Granulomatous Acute Interstitial Nephritis Revealing Multisystem Sarcoidosis Associated with Thyroiditis and Cushingoid Syndrome: Report of a Case and Review of the Literature
Introduction: Sarcoidosis can present with acute renal failure (ARF) due to granulomatous interstitial nephritis (GIN). We report the case of granulomatous acute renal failure (ARF) revealing multisystemic sarcoidosis in the nephrology department of the Aristide Le Dantec hospital in Dakar. Observation: Mrs. kD aged 54 with a past history of high blood pressure for 22 years, a multi nodular euthyroid goiter, referred to the nephrology department for impaired renal function. The clinical examination revealed at entry, deterioration in the general condition with weight loss and non-selective anorexia. Clinical anemia was also noted. The clinical examination also revealed Cushingoid syndrome and dry mouth syndrome. On biology, the blood count showed bicytopenia with anemia at 10.9 g/dl and leukopenia at 2620/mm3. There was an impairment of renal function with creatinine at 139.2 mg/l and blood urea at 1.76 g/l. The renal ultrasound became normal. Cervical ultrasound showed an aspect of abscessed thyroiditis of the right lobe. Chest computed tomography (CT) showed bilateral hilar adenomegaly and a band of bilateral basal linear atelectasis. The renal biopsy showed glomeruli of subnormal structure, the interstitium is riddled with tuberculoid follicles formed of epithelioid and multinucleated histiocytes of the Langhans type. The diagnosis of granulomatous acute interstitial nephritis revealing multisystemic sarcoidosis was kept. The evolution was favorable after 1 month of treatment with corticosteroid therapy with a clear improvement in renal function. Conclusion: Renal manifestations during sarcoidosis are rare. They can be indicative of the disease as in our patient. Renal biopsy is essential in any patient presenting with impaired renal function with extra-renal signs.
Introduction
Sarcoidosis is a multiorgan inflammatory disease of unknown cause, secondary to an uncontrolled immune response that can affect all organs. It is characterized anatomopathologically by the presence of epithelioid and gigantocellular granulomas without caseous necrosis [1]. Renal localization is the rarest among the visceral localizations of this disease. Disturbances of phosphocalcic metabolism are the most frequent abnormalities, and granulomatous tubulointerstitial nephritis represents the classic parenchymal involvement of sarcoidosis [1]. We report here the case of multisystem sarcoidosis revealed by granulomatous interstitial nephritis in a 54-year-old woman with thyroiditis and cushingoid syndrome.
Observation
Ms. K.D, aged 54, with a past history of high blood pressure known for 22 years poorly followed on amlodipine 5 mg and valsartan 160 mg per day, followed by a multi nodular euthyroid goiter and hyperuricemia on allopurinol 100 mg/day. She was referred to the nephrology department of Aristide le Dantec hospital for treatment of recently discovered impaired renal function.
On admission, examination revealed early postprandial vomiting without diarrhea or associated abdominal pain, at a rate of 3 to 4 episodes per day associated with chronic constipation without digital maneuver evolving intermittently for approximately 4 months. She also presented urinary signs such as pollakiuria at a rate of 6 urinations per day associated with burning in urination lasting ten (10) days before her admission. The patient also reported weight loss with an estimated weight loss of 5 kg in 1 month and non- selective anorexia. Blood pressure was 140/90 mm Hg, heart rate 103 beats/min, temperature 36°C, respiratocyclesry rate 22 /min. the body mass index (BMI) was 36.73 kg/ m2. Urine dipstick examination showed Proteinuria with 2 crosses (++), Hematuria with 0 crosses (-), Leukocyturia with 3 crosses (+++) and Nitrites with 2 crosses (++). The physical examination revealed a Cushingoid syndrome made up of facio-trunk obesity, amyotrophy (positive Tabouret and Foulard signs) and abdominal stretch marks; a dry mouth syndrome and a well-tolerated anemic syndrome without external bleeding. The remainder of the physical examination was normal.
Biologically, there was an alteration in renal function with serum creatinine at 139.2 mg/l and blood urea at 1.76 g/l. The blood ionogram showed hyponatremia at 130mmol/l and moderate hyperkalemia at 5.68 mmol/l. The blood count showed a slight hypochromic microcytic anemia with a hemoglobin level of 10.9g/dl, a leukopenia of 2620/ mm3 with a lymphopenia of 1770/mm3 and a neutropenia of 800/mm3. The platelet count was normal. The corrected serum calcium level showed hypercalcemia at 118 mg/l. We noted hyperphosphatemia at 80.5 mg and hypoalbuminemia at 25g/l.
Liver function was normal. Intact parathyroid hormone (PTHi) was 47 pg/ml. C-reactive protein (CRP) was 24 mg/l. The anti-ECT antibody assay was negative. Fasting blood sugar was 0.77 g/l. The angiotensin converting enzyme (ACE) dosage was elevated at 197IU/l. The aldosteronemia dosage was 330 pg. Reninemia was 5 (IU/l. Thyroid assessment showed an ultrasensitive TSH level at 0.799 IU/ml and free T4 at 13.12 pmol/l.
Serum protein electrophoresis showed a total protein level of 71.4g/L, albumin of 31.7g/L, globular alpha 1 of 3g/L; alpha 2 globular at 10.7g/L, beta 1 globular at 4.9g/L, beta 2 globular at 5.6g/L and gamma globular at 15.5g/L. In urine, calciuria was 102mg/24h and urinary free cortisol (UFC) was 19mg/24h (N= 30-200) and 24h proteinuria was 1g/24h. The cytobacteriological examination of urine was sterile.
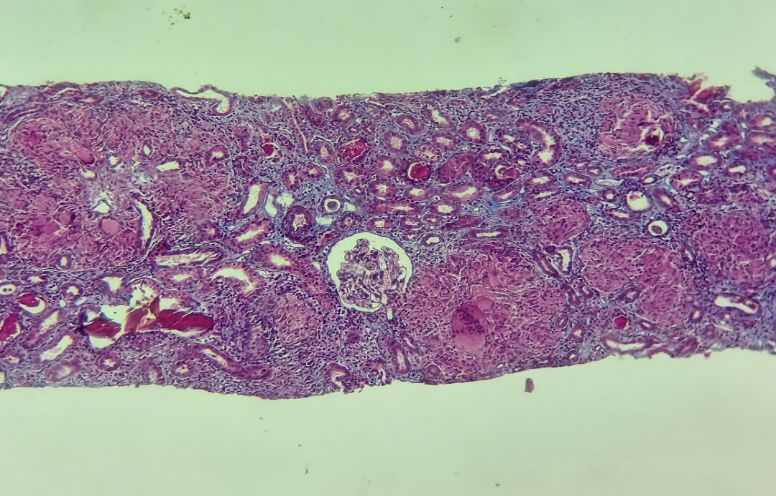
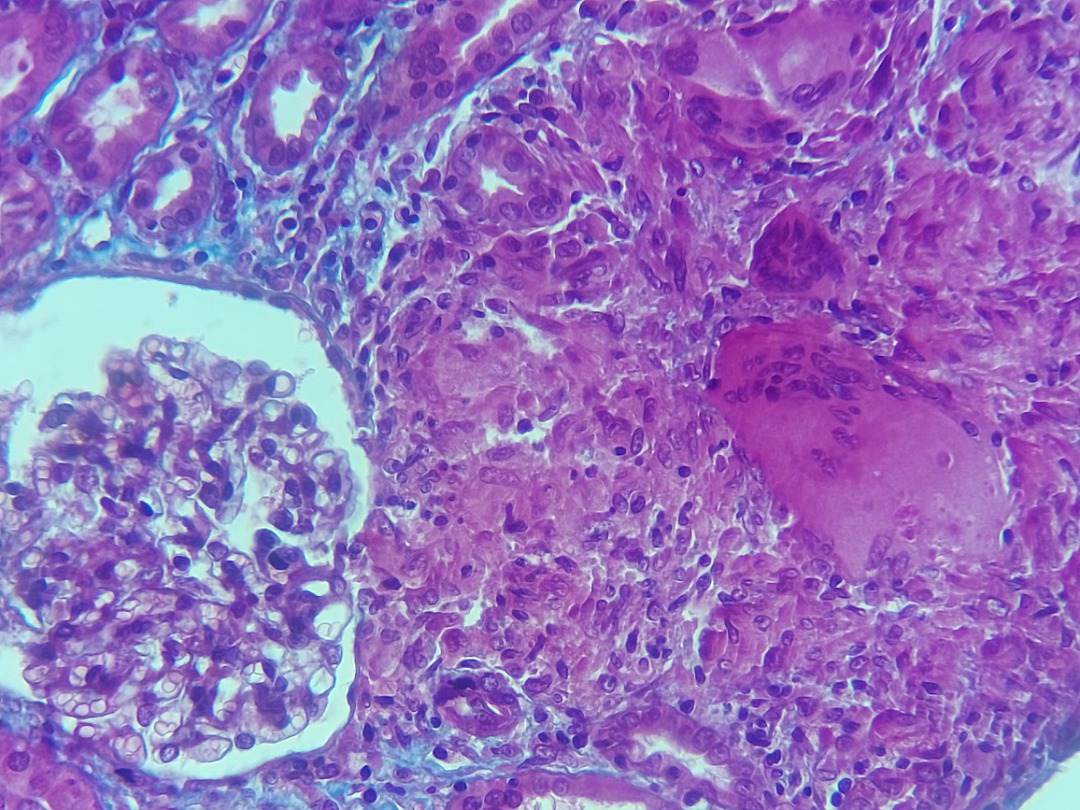
Morphologically, renal ultrasound showed kidneys of normal size (142.9mm on the right and 146.9mm on the left) with good cortico-medullary differentiation. Cervical ultrasound showed an appearance of abscessed thyroiditis of the right lobe. Chest computed tomography (CT) showed bilateral hilar, supracarinal and aortopulmonary window adenomegaly, a right scissural nodule and scissural micronodules and a band of bilateral basal linear atelectasis. Abdominal CT and brain CT were normal. The cardiac ultrasound was normal. Histologically, the renal biopsy (PBR) showed glomeruli of subnormal structure, the interstitium is riddled with tuberculoid follicles formed of epithelioid and multinucleated histiocytes of the Langhans type. These follicles are of variable size, often small and without necrosis except on one where there is central fibrinoid necrosis. These lesions have a tendency to converge diffusely. They destroy the tubules and repress the glomeruli. The residual tissue presents discreet fibrosis containing lymphoplasmocytes, slight arteriolar hyalinosis and discreet fibroproliferative endarteritis of the arcuate artery (Figures 1 & 2).
The diagnosis of systemic sarcoidosis with renal, pulmonary and lymph node localization associated with a non-toxic multi-nodular goiter, cushingoid syndrome was retained. The patient was put on 1 mg/kg/day of prednisone then dose reduction after 4 weeks, hydroxychloroquine 400 mg/day with adjuvant corticosteroid treatment.
The evolution was favorable marked by an improvement in symptoms, recovery of appetite and good improvement in renal function. The serum creatinine which was 139.2 mg/l increased to 21.71 mg/l in 1 month of treatment. The patient is followed regularly by nephrology.
Discussion
Sarcoidosis is a systemic disease of unknown etiology, predominantly affecting the respiratory system and lymphatic pathways, and characterized by the formation of immune granulomas in the affected organs [2]. The other most frequent visceral involvements are superficial lymph nodes, cutaneous and ophthalmological. Renal damage affects less than 10% of patients and usually occurs during multifocal sarcoidosis [3]. Sarcoidosis is associated with a broad spectrum of renal manifestations including hypercalcemia and hypercalciuria, granulomatous interstitial nephritis, glomerular damage, tubular dysfunction and obstructive uropathy [4]. Granulomatous vasculitis lesions are also rarely associated [5].
Histological diagnosis is not always easy in our practices, especially in semi-urban Senegalese and African environments in general. However, a case of diagnostic error was published in 2020 in Ziguinchor and concerned facial tuberculosis with dual nasopharyngeal and nasal sinus locations considered to be a malignant tumor and histology made the diagnosis [6]. Granulomatous tubulointerstitial nephritis (GTIN) is a rare histological diagnosis found in 0.5–0.9% of native renal biopsies [4] but is the most common histological lesion in renal sarcoidosis. Pathologically, the basic lesions consist of an interstitial cellular infiltrate and tubular inflammation. The presence of granulomas is not systematic. They were reported in 13 of 17 patients in Rajakariar’s series [7], and in 37 of 47 patients in Mahevas’s [3]. Interstitial fibrosis was present in 100% of cases in these two series [4, 7], demonstrating the particularly profibrotic nature of this nephropathy. A diagnostic delay is also very likely, especially since renal failure is minimally symptomatic. In our case, the cellular form was found and the fibrosis was minimal, which constitutes an element of good prognosis in our patient. The presentation of sarcoidosis with acute renal failure is rare [5].
Sarcoid GTIN is symptomatic in 0.7 to 4.3% of patients [4], when symptomatic, the mode of presentation is usually acute impairment of renal function [4, 7]. The pathological mechanism contributing to GTIN ARF in sarcoidosis is thought to be non-caseating granulomatous inflammation, composed of a central follicle of macrophages, epitheloid cells and multinucleated giant cells [8, 9].
Renal failure can complicate known sarcoidosis or be indicative of the disease [10]. The diagnosis is difficult in cases of initial renal damage. The search for an associated extra renal location, in particular mediastino-pulmonary, helps to establish the diagnosis. In our patient, the discovery of an alteration in renal function associated with hypercalcemia and an increase in ACE led to the diagnosis of renal sarcoidosis which was confirmed by the renal biopsy which showed severe tuberculoid granulomatous nephritis evoking the diagnosis of sarcoidosis in its cellular form. The search for extra renal localization of sarcoidosis made it possible to discover an asymptomatic mediastino- pulmonary localization.
The diagnosis of sarcoidosis is a diagnosis of exclusion [11]. ACE is elevated in most cases, but is nonspecific. It is produced by epithelioid cells, giant cells and macrophages and can be elevated in other granulomatoses [5]. In sarcoidosis as in other granulomatoses (Crohn’s disease, mycobacterial infections, certain lymphomas, etc.), calcitriol is produced in excess. Unlike renal 1-alpha-hydroxylase activity, 1-alpha-hydroxylase activity of macrophage origin is neither regulated by hypercalcemia nor by negative feedback of hypercalcitriolemia, which promotes intestinal absorption. of calcium and is responsible for hypercalcemia [1]. Urinary manifestations, the most common of which are aseptic pyuria and microscopic hematuria, are non-specific. Hypercalciuria is common in sarcoidosis and constitutes an element of consolidation of the diagnosis as is the case in our patient. Therefore, the diagnosis of sarcoidosis requires typical histological evidence in at least one affected organ [12].
In our patient, the presence of Cushingoid syndrome suggested a probable association of multisystem sarcoidosis with Cushing’s syndrome, but the investigations made it possible to eliminate it on the basis of the urinary free cortisol and 24-hour creatinuria ratio. Thyroid explorations carried out in front of the goiter led to the conclusion of a euthyroid goiter.
As in pulmonary sarcoidosis, glucocorticoids are the cornerstone in the treatment of renal sarcoidosis. Several retrospective studies have shown that treatment with prednisone of 0.5 to 1 mg/kg, with dose escalation over 6 to 12 months up to low-dose maintenance treatment of 5 mg/ day, allows for ‘significantly improve renal function [3, 7]. In our patient, a considerable recovery of renal function was obtained after 01 months with a dose of 1 mg/Kg/day. The favorable response to corticosteroid treatment observed in our patient constitutes an argument in favor of renal sarcoidosis as observed in other similar cases. In the cases of Sapre C and Alangari FS, all patients achieved normalization of renal function, normal serum calcium and improvement in clinical signs after 12 months of treatment [13, 14].
Our patient is currently continuing his follow-up in nephrology, endocrinology and otorhinolaryngology (ENT) for the treatment of his euthyroid goiter.
Conclusion
This observation illustrates the diversity of clinical forms of sarcoidosis. ARF due to acute interstitial nephritis outside of the infectious and immuno-allergic context should suggest a systemic origin, particularly sarcoidosis. Imagery is a tool to help with topographical diagnosis. Histology allows the diagnosis, hence the interest in performing a kidney biopsy in any patient presenting an alteration of function with extra- renal signs.
References
-
Stehlé T, Boffa JJ, Lang P, Desvaux D, Sahali D, et al. (2013) Kidney involvement in sarcoidosis. Rev Med Int 34(9): 538‑544.
-
Sadek BH, Sqalli Z, Al Hamany Z, Benamar L, Bayahia R, et al. (2011) Renal failure during sarcoidosis. Rev Pneum Clin 67(6): 342‑346.
-
(2007) Mahevas Mrenal damage during sarcoidosis, multicenter retrospective study of 47 observations.
-
Hilderson I, Van Laecke S, Wauters A, Donck J (2014) Treatment of renal sarcoidosis: is there a guideline? Overview of the different treatment options. Nephrol Dial Transplant 29(10): 1841‑1847.
-
Agrawal V, Crisi GM, D’Agati VD, Freda BJ (2012) Renal sarcoidosis presenting as acute kidney injury with granulomatous interstitial nephritis and vasculitis. American Journal of Kidney Diseases 59(2): 303‑308.
-
Ndadi TKJ, Fabrice S, Yaya K (2020) Facial tuberculosis with dual localization: nasopharyngeal and nasal sinus: report of a case. Health Sci Dis 21(9): 113-116.
-
Rajakariar R, Sharples EJ, Raftery MJ, Sheaff M, Yaqoob MM (2006) Sarcoid tubulointerstitial nephritis: long- term outcome and response to corticosteroid therapy. Kidney Int 70(1): 165‑169.
-
Manjunath V, Moeckel G, Dahl NK (2013) Acute kidney injury in a patient with sarcoidosis: hypercalciuria and hypercalcemia leading to calcium phosphate deposition. Clin Nephrol 80(2): 151‑155.
-
Kobak S (2015) Sarcoidosis: a rheumatologist’s perspective. Therapeutic advances in musculoskeletal disease 7(5): 196-205.
-
Hawrot-Kawecka A, Kawecki G, Dulawa J (2008) Acute renal failure as the first extrapulmonary presentation of sarcoidosis. Inter Med 47(24): 2201-2201.
-
Agrawal V, Kaul A, Prasad N, Sharma K, Agarwal V (2015) Etiological diagnosis of granulomatous tubulointerstitial nephritis in the tropics. Clin kidney J 8(5): 524‑530.
-
Hutchinson J (1999) Statement on sarcoidosis. joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ER. Am J Respir Crit Care Med 160(2): 736-755.
-
Sapre C, Kolla PK, Rao KV, Sadineni R, Reddy B, et al. (2020) A rare case of sarcoidosis causing granulomatous interstitial nephritis presenting as non-oliguric acute renal failure in the Indian subcontinent. Saudi J Kidney Dis Transpl 31(2): 549-552.
-
Alangari FS, Binsalih SA, Heijani B, Aloudah N (2020) Granulomatous Interstitial Nephritis Due to Renal- limited Sarcoidosis. Saudi J Kidney Dis Transpl 31(4): 856-859.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report