic hypernatremia out of 171 patients were 23 (13.5%). Left Ventricular dysfunction (LV dysfunction) was seen in 44 (25.7%). Spot urine sodium >20 meq/L was seen in the majority of patients 150 (87.7%).While Urine to serum electrolyte ratio <50% was in 101 (59.1%) patients.
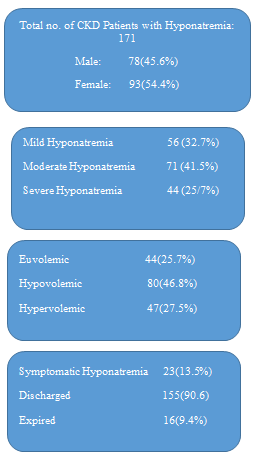
- The overall outcome of hyponatremia was good as the majority of the patients155 (90.6%) were recovered and discharged Figure 1 and Table 1.
- CKD Stages
- Hyponatremia
- Total (100%) p-Value
- Mild
- Moderate
- Severe
- Stage 1
- 3(30%)
- 5(50%)
- 2(20%)
- 10
- Stage 2
- 7(43.8%)
- 3(18.8%)
- 6(37.5%)
- 16
- Stage 3
- 12(29.3%)
- 21(51.2%)
- 8(19.5%)
- 41
- Stage 4
- 15(30.6%)
- 19(38.8%)
- 15(30.6%)
- 49
- Stage 5
- 19(34.5%)
- 23(41.8%)
- 13(23.6%)
- 55
- Total
- 56(32.7%)
- 71(41.5%)
- 44(25.7%)
- 171
Table 1: Comparison of CKD stages with Severity of Hyponatremia (n= 171).
- 0.621
Table 2: Volume status was analyzed with CKD stages which
| Laboratory Parameters | Mean ± STD | Median , IQR | Minimum | Maximum |
|---|---|---|---|---|
| Age in Years | 56.05± 15.25 | 56 , 19 | 16 | 86 |
| S. Na at enrollment | 125.19 ± 5.82 | 126 , 8 | 106 | 135 |
| Urinary Na at enrollment | 47.15 ± 26.89 | 42 ,37 | 2 | 176 |
| S.Osmolality at enrollment | 298.62 ± 38.13 | 293 ,54 | 220 | 412 |
| U.Osmolality at enrollment | 264.67 ± 87.41 | 260.50 , 103 | 21 | 612 |
| Urinary Cl at enrollment | 45.57 ± 24.06 | 39 , 34 | 10 | 135 |
| Urinary K at enrollment | 17.30 ± 11.22 | 15 , 14 | 2 | 75 |
| S. Urea at enrollment | 134.74 ± 64.80 | 125.5 , 74 | 13 | 504 |
| RBS at enrollment | 163.66 ± 84.77 | 140, 78 | 50 | 497 |
Table 3: Comparison of CKD stages with Severity of Hyponatremia (n= 171).
Analysis was done with a chi-square test to see the relation of CKD stages with the severity of hyponatremia, which was not statistically significant (p-value 0.621),
- 0.621
Table 2: Volume status was analyzed with CKD stages which
- <0.001), Table 4 Analysis was done to see severity effect of hyponatremia causing symptoms; it revealed non-significant
- (p-value 0.074), (Table.4). When we analyzed the mortality
- (outcome) in relation to neurological symptoms, the severity
- CKD Stages
- Volume Status
- Total (100%) p-Value
- Hypovolemia
- Normovolemic
- Hypervolemic
- Stage 1
- 4(50%)
- 4(9.1%)
- 2 (4.3%)
- 10
- Stage 2
- 8(18.8%)
- 2(4.5%)
- 6 (12.8%)
- 16
- Stage 3
- 21(51.2%)
- 11(25%)
- 9 (19.1%)
- 41
- Stage 4
- 21(38.8%)
- 13(29.5%)
- 15(31.9%)
- 49
- Stage 5
- 26(41.8%)
- 14(31.8%)
- 15(31.9%)
- 55
- Total
- 80(100%)
- 44(100%)
- 47(100%)
- 171
- LV Function
- Normal
- 37 (29.1%)
- 67 (52.8%)
- 23 (18.1%)
- 127
- <0.001
- Low
- 7 (15.9%)
- 13 (29.5%)
- 24 (54.5%)
- 44
- Total
- 44 (25.7%)
- 80 (46.8%)
- 47 (25.5%)
- 171
Table 4: Comparison of Volume Status with CKD stages and LV function.
| Severity of Hyponatremia | Symptomatic Hyponatremia | Total (100%) | p value | |
|---|---|---|---|---|
| Yes | NO | |||
| Mild | 4(7.1%) | 52(92.9%) | 56 | 0.074 |
| Moderate | 9(12.7%) | 62 (87.3%) | 71 | |
| Severe | 10 (22.7%) | 34(77.3%) | 44 | |
| Total | 23(13.5%) | 148 (86.5%) | 171 |
Table 5: Relation of Symptoms with Severity of Hyponatremia.
| Symptomatic Hyponatremia | Outcome | Total (100%) | p value | |
|---|---|---|---|---|
| Discharged | Expired | |||
| Yes | 16 (69.6%) | 7(30.4%) | 23 | 0.001 |
| No | 139 (93.9%) | 9 (6.1%) | 148 | |
| Total | 155 (90.6%) | 16 (9.4%) | 171 | |
| Severity of Hyponatremia | ||||
| Mild | 53 (94.6%) | 3(5.4%) | 56 | 0.363 |
| Moderate | 64(90.1%) | 7(9.9%) | 71 | |
| Severe | 38 (86.4%) | 6 (13.4%) | 44 | |
| Total | 155 (90.6%) | 16 (9.4%) | 171 | |
| LV Function | ||||
| Normal | 119(93.7%) | 8(6.3%) | 127 | 0.032 |
| Low | 36(81.8%) | 8(18.2%) | 44 | |
| Total | 155(90.6%) | 16(9.4%) | 171 |
Table 6: Outcome in Relation with Severity and Symptoms of Hyponatremia, and LV function.
Discussion
This study was conducted over 171 CKD patients with variable degree of hyponatremia admitted under medical and surgical specialties. The most prevalent comorbid was HTN, followed by DM and IHD. The most common volume status of the patients was hypovolemia. The majority of patients were having moderate degree of hyponatremia. Symptomatic hyponatremia was seen in 23 (13.5%) patients. The overall mortality remained at 9.4%. From a tonicity point in our studied patients, we observed hypertonic hyponatremia was the most often seen phenomenon. This hypertonicity must be contributed by blood sugar and urea as our studied population is CKD and diabetes is significantly present in them. In absence of these osmoles (urea, glucose), another possibility remains the presence of excessive lipids, proteins, methanol, or ethanol in blood. The possibility of the presence of these osmoles becomes more when measured osmolality comes more than calculated osmolality (osmolar gap>10) [13].
The kidney is the major organ in regulating electrolytes and volume in the body which come under stress when its function lowers due to any reason. This results in the accumulation of excessive water in the body and often gives rise to hypervolemia which is sometimes present as hyponatremia [14, 15, 16] but this is not always the case as on several occasions, the volume of the body remains either unchanged or even reduced sometimes along with hypernatremia. In such cases, salt is excreted more through the kidneys and this can be measured objectively with the laboratory test of a spot urine sample. Spot urine value >20 meq/L is suggestive of the salt-losing behavior of kidneys in presence of hyponatremia and patient is not on diuretics [17]. The salt-losing behavior of kidney is not only found in presence of renal failure or patient is on diuretics but also syndrome of inappropriate ADH secretion may cause it. We found in our population the mean value of spot urine sodium >20 meq/L, which is suggestive of significant number of patients lose sodium from kidney. It is also important to mention the predominant volume status of our patients is hypovolemia. (See Table.2) Under normal circumstance (without renal failure), kidney behavior is assumed to conserve sodium and this can be manifestoed as spot urine sodium <20 meq/L. Although this finding cannot be said impossible or false when we deal with CKD patients, but predominant hypovolemic status does not favor it. This query was helped when we studied simultaneously the ratio of sum of the urinary sodium plus potassium divided by serum sodium. The majority of the patients were having ratio less than 50%, which suggest salt conservation behavior of kidneys [18]. The conclusion can be drawn with these findings that although sodium is being lost in majority of patients but aggregated salt (sodium + potassium) is not being lost in majority of the patients.
Hypertension has long been discussed as a cause and consequence of CKD [19]. Therefore its presence significantly in our studied population is not surprising altogether. Other than this, significant presence of diabetes mellitus and Ischemic heart disease (IHD) as comorbidities in our studied population, also contribute for developing hypertension. Several factors related with CKD play their role in the pathogenesis of hypertension i.e overactive sympathetic nervous system, sodium retention, and activated RAAS etc [20]. This increases the risk of cardiovascular mortality. Hypertension has also been established an independent risk factor for CV mortality [21].
The association of congestive heart failure (CHF) with hypernatremia is well established in the literature [22, 23]. Over the years, this has been realized that the mortality in CKD patients increases many fold once ischemic heart disease is present which results in CCF [24]. This occurs primarily secondary to an increased level of vasopressin (AVP) and increased sympathetic activity. This leads to accumulation of water, making it a dilutional form of hyponatremia. This marks the severity of heart failure and plays role in morbidity and mortality [25, 26]. In our studied population, Low LV function has been observed in one-fourth of all populations where hypervolemia was the predominant volume status. This comorbid contributed statistically significant in mortality while studying our studied population.
There is different mortality rate has been seen in hypernatremia but this question remained debatable that this mortality is secondary to hypernatremia or its associated primary disease [27, 28, 29]. Whatever the reason for death among these patients but once CKD is associated, mortality increases. In our studied population, mortality remained around (9%) which is not bad enough especially if we count CKD with comorbidities. Factors found contributing to mortality were symptomatic hypernatremia and low LV function. Further studies need to be done to find actual mortality in context of CKD and factors leading to it.
Conclusion
Hyponatremia is an undoubtedly most frequently observed medical condition in hospitalized patients and often multifactorial in origin. Presence of CKD makes patients even prone for this derangement. Outcome is not often bad when management is preferably done more conservatively on part of hyponatremia and aggressiveness can be reserved for the treatment of primary disease. Severity of hyponatremia do not make prognosis worse while Symptomatic hypernatremia and low LV function do.
Acknowledgement
We gratefully acknowledge Nida Ghori for preliminary analysis of data in this manuscript and Dr. Jhanzeb Khan for incorporation of data in SPSS.
Conflict of Interest
There is no conflict of interest in this study.
References
-
Frontera JA, Valdes E, Huang J, Lewis A, Lord AS, et al. (2020) Prevalence and impact of hyponatremia in patients with coronavirus disease 2019 in New York City. Critical care medicine 48(12): e1211-e1217.
-
Asadollahi K, Beeching N, Gill G (2006) Hyponatraemia as a risk factor for hospital mortality. Journal of the Association of Physicians 99(12): 877-880.
-
Ravel VA, Streja E, Mehrotra R, Sim JJ, Harley K, et al. (2017) Serum sodium and mortality in a national peritoneal dialysis cohort. Nephrology Dialysis Transplantation 32(7): 1224-1233.
-
Rhee CM, Ravel VA, Ayus JC, Sim JJ, Streja E, et al. (2016) Pre-dialysis serum sodium and mortality in a national incident hemodialysis cohort. Nephrology Dialysis Transplantation 31(6): 992-1001.
-
Ganguli A, Mascarenhas RC, Jamshed N, Tefera E, Veis JH (2015) Hyponatremia: incidence, risk factors, and consequences in the elderly in a home-based primary care program. Clinical nephrology 84(2): 75-85.
-
Zhang R, Wang S, Zhang M, Cui L (2017) Hyponatremia in patients with chronic kidney disease. Hemodialysis International 21(1): 3-10.
-
Farmakis D, Filippatos G, Parissis J, Kremastinos DT, Gheorghiade M (2009) Hyponatremia in heart failure. Heart failure reviews 14(2): 59-63.
-
Rasouli M (2016) Basic concepts and practical equations on osmolality: Biochemical approach. Clinical biochemistry 49(12): 936-941.
-
Lim LM, Tsai NC, Lin MY, Hwang DY, Lin HY, et al. (2016) Hyponatremia is associated with fluid imbalance and adverse renal outcome in chronic kidney disease patients treated with diuretics. Scientific reports 6(1): 1-0.
-
Kobashi H, Fujii T, Kusuhara S, Shirai T, Mima K, et al. (1988) Central pontine myelinolysis following rapid correction of hyponatremia: Diagnosis by CT scan. Nihon Naika Gakkai zasshi. The Journal of the Japanese Society of Internal Medicine 77(1): 69-73.
-
Rhee CM, Ayus JC, Kalantar-Zadeh K (2019) Hyponatremia in the dialysis population. Kidney international reports 4(6): 769-780.
-
Diringer M (2017) Neurologic manifestations of major electrolyte abnormalities. Handbook of clinical neurology 141: 705-713.
-
Silver SM, Sterns RH, Halperin ML (1996) Brain swelling after dialysis: old urea or new osmoles? American Journal of Kidney Diseases 28(1): 1-13.
-
Kooman JP, van der Sande FM, Leunissen KM (2004) Role of sodium and volume in the pathogenesis of hypertension in dialysis patients. Blood purification 22(1): 55-59.
-
Chen TK, Knicely DH, Grams ME (2019) Chronic kidney disease diagnosis and management: a review. Jama 322(13): 1294-1304.
-
Hung SC, Kuo KL, Peng CH, Wu CH, Lien YC, et al. (2014) Volume overload correlates with cardiovascular risk factors in patients with chronic kidney disease. Kidney international 85(3): 703-709.
-
He J, Mills KT, Appel LJ, Yang W, Chen J, et al. (2016) Urinary sodium and potassium excretion and CKD progression. Journal of the American Society of Nephrology 27(4): 1202-1212.
-
Sahay M, Sahay R (2014) Hyponatremia: A practical approach. Indian journal of endocrinology and metabolism 18(6): 760.761.
-
Tedla FM, Brar A, Browne R, Brown C (2011) Hypertension in chronic kidney disease: navigating the evidence. International journal of hypertension 2011: 132405.
-
Arima H, Barzi F, Chalmers J (2011) Mortality patterns in hypertension. Journal of hypertension 29(1): S3-S7.
-
Farmakis D, Filippatos G, Parissis J, Kremastinos DT, Gheorghiade M (2009) Hyponatremia in heart failure. Heart failure reviews 14(2): 59-63.
-
Oren RM (2005) Hyponatremia in congestive heart failure. The American journal of cardiology 95(9A): 2B- 7B.
-
Tonelli M, Wiebe N, Culleton B, House A, Rabbat C, et al. (2006) Chronic kidney disease and mortality risk: a systematic review. J Am Soc Nephrol 17(7): 2034-2047.
-
Ahmad F, Hadi A, Iqbal MA, ullah Khan I, Adnan Y, et al. (2014) Frequency of hyponatremia and in-hospital clinical outcomes in these patients hospitalized for heart failure. Journal of Postgraduate Medical Institute (Peshawar-Pakistan) 28(4): 362-366.
-
Kumar S, Rubin S, Mather PJ, Whellan DJ (2007) Hyponatremia and vasopressin antagonism in congestive heart failure. Clinical Cardiology: An International Indexed and Peer‐Reviewed Journal for Advances in the Treatment of Cardiovascular Disease 30(11): 546-551.
-
Hao J, Li Y, Zhang X, Pang C, Wang Y, et al. (2017) The prevalence and mortality of hyponatremia is seriously underestimated in Chinese general medical patients: an observational retrospective study. BMC nephrology 18(1): 328.
-
Winzeler B, Jeanloz N, Nigro N, Suter-Widmer I, Schuetz P, et al. (2016) Long-term outcome of profound hyponatremia: a prospective 12 months follow-up study. Eur J Endocrinol 175(6): 499-507.
-
Baran D, Hutchinson TA (1984) The outcome of hyponatremia in a general hospital population. Clinical nephrology 22(2): 72-76.
-
Arzhan S, Lew SQ, Todd S, Tzamaloukas AH, Unruh ML (2021) Dysnatremias in Chronic Kidney Disease: Pathophysiology, Manifestations and Treatment. Frontiers in Medicine 8: 769287.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report