The Molecular Profile of the Urothelial Carcinoma of the Prostate
A 59-year-old-man presented with haematuria and dysuria. Concerning the pathological diagnostic a common problem was in this case to differentiate between high-grade urothelial carcinoma and high-grade prostate adenocarcinoma. The following immunohistochemical profile was found: keratin 7+, keratin 8/18 +; keratin 20+; AE1/AE3+; Ki 67+; p53+; S100-; chromogranin A-; vimentin -; PSA-. The molecular profile was a key element for establishing a correct therapeutic approach.
Introduction
Prostate cancer is the second most frequent malignancy in males after lung cancer, and in most of cases consists of a diffuse proliferation of prostatic acini. This glandular neoplasm is characterized by the proliferation of acini and only a few cases show less differentiated features. Besides conventional glandular tumours, which comprise more than 90%, there were described some rare histological variants, like primary urothelial carcinoma of the prostate [1]. Primary urothelial carcinoma of the prostate (PUC) is a rare malignant solid tumor (1% to 5% of all prostatic carcinomas) which was first described by Ende, et al. In 1963 as an aggressive behaviour malignancy with a very poor prognosis, owing to the strong tendency of distant metastasis in organs such as bladder, seminal vesicle, and ureter [2].
Patients admitted with the suspicion of primary urothelial carcinoma present nonspecific symptoms, such as haematuria, obstructive voiding, and similar symptoms to the main manifestations of benign prostatic hyperplasia or prostatic adenocarcinoma. Digital rectal examination of the prostate constantly shows an enlarged and hard prostate [2]. As laboratory parameters are mostly in normal ranges, the diagnosis of prostatic urothelial carcinoma is mainly based on pathology and immunohistochemistry, this type of tumor, being positive for CK7, CK20, P63, GATA-3 and uroplakin. Furthermore, prostatic urothelial carcinoma is generally negative for PSA and P504 s, which is also significant for differential diagnosis [3].
Treatment strategies for prostatic urothelial carcinoma are multimodal, including surgery, adjuvant chemotherapy, and radiotherapy. Some authors presented the benefits of intravesical instillation of Bacillus Calmette-Guérin (BCG) for carcinoma in situ (CIS), after complete resection of the tumor [4]. When prostatic stromal invasion is identified, radical cystoprostatectomy should be performed. Not much information is available so far in the literature regarding the results of chemotherapy in patients with prostatic urothelial carcinoma. The current adjuvant chemotherapy regimens of prostatic urothelial carcinoma include doxorubicin, cyclophosphamide, and cisplatin. When the tumor is limited to the prostate tissue or pelvis, radiotherapy is also recommended [5, 6].
Material and Methods
Here we present the case of a 59-year-old patient who was presented to the Department of Emergency of the City Emergency Clinical Hospital of Timisoara with hematuria and dysuria. A morpholological staining examination from cystoscopy biopsy revealed a presumptive urothelial carcinoma of the prostate. But a clear differential diagnosis was necessary. The immunohistochemical staining was performed. Keratins 7, 8/18, 20, AE1/3 and Ki67, p53, chromogranin A, S100, vimentin and PSA were used as primaries antibodies. All antibodies were ready to use, from Leica Biosystem Newcastle Ltd, Newcastle Upon Tyne, UK. After the pre-treatment and peroxide blocking, the incubation time with primary antibodies was 20 minutes. The visualization was realized by using the Bond Polymer Refine Detection System. 3, 3 diaminobenzidine was used as chromogen and hematoxylin as counterstain. The entire immunohistochemical procedure was performed with Bond Max autostainer (Leica Biosystem). The evaluation of the slides, pictures capture, and processing were performed by using Grundium Ocus 40 microscope (Hermiankatu 6G, 33720 Tampere, Finland). The patient therapy consists of adjuvant treatment.
Results
Hematoxylin and eosin staining method shows a malignant cell proliferation, represented by cells with abundant, clear cytoplasm and enlarged atypic nuclei. In the periglandular stroma it was identified a chronic inflammatory infiltrate, mainly formed by lymphocytes and plasmocytes surrounded by blood vessels Figure 1a.
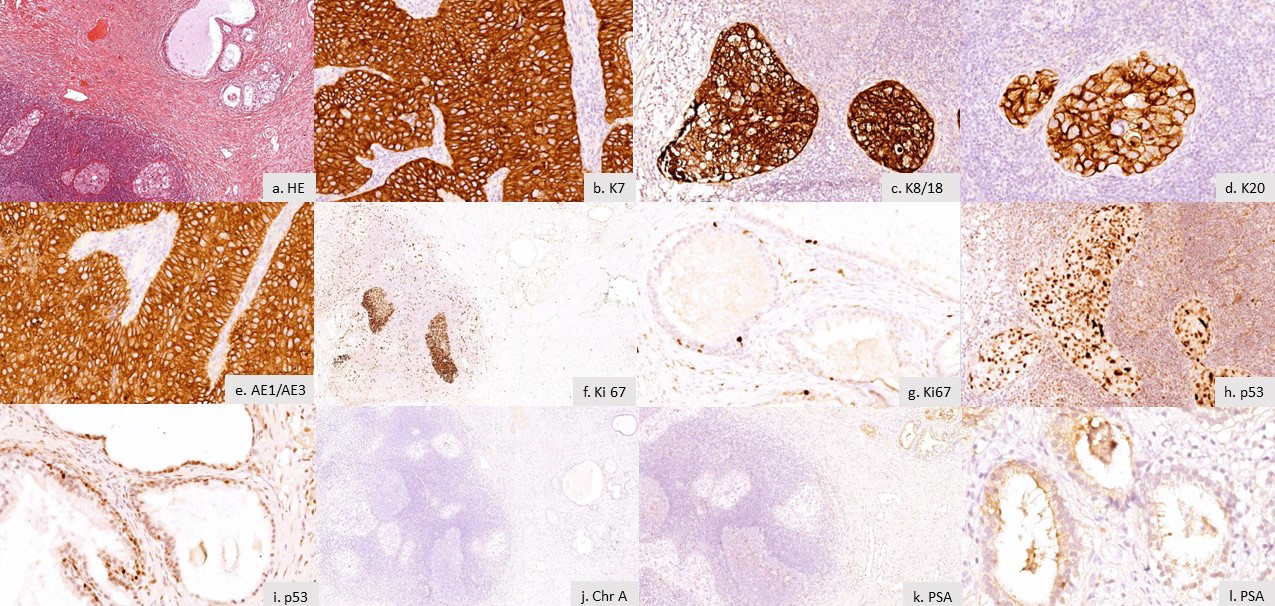
Figure 1: The molecular profile of the urothelial carcinoma of the prostate. a) HE staining, x 10 magnification. b) Immunoexpression of keratin 7 in the tumor area, x 40 magnification. c) Positivity of keratin 8/18 in the tumor area, x 20 magnification. d) Keratin 20 positive tumor cells, x 40 magnification. e) Immunoexpression of keratin AE1/AE3 in tumor cells, x 40 magnification. f) Ki 67 Immunoexpression in more than 80% of tumor cells, x10 magnification. g) Ki67 expression in the basal cells of the normal prostate glandular epithelium.h) p53 nuclear expression in the tumor cells, x 40 magnification. i) p53 positivity in the basal cells of the normal prostate glandular epithelium, x 40 magification. j) Negative reaction of chromogranine A in the tumor cells, x10 magnification. k) Absence of PSA expression in tumor cells, x 10 magnification. l) PSA Immunoexpression, in principal cells of the prostate glandular epithelium, x 40 magnification.
For both immunohistochemical markers: K7 and K8/18 it has been noticed a homogenous cytoplasmatic expression in all cells from the tumor area Figures 1b, 1c. Even more, the K20 expression was characterized by a homogenous distribution in every tumor cell of the area, similar as the positivity of the AE1/3, where intensity of expression was 3 Figures 1d, 1e. Immunoexpression of Ki67 has been identified in more than 80% of the nuclei, in tumor cells. The intern positive control was noticed at the level of basal cells from the glandular epithelium of the normal prostate Figures 1f, 1g.
P53 was positive in more than 80% of the tumoral cells nuclei with an expression of 3. We identified heterogenous expression according to the tumor area: tumoral cells with an expression of 3 situated at the periphery, and those with a 2 expression, in the central area. Moreover, it has been noticed that peritumoral inflammatory cells presented an expression of 2 regarding P53. The proper immunohistochemistry technic has been validated by the basal cell nuclei positivity of the normal prostate glandular epithelium Figures 1h, 1i.
Chromogranin A expression at the level of tumoral cells has been negative, but the intern positive control showed positivity of the neuroendocrine cells from the normal prostate glandular epithelium Figure 1j. Even though Immunoexpression of the S100 protein has been negative in tumor cells, the reaction was identified at the level of peritumoral connective tissue cells: macrophages and follicular dendritic cells. Furthermore, vimentin expression inside tumoral area was negative, but with an intern positive control Figures 1k, 1l.
Discussion
According to literature, both age and symptoms of patients presenting this diagnostic are heterogenous. On one hand, Zhou J, et al. exposed a case of a 55-year-old man who was admitted at the hospital due lower urinary tract obstructive symptoms that lasted for 5 years. On the other hand, Zhang S, et al. presented a 77-year-old man case who accused recurrent gross hematuria for 3 months with a fever for 1 month. Having an extremely low incidence rate, primary PUC is mainly diagnosed using a combination between morphologic and immunohistochemistry staining methods. HE staining usually show many small nests, often with marked nuclear pleomorphism and variably presents nucleoli.
Most of the patients are at an advanced stage with distant metastasis at diagnosis moment. It has been confirmed that PSA level measurement plays an important role in the differential diagnosis of bladder cancer from prostate cancer. However, PSA is also expressed in extra-prostatic neoplasms, such as urethral, periurethral, perianal glands, salivary duct carcinoma, salivary gland adenoma, and rare breast carcinomas. Given the limitations of PSA, the clinical differential diagnosis becomes more difficult [7]. Liedberg, et al. showed primary PUC had a unique and separate staging system, which was different from the prostatic adenocarcinoma [8]. Radical surgery should be pursued for patients with PUC who are in the early stage of disease. For advanced-stage PUC, gemcitabine combined with cis- platinum is the first-line chemotherapy regimen. Lchihara, et al. study suggested that primary PUC patients with stromal invasion or lymph node metastasis have worse prognosis [9].
Conclusion
Primary urothelial carcinoma of the prostate involves the urinary system, being associated with a poor prognosis. This case report emphasizes the importance of the molecular profile in these patients, and its importance in diagnosis, differential diagnosis and the therapeutic approach.
References
-
Rawla P (2019) Epidemiology of Prostate Cancer. World J Oncol 10(2): 63-89.
-
Zhou J, Yang C, Lu Z, Zhang L, Yin Y, et al. (2019) Primary urothelial carcinoma of the prostate. A rare case report. Medicine (Baltimore) 98(3): e14155.
-
Liang Y, Heitzman J, Kamat AM, Dinney CP, Czerniak B, et al. (2014) Differential expression of GATA-3 in urothelial carcinoma variants. Hum Pathol 45(7): 1466-1472.
-
Cui J, Wang W, Chen S, Xiang P, Yue Y, et al. (2016) Combination of Intravesical Chemotherapy and Bacillus Calmette-Guerin Versus Bacillus Calmette-Guerin Monotherapy in Intermediate- and High-risk Nonmuscle Invasive Bladder Cancer: A Systematic Review and Meta- analysis. Medicine (Baltimore) 95(3): e2572.
-
Kohei N, Sugiyama K, Chihara I, Muro Y, Imamura M, et al. (2018) Impact of relative dose intensity in gemcitabine- cisplatin chemotherapy for metastatic urothelial carcinoma. SAGE Open Med 6: 2050312118783011.
-
Lorenzo GD, Buonerba C, Bellelli T, Romano C, Montanaro V, et al. (2015) Third-Line Chemotherapy for Metastatic Urothelial Cancer: A Retrospective Observational Study. Medicine (Baltimore) 94(51): e2297.
-
Zhang S, Guo Z (2018) Case report of a primary prostatic urothelial carcinoma patient with sustained fever. Onco Targets and Therapy 11: 4547-4550.
-
Liedberg F, Chebil G, Månsson W (2007) Urothelial carcinoma in the prostatic urethra and prostate: current controversies. Expert Rev Anticancer Ther 7(3): 383- 390.
-
Ichihara K, Masumori N, Kitamura H, Hasegawa T, Tsukamoto T, et al. (2014) Clinical outcomes of urothelial carcinoma of the prostate detected in radical cystectomy specimens. Int J Clin Oncol 19(1): 152-156.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report