Intra Testicular Leiomyoma: First Case Report from an Ethiopian Patient
Leiomyomas are benign tumors arising from smooth muscle cells myometrium being most common site of origin. Capsule of kidney is most common site of origin in male Genito urinary system. Testicular parenchyma is an extremely rare site where tumor presents as a painless, slowly growing mass. It is very difficult to diagnose this lesion preoperatively as ultrasound features are nonspecific. Microscopic evaluation only renders an exact diagnosis. Intraoperative frozen section biopsy followed by local excision is the current treatment of choice but if not available radical orchidectomy would be done. We report case of intratesticular leiomyoma in a 32-year-old Ethiopian patient.
Introduction
Smooth muscle fiber consisting of organ or structure can be an origin of Leiomyomas which are benign mesenchymal tumors. Majority of cases are seen in mid adult years arising commonly from uterus, small bowel, and esophagus.
Capsule of the kidney is the most common site of origin in the male genital and urinary system. In the mentioned systems other common sites of origin include tunica albuginea, spermatic cord, and epididymis. Intratesticular leiomyomas are rarely reported around the world. Here we report the first case of intratesticular leiomyoma from an Ethiopian patient highlighting its diagnostic and treatment aspects [1, 2].
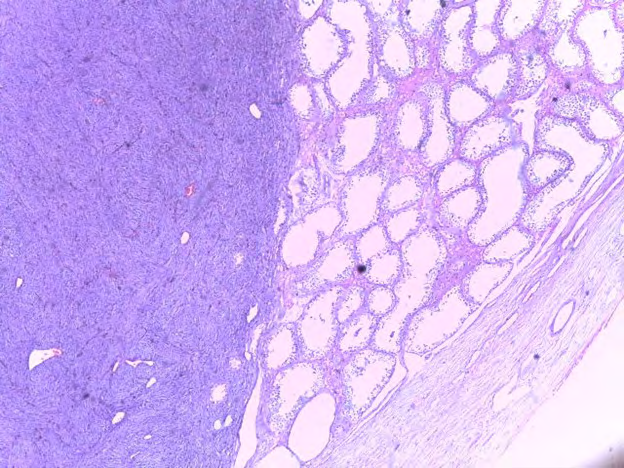
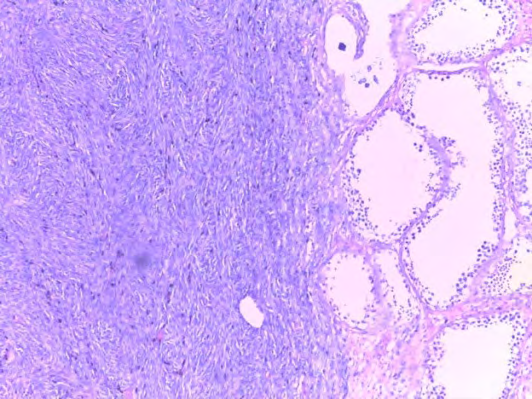
Right orchidectomy biopsy specimen was received at department of pathology from a 32-year-old male patient. Up on review of clinical, radiologic and laboratory data his presentation was with a firm to hard right testicular mass with no associated pain growing slowly over a period of three years. The ipsilateral spermatic cord, epididymis as well contralateral testis, spermatic cord and epididymis were normal. Tumor marker studies including α feto protein (AFP) and β human chorionic gonadotropin (HCG) levels were normal. Ultrasonography (US) showed hypo-echoic lesion with central iso-echoic area in the upper pole of right testis. With a preoperative diagnosis of seminoma Patient underwent radical inguinal orchidectomy. Gross Examination of the specimen revealed a circumscribed solid mass at upper pole of testis. Cut section revealed well circumscribed 3X2X2 CMS, grey - white, firm solid mass with whirling pattern (Figure 1). The rest of testicular parenchyma and pretesticular tissue was normal. Microscopic examination displayed circumscribed proliferation of spindle cells with cigar shaped nuclei in interlacing pattern without nuclear atypia or mitosis. No area of necrosis (Figures 2 & 3). These microscopic findings are in keeping with histologic diagnosis of intratesticular leiomyoma. Clinical, radiologic and laboratory follow up was normal warranting no additional therapy.

Discussion
Benign mesenchymal neoplasms arising from smooth fibers are known as leiomyomas. Myometrium is the most common sites of origin. In male genital and urinary system cases have been seen to arise from renal capsule, Para testicular tissue, urinary bladder, prostate, and glans penis. Testicular parenchyma is an extremely uncommon site of origin. Currently, the Contractile cells in the tunica propria of seminiferous tubules are thought to be the cells of origin of this tumor with unknown pathogenesis, [2, 3]. Majority of patients typically are middle aged individuals presenting with a slowly growing painless solid mass [4]. In patients presenting with intratesticular solid mass malignant tumors including seminomas, lymphomas, germ cell tumors and metastatic tumors are common causes but epidermoid cyst, Leyding cell hyperplasia, fibroma, hemangioma, leiomyoma, spontaneous hemorrhages, sarcoidosis, and tuberculosis should also be entertained as a differential diagnosis. Ultrasound is the preferred radiologic investigative method in evaluating disease of the scrotum. Leiomyoma has no defined sonographic features, but findings include homogenous echogenicity or heterogeneous mass. During ultrasound examination variations in overall sonic output may result in variation of the echogenicity from low too high in turn making it difficult to differentiate leiomyoma from malignant tumors and for these reasons it is only histopathologic evaluation which renders the exact diagnosis. On gross examination of resected specimen, leiomyomas are well-circumscribed with a whorled cut surface. In addition to leiomyoma, intratesticular smooth muscle tumors include atypical leiomyoma and leiomyosarcoma. Differentiation among these entities is possible only after evaluating the tumor with the following set of Morphologic criteria.
1) Tumor size of greater or equal to five CMS along greater dimension 2) invasive margin; 3) greater than or equal to five mitotic figures per 10 high power fields; and 4) moderate cytological atypia. Leiomyoma will be diagnosed if the tumor shows only one of the features; those showing two features are diagnosed as atypical leiomyomas and diagnosis of leiomyosarcoma will be made if tumor shows three to four of the listed features. Despite its benign nature, treatment usually consists of radical orchidectomy as it is difficult to make a preoperative diagnosis of leiomyoma.
The proposed current treatment is local excision. Radical orchiectomy is preserved in cases where malignancy is suspected or in cases where there is extensive fibrosis adhering it to nearby normal testicular parenchyma, otherwise it is unnecessary. Frozen section is helpful in determining the type of procedure if those conditions are encountered. In setups where frozen section is not available, radical orchiectomy is the main treatment method [5].
Conclusion
Intratesticular leiomyoma is an extremely uncommon benign tumor presenting as a painless, slowly growing mass and should be considered in the differential diagnosis of any scrotal mass. Unnecessary orchidectomies have been performed as it is very difficult to make an exact preoperative diagnosis differentiating it from the more common malignancies and only histological examination validates its diagnosis. An intraoperative frozen section biopsy only allows for the test is to be salvaged.
Consent for Publication
Written informed consent was obtained from the patient for publication.
Declaration of Competing Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Acknowledgments
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
-
Sharma M, Brar N, Sidhu BS, Manjari M , Madan M (2014) Leiomyoma of scrotum, a case report of rare testicular tumor and review of literature. International Journal of Advanced Research 2(12): 217-219.
-
Asanad K, Remulla D, Nassiri N, Ghodoussipour S (2020) Leiomyoma of the testis: case report, review of literature, and discussing the role of contrast-enhanced ultrasound. Urology Case Reports 31: 101168.
-
Seubsang B (2014) Leiomyoma of Testis: A Case Report and Literature Review. Thai J Surg 35(1): 24-27.
-
Baliyan A, Dhingra H, Bhagat R (2017) Leiomyoma of Testis –Rare Benign Mimicker of Testicular Malignancy. Journal of Clinical and Diagnostic Research 11(10): ED08-ED09
-
Bedir R, Yilmaz R, Eren H (2017) Intra-testicular leiomyoma: A case report. J Clin Anal Med 8(3): 206-208.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report