PCNL as a Safe Option in Anomalous Kidneys for Stones More Than 2 Cm
Background: The incidence of anomalous kidney varies from 3-11%. Various types of anomalous kidneys exist like simple ectopic kidney, malrotated kidney, horse-shoe kidney, crossed fused ectopia, kidneys with duplex system and pelvic kidney etc. Treatment of stone disease in such kidneys is a bit different because of abnormal orientation of kidney, abnormally placed calyces and high incidence of abnormal renal vessels. Various options to deal with the stone in such kidneys include – ESWL, RIRS, PCNL, laproscopy assisted PCNL and laproscopic/robotic pyelolithotomy. Among these, PCNL is one of the recommended modalities to deal with stone disease in anomalous kidneys with the highest success rate for stone clearance. Primary aim of the study was to assess the success of PCNL in anomalous kidneys in terms of the stone clearance. Secondary aims were perioperative and postoperative complications. Methods: This retrospective study was done in SMBT IMS & RC, Nashik, India from August 2016 to July 2021. All patients were evaluated preoperatively with history, clinical examination, and blood and urine investigations, X-ray KUB, USG KUB, CT KUB and IVP. For statistical analysis, SPSS 19.0 software was used. We used standard PCNL technique of puncture followed by serial dilatation of the tract to the desired size. Minimum size of Amplatz sheath used was 20 Fr and maximum were 26 Fr. Results: Total 29 sessions of PCNL was done in 26 patients. Mean age of the patients were 30.6 years and duration of symptoms was 1-2 years. Mean haemoglobin drop was 0.8mg/dl with only three patients requiring blood transfusion. The operating time ranged from 80-120 minutes and average hospital stay was 3.8 days. Clavein grade 1 and grade 2 complications were recorded and were managed conservatively. Overall, the stone free rate immediately after surgery was 92.3% and 100% after 3 months for stone less than 4mm. Conclusion: PCNL in anomalous kidneys is technically demanding procedure but it gives much better results when compared other modalities of treatment. It is as safe as the PCNL done for a normal situated and oriented kidney. Infact, it increases the surgeon’s skills and make him more demanding for the complex cases.
Introduction
Background
Urologists deal with an anomalous kidney in their routine practice. The incidence of anomalous kidney varies from 3-11% [1]. Various types of anomalous kidneys exist like simple ectopic kidney, malrotated kidney, horse-shoe kidney, crossed fused ectopia, kidneys with duplex system and pelvic kidney etc. All these types of anomalies have problem with the drainage of urine either due to abnormal PUJ (pelvi-ureteric junction), high insertion of the ureter, abnormal vasculature or presence of isthmus leading to increased chances of stasis and stone formation.
Treatment of stone disease in such kidneys is a bit different because of abnormal orientation of kidney, abnormally placed calyces and high incidence of abnormal renal vessels. In normal located and oriented kidney, pelvis is found medially while calyces are found posteriorly. In anomalous kidneys, pelvis rotates anteriorly, and calyces are found posterolaterally so puncture becomes difficult Figures 1-4. In ectopic pelvic kidney bowels surround the kidney so laparoscopic assistance is required Figure 5. In complete duplex system, stones of superior calyx cannot be negotiated by inferior calyx and vice versa Figures 3a-3c. All these factors make PCNL different and difficult in anomalous kidneys.
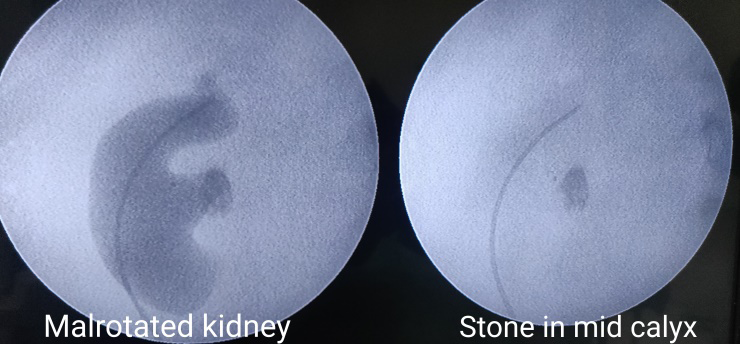
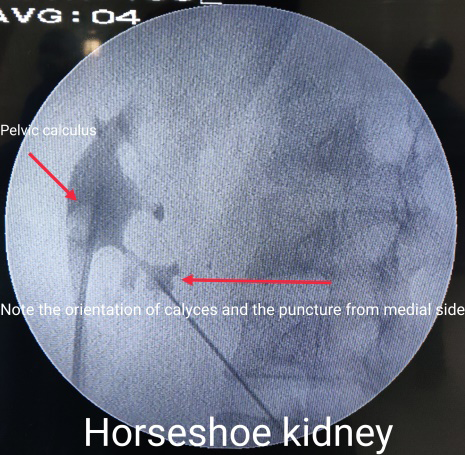
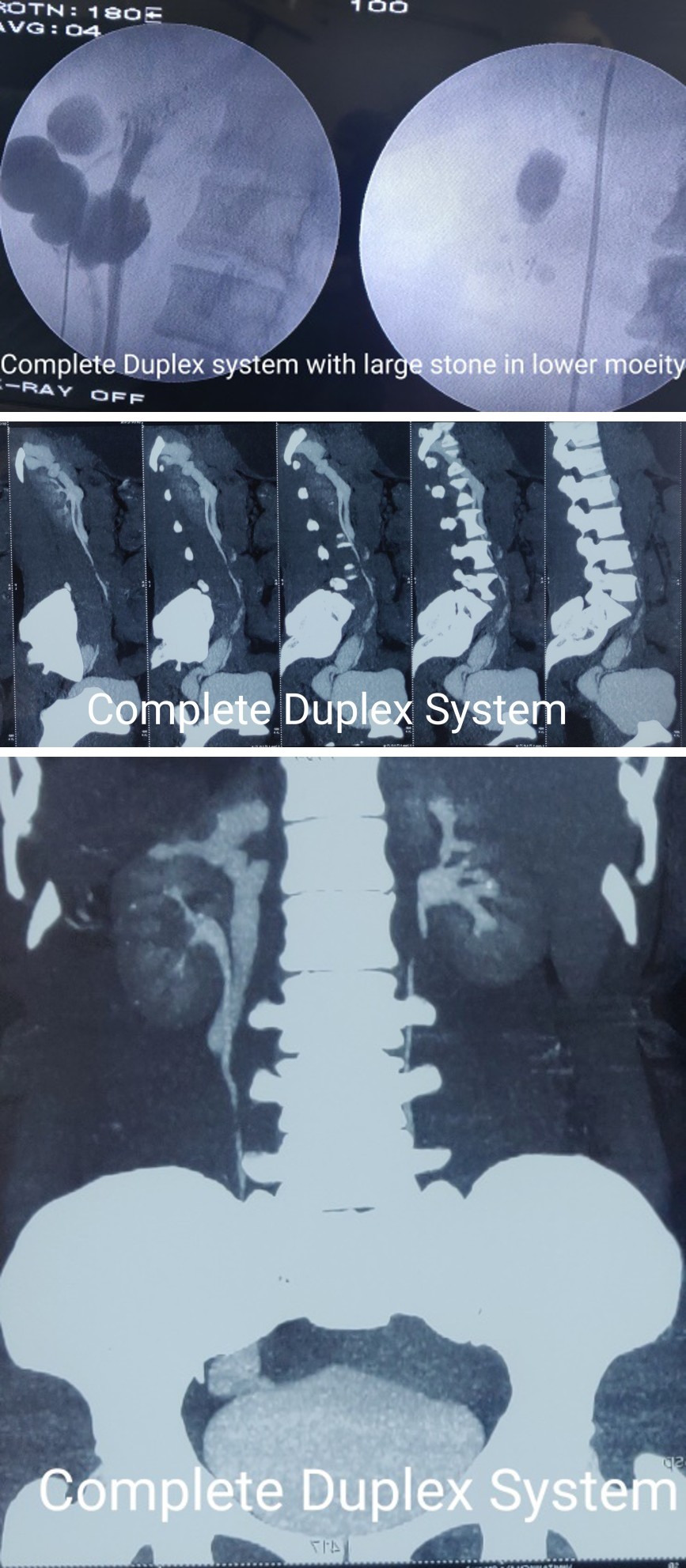
Figure 3a: Complete Duplex System.
Figure 3b: Complete Duplex Sytem 2.
Figure 3c: Complete Duplex System.

Figure 4a: Crossed ectopic Kidney.
Figure 4b: Crossed fused Ectopia.
Various options to deal with the stone in such kidneys include – ESWL (extra-corporeal shock wave lithotripsy), RIRS (retrograde intra-renal surgery), PCNL (percutaneous nephrolithotomy), laproscopy assisted PCNL and laproscopic/robotic pyelolithotomy. All these modalities have variable rate of success for treatment of renal calculi viz. ESWL for stone in ectopic kidney has success rate of 66- 71%) and in horse-shoe kidney success of around 28-80% [2]. RIRS has success of around 75% for stone clearance in anomalous kidneys [3]. Among all the above modalities to treat renal calculi, PCNL is one of the recommended modalities to deal with stone disease in anomalous kidneys with the highest success rate for stone clearance.
Methods
This retrospective study was done in SMBT Institute of Medical Sciences and Research Centre, Nashik, Maharashtra, India from August 2016 to July 2020. All records related to study were taken in detail and the data was analysed. Among these, two patients had simple ectopic kidney, three had malrotated kidneys, thirteen had horse-shoe kidneys, five kidneys were with the complete duplex system, and two were pelvic kidney and one as a crossed ectopic separate kidney.
All patients were evaluated preoperatively with history, clinical examination, complete hemogram, renal function test, liver function test, and urine analysis and urine culture and sensitivity. Ultrasonography (USG) and X-ray of kidney, ureter, and bladder (KUB) were done in all the patients. Intravenous pyelography (IVP) was done in 8 patients and Computed tomography (CT) urography in 18 patients. Diethylenetriaminepentaacetic acid (DTPA) scan was done in 4 patients, who had thin renal parenchyma due to obstruction and the function was preserved in all the cases. All data were collected in retrospective manner. For statistical analysis, SPSS 19.0 software was used.
We used standard PCNL technique of puncture followed by serial dilatation of the tract to the desired size. We used 20 Fr Wolf’s Dresden rigid nephroscope. Standard Indian pneumatic lithoclast made by Sigma Company was used for fragmentation of the stones. Minimum size of Amplatz sheath used was 20 Fr and maximum were 26 Fr.
Results
Total 29 sessions of PCNL were done in 26 patients. Mean age of the patients were 30.6 years and duration of symptoms was 1-2 years. Most of the patients presented with complaints of flank pain (46%), haematuria (18%), nausea (18%) and nonspecific abdominal pain (14%). Total 23 patients required only single session of PCNL for complete stone clearance while 3 patients underwent relook procedure. However, only one could achieve complete stone clearance. Out of 29 sessions, 24 patients had single puncture while two patients had multiple calyceal puncture for stone removal. Mean haemoglobin drop was 0.8mg/dl with only three patients requiring blood transfusion. The operating time ranged from 80-120 minutes and average hospital stay was 3.8 days. No major complications were found during intra- and post-operative period. Only Clavein grade 1 and grade 2 complications were recorded and were managed conservatively. Overall, the stone free rate immediately after surgery was 92.3% and 100% after 3 months for stone less than 4mm. Two patients with residual stones were later subjected to ESWL and were cleared of all the fragments.
Discussion
Dealing with the stone in anomalous kidney by PCNL is a bit difficult. This is due to altered orientation of the renal pelvis and calyces, altered renal vasculature, altered relations with intra-abdominal organs and relative immobility. Minimal invasive options like PCNL for stone removal are advantageous due to good stone clearance, less hospital stay, early patient recovery, and reduced requirement of analgesia. There are individual studies of minimal invasive techniques in horseshoe kidneys [4, 5, 6, 7] or pelvic ectopic kidney, [8]. Overall studies regarding PCNL in various anomalous kidneys are very less [9, 10, 11, 12, 13].
Flexible ureteroscopy (RIRS) is a good option for stones in ectopic and pelvic kidneys [3], but again it is indicated for stones less than 20mm.
The mean stone size in the present study was 3.5 cm for which PCNL should be the preferred treatment. Gaurav P, et al. has mean size of 4.4cm, Gupta NP, et al. had 2.4cm and Hussein M Abdeldaeim, et al. had mean size of 324.9 ± 191.8 mm in their study.
Flexible nephroscopy could be one option in those patients where there were complex stones in the anomalous kidney [14]. Here flexible nephroscopy can help in achieving complete clearance. In our study we were able to achieve only 92.3% clearance only, inspite of re-look nephroscopy in three patients due to the complex anatomy as we were not able to reach the desired calyx. Because of the unavailability of the flexible nephroscope, we were not able to achieve complete clearance immediately and two patients requires ancillary procedure in the form of ESWL for complete stone clearance later on.
ESWL remains one of the non-invasive options for stone clearance, but the anatomic abnormalities sometimes prevent smooth fragment passage in a number of patients. The main limitation of ESWL is that success rate of stone clearance decreases with increasing stone size. In the study by Lufti Tunc, et al. of ESWL in anomalous kidney, they had the stone‐free rates in horseshoe, malrotated, pelvic and crossed ectopic kidneys were found to be 66.7%, 56.7%, 57.2% and 25%, respectively [2]. Also, in patients with a stone >30 mm, the stone‐free rate was only 34%, compared to a rate of 92% for calculi <10 mm [2].
Location of the calculus in the kidney also has an important role in the stone clearance. Single pelvic and calyceal stones were cleared in single sitting in our study. We did complete clearance in 23 (88.4%) patients in single sitting. Prakash G, et al. Also has complete stone clearance in single session in their study [9].
There are chances of residual stone(s), if the stone bulk is more. These patients may need re-look procedure for complete clearance. In our study, we had five patients with multiple calculi. Of which 3 were completely cleared of the stone in a single session and two patients needed re-look PCNL but complete clearance was not achieved. Another patient had calculus in inaccessible calyx for which re-look nephroscopy failed. Thus overall, we did re-look PCNL in three patients and only one patient got complete clearance. Thus, we had 88.4 % clearance in single session and 92.3% clearance after second session. Prakash G, et al. Also has similar success rate in their study [9]. Gupta NP in their study had complete clearance after 7 re-look sessions [10] and Hussein M Abdeldaeim, et al. had complete clearance after one re-look procedure [11].
The most common approach for puncture in our study was middle calyx, followed by the upper calyx making 80.7% of the total. These punctures could be done avoiding the pleura owing to the malrotation and favourable calyceal position more medially. Infact, whole of the kidney can be inspected through this approach, including the upper ureter. Gaurav P, et al. had mid-calyceal puncture as the commonest approach in their study of outcome of PCNL in anomalous kidney [9]. Bannakit Lojanapiwat also had upper pole access as the most common approach in PCNL in anomalous kidneys [1]. Satav, et al. used upper calyceal approach in all the 24 renal units without any pleural injury in their study of PCNL in horse-shoe kidney [15].
Overall, we did multiple punctures in two patients (7.6%) and we were able to achieve complete clearance in one patient only. Gupta NP used two tracts in six patients for complete clearance [10] and Hussein M Abdeldaeim, et al. also used more than one tract in three patients for complete clearance [11].
PCNL in itself inherits many complications, the common being post-operative fever, minor haematuria, need of blood transfusion, nearby organ injuries, etc.
There was no pleural injury in our study. Various studies had reported various rates of pleural injury. Gaurav P, et al. Had no evidence of pleural injury in their study [9], Gupta NP had one pleural injury in their study [10], and while Lojanapiwat B, et al. had pleural effusion in their study that was managed conservatively [12].
We have 23% Clavein grade 1 complications following PCNL and 23% grade 2 Clavein complications. Out of which 3 patients required blood transfusion and other 3 required intravenous antibiotics for post-operative fever. Rest were managed conservatively with intravenous fluids and other supportive treatment. Awad Ka`abneh in their study gave blood transfusion in 3 patients (8.6%) and 16.7% patients had post-operative pyrexia [16] Gupta NP, et al. had post PCNL sepsis in two patients [10], Hussein M Abdeldaeim, et al. had fever in one case only [11] while Abdul, et al. [17] had three blood transfusions in their study.
The operating time in our study ranged from 80-130 minutes. Most of the other studies have similar operating time with minimum time starting from 25 minutes in one to maximum 150 minutes in others [10, 11, 16].
The mean haemoglobin drop in our study was 0.8mg/dl (range 0.5-1.3). Awad Ka`abneh, et al. had 2.8 mg/dl (0.9-5.1) of mean haemoglobin drop in their study [16] while Gupta NP, et al. had mean haemoglobin drop of 1.4 (0.5-1.4) in their patients [10].
The average hospital stay in our study was 3.8 days. Awad Ka`abneh, et al. Had 3.8 mean days of hospital stay in their study [16] while Gupta NP had 3.2 mean days of hospital stay in their study [10].
In our study we also operated upon five renal units of complete duplex systems. In these kidneys also, we did standard PCNL with lower and upper pole calyceal approaches and we were able to do complete stone clearance in all the patients. Gaurav P, et al. also had similar 100% success of stone clearance all the forty patients of bifid system [9].
We did laproscopic assisted PCNL in two cases and they were also uneventful and we achieved 100% stone clearance in this type of kidneys also. Ganpule A P in their study told that laparoscopic assisted PCNL has shown good clearance rates with minimal morbidity and less likelihood of any added procedures [18].
Overall, PCNL yields good stone free rates in spite of complex anatomy and large stone burden, with no difference in the post-operative complications. Patients get benefitted when they are referred and treated in high volume centres that have experience in treating these complex cases.
The limitations of the study include the retrospective nature and smaller study cohort. Further future randomised controlled trials will add further to future research. Still our study adds at least a pinch to the larger sea.
The best part of our study is PCNL in a very wide variety of the renal anomalies (Tables 1-3).
| Type of Anomalous Kidney | Number of Patients | |
|---|---|---|
| 1 | Simple Ectopic kidney | 2 |
| 2 | Malrotated kidney (Figure 1) | 3 |
| 3 | Horse-shoe kidney (Figure 2) | 13 |
| 4 | Kidney with complete duplex system (Figures 3a, 3b, 3c) | 5 |
| 5 | Crossed fused ectopica (Figures 4a,4b) | 1 |
| 6 | Pelvic kidney (Figure 5) | 2 |
Table 1: Showing the total patients and the types of anomalies.
| Age (mean age) | 30.6 years |
|---|---|
| Duration of Symptoms | 1-2 years |
| Laterality | |
| Right | 18 |
| Left | 8 |
| Stone size (mean) | 3.5cm |
| Stone configuration | |
| Pelvic | 15 |
| Calyceal | 6 |
| Multiple | 5 |
Table 2: Showing Demographic features and Stone configuration.
| Operating time | 80-120 minutes |
|---|---|
| Stone clearance in single sitting | 23 (88.4%) |
| Stone clearance in second sitting | 24 (92.3%) |
| Incomplete clearance | 2 (7.6%) |
| Hospital stay (mean) | 3.8 days |
| Calyceal puncture | |
| Upper | 8 |
| Middle | 13 |
| Lower | 5 |
| Multiple | 2 (7.6%) |
| Blood transfusion | 3 patients only (11.5%) |
| Haemoglobin drop (mean) | 0.8mg/dl (0.5-1.3) |
| Complications (Clavein) | |
| Gr 1 | 12 (46.1%) |
| Gr 2 | 5 (23%) |
| Gr 3 | Nil |
| Gr 4 | Nil |
Table 3: Showing Results of PCNL in anomalous kidneys.
Conclusion
PCNL in anomalous kidneys is technically demanding procedure but it gives much better results when compared with RIRS, ESWL and other related procedures for renal calculi specially when there is large stone bulk. It is as safe as the PCNL done for a normal situated and oriented kidney. Infact, it increases the surgeon’s skills and make him more demanding for the complex cases.
Financial Support and Sponsorship: Nil.
Conflicts of Interest: There are no conflicts of interest.
References
-
Barakat AJ, Drougas JG (1991) Occurrence of congenital abnormalities of kidney and urinary tract in 13,775 autopsies. Urology 38(4): 347-350.
-
Tunc L, Tokgoz H, Tan MO, Kupeli B, Karaoglan U, et al. (2004) Stones in anomalous kidneys: results of treatment by shock wave lithotripsy in 150 patients. Int J Urol 11(10): 831-836.
-
Weizer AZ, Springhart WP, Ekeruo WO, Matlaga BR, Tan YH, et al. (2005) Ureteroscopic management of renal calculi in anomalous kidneys. Urology 65(2): 265-269.
-
Shokeir AA, El-Nahas AR, Shoma AM, Eraky I, El-Kenawy M, et al. (2004) Percutaneous nephrolithotomy in treatment of large stones within horseshoe kidneys. Urology 64(3): 426-429.
-
Viola D, Anagnostou T, Thompson TJ, Smith G, Moussa SA, et al. (2007) Sixteen years of experience with stone management in horseshoe kidneys. Urol Int 78(3): 214- 218.
-
Jones DJ, Wickham JE, Kellett MJ (1991) Percutaneous nephrolithotomy for calculi in horseshoe kidneys. J Urol 145(3): 481-483.
-
Al-Otaibi K, Hosking DH (1999) Percutaneous stone removal in horseshoe kidneys. J Urol 162(3 Pt 1): 674- 677.
-
Maheshwari PN, Bhandarkar DS, Andankar MG, Shah RS (2004) Laparoscopically guided transperitoneal percutaneous nephrolithotomy for calculi in pelvic ectopic kidneys. Surg Endosc Other Interv Tech 18(7): 1151.
-
Prakash G, Sinha RJ, Jhanwar A, Bansal A, Singh V (2017) Outcome of percutaneous nephrolithotomy in anomalous kidney: Is it different? Urol Ann 9(1): 23-26.
-
Gupta NP, Mishra S, Anand A, Seth A (2009) Percutaneous Nephrolithotomy in Abnormal Kidneys: Single Center experience. Urology 73(4): 714-715.
-
Abdeldaeim HM, Islam M Hamdy SA, Mokhless IA (2011) Percutaneous nephrolithotomy for the management of stones in anomalous kidneys in children. J Pediatr Urol 7(3): 239-243.
-
Lojanapiwat B (2005) Percutaneous nephrolithotomy (PCNL) in kidneys with fusion and rotation anomalies. J Med Assoc Thai 88(10): 1426-1429.
-
Lim EJ , Teoh JY , Fong KY , Emiliani E , Gadzhiev N , et al. (2022) Propensity score-matched analysis comparing retrograde intrarenal surgery with percutaneous nephrolithotomy in anomalous kidneys. Minerva Urol Nephrol.
-
Raj GV, Auge BK, Weizer AZ, Denstedt JD, Watterson JD, et al. (2003) Percutaneous management of calculi within horseshoe kidneys. J Urol 170: 48-51.
-
Satav V, Sabale V, Pramanik P, Kanklia SP, Mhaske S (2018) Percutaneous nephrolithotomy of horseshoe kidney: Our institutional experience. Urol Ann 10(3): 258-262.
-
Ka`abneh A, Al-Hammouri F (2011) Large calculi within malpositioned and malformed kidneys, is percutaneous nephrolithotomy (PCNL) feasible? A Single Center’s Experience over 10 Years. Sudan JMS 6(1): 17-21.
-
Rana AM, Bhojwani JP (2009) Percutaneous Nephrolithotomy in Renal Anomalies of Fusion, Ectopia, Rotation, Hypoplasia, and Pelvicalyceal Aberration: Uniformity in Heterogeneity. Journal of Endourology 23(4): 609-614.
-
Ganpule AP, Desai MR (2011) Urolithiasis in kidneys with abnormal lie, rotation or form. Current Opinion in Urology 21(2): 145-153.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report