Lower Urinary Tract Symptoms and Urodynamic Findings in Hemodyalisis Patients
Urodynamics is the more accurate diagnostic tool to assess functional alterations of lower urinary tract. International guidelines provide specific indications to adopt this test for the evaluation algorithm of patients with lower urinary tract symptoms. Although recent innovations in diagnostic methodologies, especially regarding ultrasounds, have reduced the use of urodynamics compared to the past, this procedure retains its importance in specific conditions, such as in patients with neurogenic lower urinary tract dysfunction, when symptoms do not improve after first line therapeutic approaches, especially in cases of complicated urinary incontinence and bladder outlet obstruction. Among patients’ cathegories who are often requested to provide urodynamic data are those undergoing hemodialysis. In these subjects urinary symptoms often develop reducing quality of life and increasing the risk of severe sistemic complications. Furthermore, bladder outlet obstruction and other alterations that increase the risk of vesico-ureteral refluxes and chronic urinary retention have to be excluded before a kidney transplant. Urodynamics can properly assess lower urinary tract dysfunction of patients undergoing hemodialysis, who are often oliguric and anuric, and therefore suffering for bladder atrophy with impaired function. This alteration is frequently responsible for recurrent inflammatory disorders of the lower urinary tract. Considering these aspects and lack of data provided by Literature on this topic, aim of this study was to assess the prevalence of lower urinary tract symptoms in a cohort of patients undergoing hemodialysis and to investigate their urodynamic findings. The results show that lower urinary tract symptoms are prevalent in patients attending our hemodialysis center, being inflammatory disorders the most represented as a consequence of bacterial urinary tract infections. Lower urinary tract symptoms, especially urinary burning, frequency, urgency and nocturia, resulted to be the third reason for seeking medical assistance by patients, following cardiovascular and respiratory symptoms. Urodynamics showed in all patients a reduced cystometric capacity, often associated with reduced compliance and detrusor overactivity; pressure / flow studies provided evidence either of bladder outlet obstruction and underactive detrusor.
Introduction and Aim of the Study
Urodynamic (UD) is the measurement of the relevant physiological parameters of the lower urinary tract to assess its function and dysfunction. This instrumental examination is performed under specific indications, for the specialized management of lower urinary tract symptoms (LUTS), and following specific guidelines that standardize the procedure [1]. Urodynamics is usually adopted during the diagnostic algorythm of the lower urinary tract especially in particular conditions, such as the assessment of neurogenic lower urinary tract dysfunction (NLUTD), in case of complicated urinary incontinence (UI) or in patients suffering from LUTS resistant to first line treatments [1]. Among patients’ cathegories that are requested to provide urodynamic outcomes are those waiting for renal transplant, because risk factors that can affect the health of the transplanted kidney should be excluded or treated before surgery. Many patients who are in waiting list for a kidney transplant undergo to chronic dialysis treatment, and most of them are oliguric or anuric since many years. Despite this conditon of reduced diuresis, LUTS are often reported by patients undergoing haemodialysis [2], therefore requiring diagnostic procedures and specific treatments. However, there is a lack of studies focusing the attention on this topic, and very poor data are available about the use of urodynamic examination for the assessment of LUTS in these patients [3]. In our clinical practice, working at a large hemodialysis center, we have noticed that LUTS are one of the most frequent reasons for demanding medical assistance by patients. The onset and recurrence of LUTS in patients suffering from end stage renal disease (ESRD) may be often associated with severe complications [4]. Furthermore, it can negatively affect their quality of life (QoL), which is already impaired due to the hemodialysis treatment [5]. Preserving the anatomical and functional integrity of the lower urinary tract is therefore important in hemodialysis patients because, in addition to allow the preservation of a good QoL and to limit the occurence of systemic complications, it is essential to ensure long-term success in case of renal transplant [6]. Considering these aspects and the poor Literature available on this topic, we designed a prospective recording of data regarding LUTS in patients attending our hemodialysis center from january 2019 to september 2022 aiming to assess the prevalence of LUTS and their UD outcomes.
Methods
Clinical, laboratory, and instrumental outcomes have been recorded and subsequently extracted from an electronic database system (Gepadial Sotware, info@ gepadial.net). Data management is under the responsability of the chief of our hemodialysis center and all patients have authorized the use of data (anonimously) by signing an informed consensus. All clinical (history), laboratory exams and instrumental assessments of patients with LUTS attending our centre from january 2019 to semptember 2022 have been collected. Basing on the outcomes provided by previous studies on this topic, we investigated in the charts of patients the following symptoms and clinical signs: urinary urgency, urinary frequency, nocturia, urinary incontinence, urinary burning, poor voiding flow, haematuria. We have classified the prevalence of these findings counting how many times we found them in the patients flow-charts. To assess prevalence of LUTS in this population, also symptoms not related to the lower urinary tract and reported by patients during the same time-interval have been collected to make a comparison. Data collected from the analysis of patients’ charts were statistically analyzed. Specifically, demographic data were assessed using the Student T test, while Chi-Square test was utilized for nominal data. In addition, possible correlations between type of symptoms, patients’ age and dialytic age were calculated using the Spearman Correlation Test.
Results
A total number of 145 patients has attended our haemodialysis center during all the time interval considered for this study and they represented our cohort. All patients were caucasian, mean age resulted 68,6 (range 22-88), 65 were women (44,8%) and 80 (55,1%) were men. All patients suffered from ESRD due to the following medical conditions: diabetes (19,3%), blood hypertension (17,9%), glomerulonephritis (16,5%), chemotherapy (13,7%), polycystic kidney disease (13,7%), abuse of non-steroid- anti-inflammatory drugs and other toxic agents (7,5%), long term bladder outlet obstruction due to benign prostatic hyperplasia, urinary stones, prostatic cancer or urothelial cancer (5,5%), other minor conditions mostly including immunologic disorders (6,8%). Mean dialytic time of the population enrolled was 48,46 months (range 2-73). Age time and dialytic time did not show statistically significant difference between the two sexes. The rate of patients with diuresis (reduced) was 37,2% (54/145 patients). Table 1 shows main characteristics of study population.
| 145 | ||
|---|---|---|
| Race of patients | 100% caucasian | |
| Mean age | 68,6 (22-88) years | Men (66,2; range 21-86) yearsWomen (64,5; range: 25-88) years |
| Sex | 65 women (44,8%), 80 men (55,1%) | Castleman syndrome; Lupus erythematosus; sclerodermia; muscle dystrophy |
| Causes of ESRD | Diabetes (19,3%) | Castleman syndrome; Lupus erythematosus; sclerodermia; muscle dystrophy |
| Causes of ESRD | Blood hypertension (17,9%) | Castleman syndrome; Lupus erythematosus; sclerodermia; muscle dystrophy |
| Causes of ESRD | Glomerulonephritis (16,5%) | Castleman syndrome; Lupus erythematosus; sclerodermia; muscle dystrophy |
| Causes of ESRD | Chemotherapy (13,7%) | Castleman syndrome; Lupus erythematosus; sclerodermia; muscle dystrophy |
| Causes of ESRD | Polikystic kidney disease (13,7) | Castleman syndrome; Lupus erythematosus; sclerodermia; muscle dystrophy |
| Causes of ESRD | NSAD (7,5%) | Castleman syndrome; Lupus erythematosus; sclerodermia; muscle dystrophy |
| Causes of ESRD | Urinary tract obstruction including bladder outlet obstruction (5,5%) | Castleman syndrome; Lupus erythematosus; sclerodermia; muscle dystrophy |
| Causes of ESRD | Other conditions (6,8%) | Castleman syndrome; Lupus erythematosus; sclerodermia; muscle dystrophy |
| Mean dialytic age | 48,46 months (range 6-83) | Men: 39,7 (range 8-83); women 36,4 (range 9-82) |
Table 1: The main characteristics of population enrolled in the study are reported.
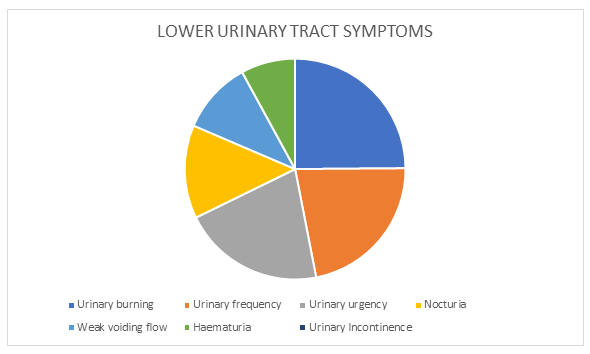
The most reported LUTS, indicated as number of records during the time of study, were urinary burning (n. 122), followed by urinary frequency (n. 108), urinary urgency (102), nocturia (n. 67), poor voiding flow (n. 52), haematuria (n. 39), and UI (n. 22) (Figure 1).
Comparing the reports between sexes, a significant difference of symptoms’ prevalence was found regarding UI (n. 18 in females vs n. 4 in males), poor voiding flow (reported only by men), and nocturia (n. 40 in males vs 12 in females). These reported symptoms were related to the following pathologic conditions achieved by the diagnostic procedures prescribed by clinicians of our center: urinary tract infections (UTI) of bacterial origin (n. 98 events recorded in 55 patients respectively; 2 cases of urinary tubercolosis), benign prostatic hyperplasia (n. 44 male patients), urinary stones (41 cases, 33 in men and 8 in women), genital prolapse (in 11 women), bladder tumors (10 patients, 6 males and 4 females), kidney tumor (2 male patients suffering from Polikysitic Kidney Disease), chronic rejection of transplanted kidney (1 male patient). In the male cohort, 23 subjects (28%) reported to assume alpha-blockers (5 patients tamsulosin, 11 patients silodosin, 7 patients alfuzosin) and 5 of them assumed also dutasteride. The total number of recorded events (symptoms) attributable to LUTS was 512. Therefore, LUTS were the third reason for seeking medical assistance by the study population, after symptoms of the cardiovascular system (n. 899), and respiratory system (n. 754). Lower urinary tract symptoms were prevalent compared to some other conditions, recorded with a significantly lower frequency, such as abdominal pain (n. 475), bone and joint disorders (n. 441), sleep disturbances, headache (n. 221), dermatological alterations (n. 214), symptoms related to electrolyte alterations, in particular hyperkalaemia (n. 190), symptoms referable to neurological events (n. 39).
Patients with lower dialytic age and residual renal function had more nocturia than those with longer one and anuric (coefficient -0,22, p<0,01). Urinary urgency and UI resulted significantly associated with diabetes mellitus either in men and in women (correlation coefficient 1,16, p>0,01), and to blood hypertension in men (correlation coefficient 1,11 p>0,01). Urodynamic investigation was prescribed by the urologist consultant to 41/145 patients (28,2%) during the time interval of the study. In this sub-group, 31 patients were males (mean age 59, range 22-72 years) and 10 were females (mean age 66, range 44-71 years). In the male cohort, the UD was requested due to the following reasons: persistent urinary frequency associated with urinary and / or urgency UI resistant to pharmacologic therapy, recurrent bacterial UTI, often associated to fever with urinary burning, bladder pain with no evidence of UTI. In the female group the UD was prescribed in subjects suffering from stress UI or urgency UI resistant to pharmacologic treatment, bladder chronic pain, recurrent UTI. Among patients submitted to UD, in 9/41 individuals (6 men, 3 women), the total amount of urine recorded per 24 hours was poor (< 200 mls). A standard UD procedure was administered in all the patients following the Good Urodynamic Practice [1], using a Medtronic device equipped with DuetR Software. All patients have been examined in sitting position after signing an informed consensus. Cystometry was performed through a 6 double lumen catheter to fill the bladder and record vesical pressure, and a rectal balloon to record abdominal pressure. Antibiotic prophylaxis was administered in all the subjects using ciprofloxacin 250 mg / 24 hours starting 24 hours before the test and continuing up to 48 hours after. Filling cystometry was achieved by administrating 30 ml/min of sterile saline (0,9% NaCl) solution at room temperature until maximum cystometric capacity was obtained, and consequently pressure / flow study was performed. The reduced speed of filling cystometry instead of standard 50 ml/min was adopted in these patients considering that most of them had no diuresis since many years (atrophic bladder). The following most represented outcomes were assessed during UD (Figure 2): all patients had a reduced cystometric capacity (ranging from 125 to 309 mls, median value 189 mls); reduced compliance was found in 33/41 patients, and detrusor overactivity in 19/41 patients.
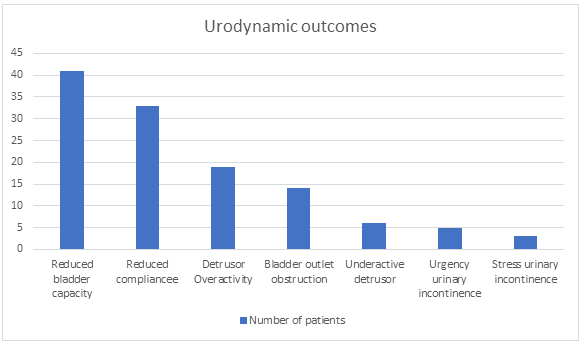
Detrusor overactivity was severe (detrusor pressure ranging from 75 to 99 cm H2O) in 7 subjects and associated with UI in 5 patients (detrusor leak point pressure ranging from 78 to 81 cmH2O). Eleven males and 3 females presented a bladder outlet obstruction due to bening prostatic hyperplasia in men and genital prolapse in women; in 4 females and 2 males bladder underactivity was observed. Two patients suffering from detrusor overactivity and affected by recurrent fever and UTI were then submitted to cystography at an external radiologic center that allowed to diagnose a vesico-ureteral reflux (bilateral in 1 subject, and bilateral in the other one). Stress UI as a consequence of intrinsic sphincteric deficiency (Valsalva leak point pressure < 25 cm H2O) was observed in 2 females. None patient reported complications after the UD. Compliance was good in all the subjects.
Discussion
There is a lack of data about LUTS in patients undergoing hemodialysis and even less data is available about UD outcomes [7]. This was the main reason inducing us to conduct a specific survey to produce consistent data on this topic. The results support the evidence that LUTS are prevalent in patients attending our hemodialysis center. In fact, LUTS were the most frequent cause for seeking medical assitance following cardiovascular and respiratory symptoms (including among the cardiovascular symptoms also those secondary to vascular access troubles). From our analysis it is evident that the most frequent urinary symptom reported by patients was urinary burning, while the most frequent clinical event (diagnosis) was represented by bacterial UTI. This outcome is in accordance with some data provided by Literature. In fact, as previously reported by other studies, UTI are common in patients undergoing hemodialysis (even in oliguric and anuric individuals) and some cathegories (as those suffering from polykistic disease) are considered at risk of severe complications [7]. Basing on these outcomes, some authors investigated the controversial of antimicrobial drug urine concentrations in hemodialysis showing high rate of clinical and microbiological cure in the treatment of oliguric and anuric hemodialysis dependent patients [8]. Therefore, it is important to assess the functional aspects of lower urinary tract in patients undergoing hemodialysis, even if asymptomatc, to prevent the development of LUTS that can lead to severe complications potentially at risk for life. Among the other symptoms reported, it was evident that voiding ones were more represented in men than in women, while UI was prevalent in women. Other symptoms, as urinary urgency and urinary frequency, were equally distributed in the population without significant difference among sexes. The association between nocturia and dialytic age that we found in our study is consistent with data already shown by other authors in previous studies [7]. Specifically, other Authors have found nocturia was a prevalent condition in ESRD patients (63.8% undergoing hemodialysis and 57.7% undergoing peritoneal dialysis) [7]. Nocturia is a disabling symptom [9] and in dialysis patients, who already have a reduced QoL due to renal disease, it further worsens QoL [6]. In our study, event it did not resulted statistically significant (p = 0,66), 21% of patients suffering from nocturia were diabetics. Diabetes was also a condition slightly associated to patients reporting irritative and voiding symptoms (respectively 18% and 19.5% of patients, p = 0,85). This outcome has already some evidence from Literature: previous studies clearly show that people suffering from diabetyes can develop bladder symptoms, that usually are represented by irritative disorders in the early stage of the disease and move to voiding symptoms in the late one [9]. This evidence even more supports the importance of periodically assess the condition of lower urinary tract function in patients undergoing hemodialysis, using also instrumental tools like UD in selected cases. An important aspect of our study concerns UD outcomes. Data from cystometric and pressure/flow studies in the study population show the prevalence of alterations of the bladder filling phase. All the patients presented a reduced cystometric capacity, with an earliness of the strong desire to void the bladder, and also a reduced bladder compliance. In many cases the reduced bladder compliance was associated with detrusor overactivity, almost always of low amplitude, especially in patients with very low residual diuresis and in anuric patients. In addition, some patients have reported pain upon reaching the cystometric capacity. All these findings are probably consequent to the progressive loss of bladder filling and emptying function that causes bladder atrophy and detrusor hypotonia [10]. Moreover, previous studies, supported by anatomopathological findings, documented that especially in patients undergoing long term hemodialysis, anatomical changes (muscle cells atrophy, vacuolar change of smooth muscle cells) are responsible for functional alterations (reduced compliance, hypersensitivity, detrusor overactivity) that are associated to bladder symptoms and may increase the risk of complications after renal transplant [11, 12]. Urodynamic findings provided by our experience can be considered the consequence of these morpho-functional changes. However, Literature is very poor of data on this aspects, and UD outcomes have been not enough investigated. Therefore, it has been not possible to assess a comparison of our findings with those provided by many other studies. Bladder hypersensitivity, poor bladder compiance, and detrusor instability were found only in one study performed in 2011 on a large cohort of patients undergoing hemodialysis and peritoneal dialysis [2]. These authors explored prevalence and type of LUTS using the International Prostate Symptoms Questionnaire. This study has the advantage of a very numerous population and highlights the evidence that in these subjects bladder alterations and storage symptoms are well represented. Furthermore, these Authors discuss the importance to better assess LUTS in patients undergoing hemodialysis, especially because no standard protocols for treating these symptoms are still available and there should be underestimations of their associated risks. In fact, it has to be underlined that many patients undergoing hemodialysis are elegible for kidney transplant and their dialytic time could be only transitory. Therefore, aiming to prevent significant complications after transplantation, lower urinary tract function must be assessed and functional alterations need to be corrected before surgery. Various Authors report LUTS, especially UTI and UI in renal tranplanted patients [13]. These Authors evidence functional alterations, particularly reduced bladder capacity and bladder compliance, during dialysis, and strongly recommend to adequately assess lower urinary tract function before kidney transplantation, even in asymptomatic patients, because symptoms could be understimated due to oliguria or anuria [13, 14] (Figure 2).
Conclusion
This study support the evidence that LUTS are higly represented in patients undergoing hemodialysis and UD show the prevalence of bladder alterations, especially reduced both capacity and compliance. Urinary symptoms should not be underestimated in these patients (due to oliguria or anuria) because they can be responsible for severe complications that can become a risk to life. Furthermore, the assessment of lower urinary tract function is very important in subjects elegible for kidney transplant aiming to prevent complications that can compromize the success of renal substitution. This research suffered some limitations, such as the type of population, represented only by caucasians, and the number of patients who underwent to UD. Multicenter and prospective protocols including patients after kidney transplantation could further support the importance of LUTS assessment in subjects undergoing hemodialysis.
References
-
Rosier PFWM, Schaefer W, Lose G, Goldman HB, Guralnick M, et al. (2017) International Continence Society Good Urodynamic Practices and Terms 2016: urodynamics, uroflowmetry, cystometry, and pressure-flow study. Neurourol Urodyn 36(5): 1243-1260.
-
Wu MY, Chang SJ, Hung SC, Chiang IN (2011) Lower Urinary Tract Symptoms are frequent in dialysis patients. Perit Dial Int 31(1): 99-102.
-
Zermann DH, Löffler U, Reichelt O, Wunderlich H, Wilhelm S, et al. (2003) Bladder dysfunction and end stage renal disease. Int Urol Nephrol 35(1): 93-97.
-
Scherberich JE, Fünfstück R, Naber KG (2021) Urinary tract infections in patients with renal insufficiency and dialysis – epidemiology, pathogenesis, clinical symptoms, diagnosis and treatment. GMS Infect Dis 9: 7.
-
Zazzeroni L, Pasquinelli G, Nanni E, Cremonini V, Rubbi I, et al. (2017) Comparison of Quality of Life in Patients Undergoing Hemodialysis and Peritoneal Dialysis: a Systematic Review and Meta-Analysis. Kidney Blood Press Res 42(4): 717-727.
-
Mitsui T, Shimoda N, Morita K, Tanaka H, Moriya K, et al. (2009) Lower urinary tract symptoms and their impact on quality of life after successfull renal transplantation. Int J Urol 16(4): 388-392.
-
Wu MY, Chang SJ, Hung SC, Chiang IN (2011) Lower urinary tract symptoms are frequent in dialysis patients. Perit Dial Int 31(1): 99-102.
-
El Nekidy WS, Mallat J, Nusair AR, Eshbair AH, Attallah N, et al. (2022) Urinary tract infections in hemodialysis patients-The controversy of antimicrobial drug urine concentrations. Hemodial Int 26(4): 548-554.
-
Wyndaele JJ (2012) Nocturia and quality of life. Eur Urol 61(1): 85-87.
-
Palleschi G, Pastore AL, Maggioni C, Fuschi A, Pacini L, et al. (2014) Overactive bladder in diabetes mellitus patients: a questionnaire based observational investigation. World J Urol 32(4): 1021-1025.
-
Hotta K, Miura M, Wada Y, Fukuzawa N, Iwami D, et al. (2017) Atrophic bladder in long-term dialysis patients increases the risk for urological complications after kidney transplantation. Int J Urol 24(4): 314-319.
-
Tsujimoto Y (1992) Morphological and physiological change in the dis-used bladder of hemodialysis patients. Nihon Hinyokika Gakkai Zasshi 83(11): 1852-1860.
-
Drouin S, Defortescu G, Prudhomme T, Culty T, Verhoest G, et al. (2021) Lower urinary tract symptoms and urinary incontinence in renal transplant recipients and candidates: The French guidelines from CTAFU. Prog Urol 31(1): 45-49.
-
Thuret R, Hurel S, Kleinclauss F, Timsit MO (2016) Lower urinary tract symptoms and pelvic floor dysfunction in renal transplant candidates and recipients. Prog Urol 26(15): 1114-1121.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report