Emphysematous Pyelonephritis: A Comprehensive Review
Emphysematous pyelonephritis (EPN) is a severe necrotizing infection of the renal parenchyma, characterized by gas within the kidney tissues, predominantly affecting diabetic individuals. We present a comprehensive review of EPN, encompassing its epidemiology, clinical presentation, diagnosis, and management strategies. Despite its rarity, EPN poses significant clinical challenges due to its potential for rapid progression and life-threatening complications. Prompt diagnosis facilitated by advanced imaging modalities and multidisciplinary management approaches are essential for optimizing patient outcomes. Through this review, we aim to enhance understanding and highlight the importance of early recognition and tailored interventions in the management of EPN.
Introduction
Emphysematous pyelonephritis (EPN) is an acute, severe necrotizing infection of the renal parenchyma and surrounding tissues, characterized by the presence of gas within the kidney tissues [1]. This condition predominantly affects individuals with diabetes, with an overwhelming 95% of cases occurring in diabetic patients, presenting a notable male-to-female ratio of 1:6 [1, 2]. Clinical manifestations mimic those of severe, acute pyelonephritis, including symptoms such as fevers, chills, flank or abdominal pain, nausea, and vomiting. The onset of symptoms may vary from abrupt to gradual over two to three weeks. EPN poses a serious and potentially fatal clinical trajectory if not promptly identified and managed. Diagnostic imaging, such as plain radiographs, ultrasound scans, or computed tomography, plays a crucial role in confirming the diagnosis, with gas shadows seen in the renal areas raising suspicion. Escherichia coli is the most commonly isolated pathogen, accounting for nearly 70% of reported cases. While EPN primarily occurs in diabetics, cases in non-diabetic patients are rare but noteworthy. Despite its rarity, a structured approach to image interpretation and holistic management of critically unwell patients are crucial. Additionally, urinary tract obstructions and immunosuppression are predisposing factors. Treatment approaches vary, ranging from aggressive medical and interventionist strategies to conservative management, with outcomes showing considerable variability in mortality rates. This report integrates diverse clinical perspectives and highlights the necessity for a comprehensive understanding and management of EPN.
A 27-year-old previously healthy woman presented to the emergency department with a two-week history of anorexia, loss of appetite, and worsening right low back pain radiating to the right flank, which had exacerbated over the preceding four days along with the onset of fever. Notably, the patient had no significant medical history, was not known to be diabetic, and had not undergone any prior surgeries.
On examination, she was febrile with a temperature of 38.4°C, tachycardic with a heart rate of 100 beats/ min, and normotensive with a blood pressure of 110/60 mmHg. Physical examination revealed swelling, warmth, and tenderness in the right lumbar region. Laboratory investigations revealed findings consistent with a severe systemic inflammatory response, including microcytic hypochromic anaemia (Hb: 4.20 g/dl), hyperleukocytosis (white blood cell count of 32,500/mm^3), thrombocytosis (platelet count of 1,190,000/mm^3), significantly elevated C-reactive protein (496 mg/l), and elevated creatinine (17.6 mg/l).
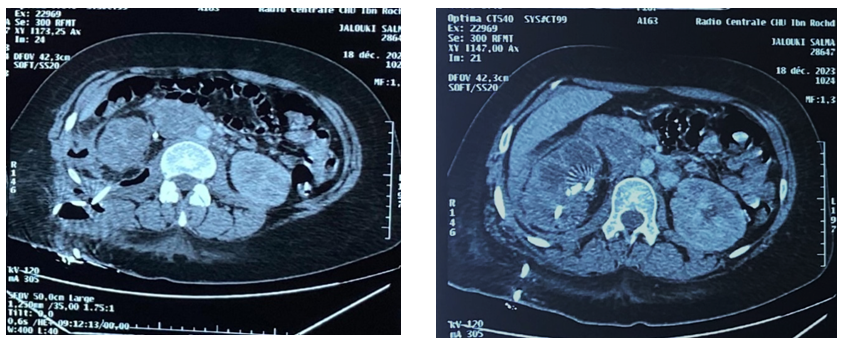
An abdomino-pelvic CT scan demonstrated emphysematous pyelonephritis Class 3B on the right side, accompanied by a 31x19x8mm pyelic lithiasis with a density of 360 HU, complicated by multiple right retroperitoneal collections (Figures 1 & 2).
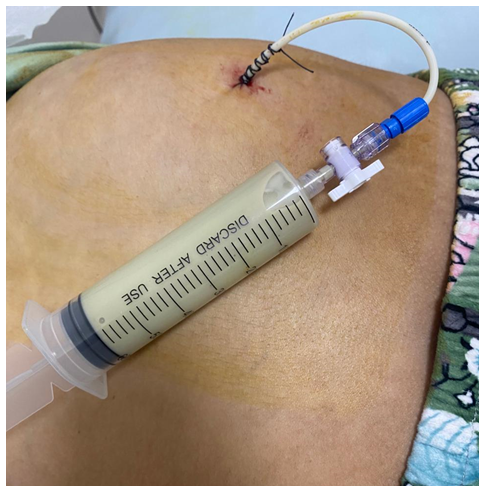
Prompt initiation of empirical antibiotic therapy with Ceftriaxone, gentamicin, and metronidazole was followed by percutaneous drainage and a discharge incision, yielding over 2 liters of frank greenish pus. Subsequent placement of a double-J stent and continuation of antibiotics for two weeks constituted the management strategy during the hospitalization. After one month, a scintigraphy was performed, revealing non-functional involvement of the affected kidney. Nephrectomy was carried out in the patient two months after her acute episode, with uncomplicated postoperative recovery.
Discussion
Emphysematous pyelonephritis (EPN) presents a unique challenge in the realm of renal pathology, characterized by its insidious progression and potential for life-threatening complications. Our exploration into this complex condition sheds light on the intricate interplay of factors contributing to its pathogenesis, clinical presentation, diagnosis, and management.
First and foremost, our findings underscore the multifactorial nature of EPN etiology. While traditionally associated with diabetes mellitus [3], we delve deeper into the landscape of predisposing factors, unraveling the roles of obstructive uropathy, hypertension, and geographical distribution, particularly prevalent in regions like Asia [4]. These insights not only broaden our understanding but also pave the way for more targeted preventive strategies tailored to high-risk populations.
In parallel, our discussion delves into the diagnostic challenges posed by EPN. Despite advancements in imaging modalities such as ultrasonography and computed tomography [5], the nonspecific nature of symptoms often obscures early detection. We emphasize the importance of a high index of suspicion, particularly in patients presenting with fever, flank pain, and altered mental status, to facilitate timely intervention and improve outcomes.
Moreover, our analysis sheds light on the evolving landscape of EPN management. Historically dominated by emergent nephrectomy [5, 6], contemporary approaches favor a multidisciplinary paradigm encompassing antibiotic therapy, drainage procedures, and supportive care. This shift towards less invasive interventions underscores the importance of individualized treatment strategies tailored to patient-specific factors and disease severity. As we navigate the intricacies of EPN, our study serves as a catalyst for further research and innovation in this field. By elucidating the underlying mechanisms, refining diagnostic algorithms, and optimizing therapeutic approaches, we endeavor to enhance patient outcomes and mitigate the burden of this formidable renal infection.
In conclusion, our discussion encapsulates the dynamic landscape of EPN, weaving together insights from epidemiology, pathophysiology, clinical practice, and therapeutic interventions. Through collaborative efforts and a comprehensive understanding of the disease process, we aim to forge new frontiers in EPN management and ultimately improve patient care.
References
-
Laila N, Chan Y (2013) Emphysematous pyelonephritis- case report and literature review. Pathology 45: S73.
-
Rafailidis V, Karamidou V, Liouliakis G, Kougioumtzoglou D (2013) Ephysematous pyelonephritis: a case report. Hippokratia 17(4): 373-375.
-
Arrambide-Herrera JG, Robles-Torres JI, Ocaña-Munguía MA, Romero-Mata R, Gutiérrez-González A, et al. (2022) Predictive factors for mortality and intensive care unit admission in patients with emphysematous pyelonephritis: 5-year experience in a tertiary care hospital. Actas Urol Esp Engl Ed 46(2): 98-105.
-
Karthikeyan VS, Manohar CMS, Mallya A, Keshavamurthy R, Kamath AJ, et al. (2018) Clinical profile and successful outcomes of conservative and minimally invasive treatment of emphysematous pyelonephritis. Central European Journal of Urology 71(2): 228-233.
-
Wu SY, Yang SS, Chang SJ, Hsu CK (2022) Emphysematous pyelonephritis: classification, management and prognosis. Tzu Chi Medical Journal 34(3): 297-302.
-
Somani BK, Nabi G, Thorpe P, Hussey J, Cook J, et al. (2008) Is percutaneous drainage the new gold standard in the management of emphysematous pyelonephritis? Evidence from a systematic review. The Journal of Urology 179(5): 1844-1849.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report